
| 📌 The essentials On May 21, 2026, the FDA approved Linzess (linaclotide 72 mcg, Ironwood Pharmaceuticals/AbbVie) for functional constipation in pediatric patients aged 2 years and older. This expands Linzess’s prior pediatric FC approval (ages 6 and older, approved 2023) to now include children ages 2 to 5 years. Linzess remains the only FDA-approved prescription therapy for pediatric functional constipation. Clinical basis: a Phase 3 randomized, placebo-controlled, double-blind 12-week trial in patients aged 2 to 5 years with functional constipation, showing that linaclotide 72 mcg significantly increased spontaneous bowel movements versus placebo with a consistent safety profile. This approval was supported by efficacy data from the earlier Phase 3 trial in children aged 6 to 17 years published in The Lancet Gastroenterology and Hepatology. Complete Linzess pediatric FC indication: ages 2 to 17 years, 72 mcg once daily. Critical safety warning: Linzess is contraindicated in patients under 2 years of age due to the risk of serious dehydration based on neonatal animal data. This age floor is absolute. The most common adverse event in pediatric patients is diarrhea. Severe diarrhea requires discontinuation and rehydration. Linzess is not a laxative and should not be used in patients with known or suspected mechanical gastrointestinal obstruction. |
|---|
Functional constipation in children is one of the most common complaints seen in pediatric primary care and pediatric gastroenterology. It accounts for approximately 25% of all pediatric gastroenterology visits and up to 5% of all general pediatric office visits in the United States. For a condition that affects millions of children, the treatment options have been remarkably limited: behavioral and dietary interventions, over-the-counter osmotic laxatives like polyethylene glycol (MiraLAX), and in more refractory cases, office-based and specialist-managed regimens that still often fall short.
Until 2023, there was no FDA-approved prescription drug specifically for functional constipation in children. That changed when linaclotide was approved for children aged 6 to 17 years. On May 21, 2026, the FDA extended that approval to children as young as 2, supported by a Phase 3 trial specifically designed and conducted in the 2-to-5 age group.
This post covers what functional constipation is in children, how linaclotide works, what the evidence shows for the 2-to-5 age group, how to administer the drug in young children, and what the critical safety considerations are for parents and clinicians.
What Functional Constipation Is and Why Young Children Are Particularly Affected
Functional constipation is a clinical diagnosis based on symptoms rather than a structural or metabolic cause. In the pediatric population, it is defined using Rome IV criteria as the presence of at least two of the following symptoms over at least one month, without evidence of organic pathology:
- Fewer than 3 spontaneous defecations per week
- History of excessive stool retention or fecal withholding
- History of painful or hard bowel movements
- History of large-diameter stools that may obstruct the toilet
- Presence of a large fecal mass in the rectum on examination
The estimated worldwide prevalence in preschool-aged children is approximately 3%, though regional variation is substantial and the true prevalence may be higher given that many cases are managed at home without clinical contact. In the United States, functional constipation affects an estimated 1 in 20 young children at any given time.
Why the 2-to-5 age group is particularly vulnerable
Preschool-aged children are at elevated risk for functional constipation for several physiological and behavioral reasons. Toilet training is a common precipitant: the transition from diapers to toilet use can trigger withholding behaviors, particularly if a child associates the toilet with discomfort or anxiety. Any painful stool passage creates a cycle: pain leads to withholding, withholding leads to harder and larger stools, larger stools cause more pain on passage, which reinforces withholding further.
Dietary transitions in this age group, including the shift to family foods, weaning from breast milk, and inconsistent fiber intake, also contribute. Limited communication ability in younger children means parents often underestimate the degree of discomfort or may not recognize withholding behaviors for what they are.
Untreated functional constipation in young children has real consequences beyond discomfort. Chronic fecal retention can lead to fecal impaction, which may require emergency intervention. Encopresis (overflow fecal incontinence) can develop and carries significant social and psychological consequences for school-aged children. The earlier effective treatment is initiated, the lower the risk of this cascade.
| What the Rome IV criteria mean in practice for ages 2 to 5 For the youngest patients covered by the expanded Linzess indication, the Rome IV criteria for toddlers and preschoolers specifically recognize behaviors that are not always recognized as constipation by parents. Fecal withholding, in which a child deliberately tightens pelvic floor muscles and assumes characteristic postures to prevent defecation, is one of the most common presentations. Parents often mistake withholding postures for straining. The assessment of whether stools are hard, the frequency of natural bowel movements, and the presence of pain should all be evaluated in context of the child’s developmental stage, dietary history, and any identifiable precipitants. Organic causes of constipation in this age group that must be excluded before a functional diagnosis is made include Hirschsprung’s disease (rare but important), hypothyroidism, celiac disease, and anatomical abnormalities. A thorough evaluation by the pediatrician or pediatric gastroenterologist before initiating prescription therapy is appropriate. |
|---|
How Linzess Works: The GC-C Mechanism
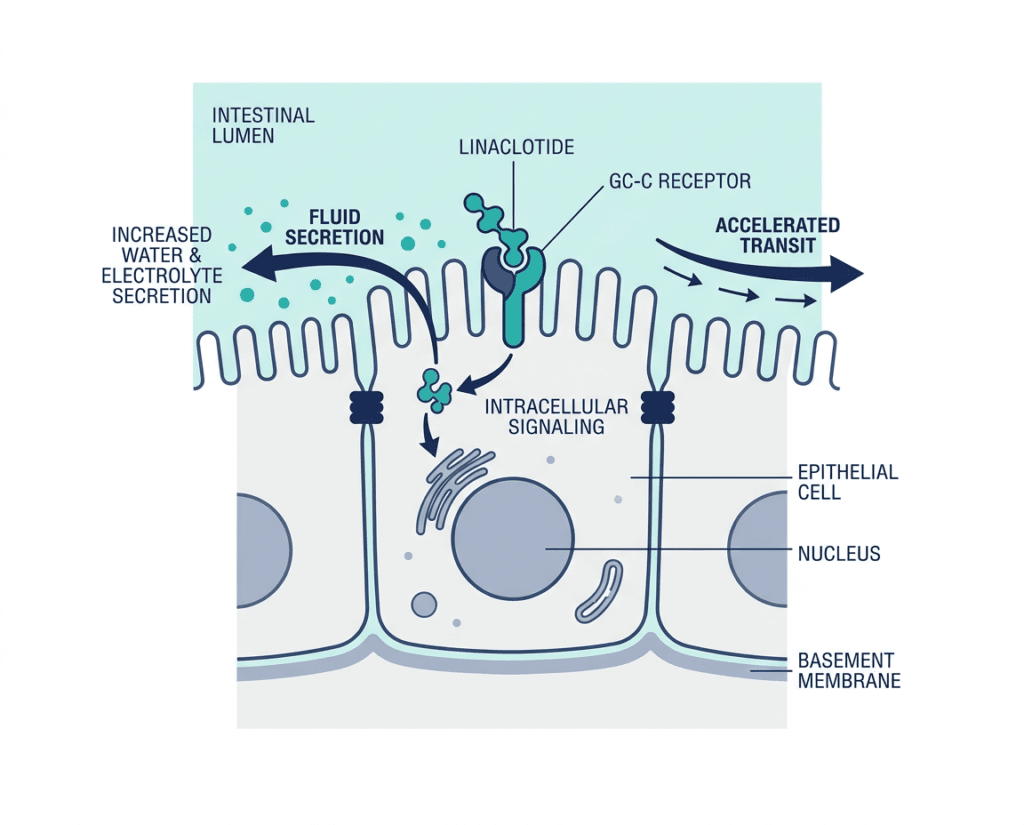
Linaclotide is a guanylate cyclase-C (GC-C) agonist. It is a 14-amino-acid peptide structurally similar to endogenous GC-C-activating peptides (guanylin and uroguanylin) that are produced naturally by intestinal epithelial cells.
When linaclotide binds to GC-C receptors on the luminal surface of intestinal epithelial cells, it activates a signaling cascade that produces cyclic GMP (cGMP) inside those cells. Elevated intracellular cGMP activates a chloride and bicarbonate channel (CFTR) in the intestinal epithelium, which secretes fluid into the intestinal lumen. The resulting increase in luminal fluid content softens stool and accelerates intestinal transit.
Locally elevated cGMP also activates pathways that reduce the activity of pain-sensing nerve fibers in the intestinal wall. This visceral analgesic effect is believed to contribute to reduced abdominal discomfort and pain associated with constipation, though the clinical relevance of this mechanism in pediatric patients has not been specifically established.
Critically, linaclotide acts almost entirely in the gut. Systemic absorption is minimal: the drug is not measurably detected in the bloodstream at therapeutic doses. This limited absorption is one reason the pediatric side effect profile is favorable compared to systemically acting drugs.
The Pediatric Evidence Base: What the Trials Showed
Linzess’s expanded approval for ages 2 to 5 years builds on a pediatric evidence program that has been developed over several years.
Phase 3 trial in children aged 6 to 17 (the foundational pediatric trial)
The original pediatric FC indication (ages 6 to 17) was supported by data from Trial 7 (NCT04026113), a 12-week, double-blind, placebo-controlled, randomized, multicenter Phase 3 trial in 328 children aged 6 to 17 years meeting modified Rome III criteria for functional constipation, published in The Lancet Gastroenterology and Hepatology.
Key results from Trial 7:
| Outcome | Linaclotide 72 mcg | Placebo |
|---|---|---|
| Spontaneous bowel movement frequency rate | Significantly higher | Reference |
| Patients with at least 1 SBM within 24 hours of first dose | 30.5% | 20.7% (p=0.043) |
| Patients with at least 1 SBM within 48 hours of first dose | 56.7% | 38.4% (p=0.0009) |
| Most common adverse event (diarrhea) | 4% (7 of 164) | Lower rate |
| Safety vs. adults | Consistent profile | — |
Phase 3 trial in children aged 2 to 5 (the basis for the May 2026 expansion)
The May 2026 approval for ages 2 to 5 was based on a Phase 3, 12-week, randomized, placebo-controlled trial specifically designed for this younger age group. This trial evaluated linaclotide 72 mcg in children aged 2 to 5 years with functional constipation, demonstrating that the drug significantly increased spontaneous bowel movements versus placebo with a consistent safety profile in this age range.
The trial specifically confirmed that the mechanism is active in this age group: GC-C intestinal expression in children aged 2 to less than 18 years was examined in a clinical study and showed no age-dependent trend, providing the biological rationale for why the same dose produces consistent effects across the 2-to-17 age range. Below age 2, insufficient data on GC-C expression precludes safe use, which is the basis for the absolute age-2 lower limit.
Both the pediatric 6-to-17 trial and the new 2-to-5 trial data are also supported by efficacy extrapolation from robust adult trials in chronic idiopathic constipation, providing multiple layers of evidence that the mechanism operates consistently.
The Full Linzess Pediatric Approval Picture: A Rapidly Expanding Label
The May 2026 approval is the most recent in a series of pediatric Linzess approvals that have expanded its use substantially since the original 2012 adult approval:
| Indication | Population | Approval date |
|---|---|---|
| Chronic idiopathic constipation (CIC) | Adults | August 2012 |
| Irritable bowel syndrome with constipation (IBS-C) | Adults | August 2012 |
| Functional constipation (FC) | Pediatric patients aged 6 to 17 years | September 2023 |
| IBS-C | Pediatric patients aged 7 years and older | November 2025 |
| Functional constipation (FC) expanded | Pediatric patients aged 2 years and older | May 21, 2026 |
Linzess is now the only FDA-approved prescription drug for functional constipation in children from age 2 through age 17. It is also the first and only FDA-approved prescription therapy for IBS-C in children aged 7 and older.
Dosing and Administration
Recommended dose for all pediatric FC patients (ages 2 to 17): Linaclotide 72 mcg orally once daily.
Timing: On an empty stomach, at least 30 minutes before the first meal of the day.
Administration in young children (ages 2 to 5): Young children cannot swallow capsules whole. The capsule contents can be administered in two ways, as outlined in the prescribing information:
- With applesauce: Open the capsule, sprinkle the contents onto one teaspoon of room-temperature applesauce, and have the child swallow the mixture immediately without chewing. Do not store the mixture.
- With water: Open the capsule, pour the contents into a clean cup containing approximately 1 teaspoon (about 5 mL) of room-temperature water, gently swirl for approximately 20 seconds, and have the child swallow the mixture immediately. Do not store the mixture.
Do not administer by crushing or dissolving the capsule itself. Do not add the contents to infant formula, breast milk, or beverages other than water.
If a dose is missed: Take it as soon as possible on the same day. If that day has passed, skip the missed dose and resume the next day. Do not double up.
Duration of therapy: The appropriate treatment duration should be determined by the prescribing clinician based on treatment response and the child’s clinical course. Functional constipation in young children can be a chronic, relapsing condition, and ongoing therapy may be appropriate in some children after other management strategies have been optimized.
Safety: What Parents and Clinicians Need to Know
Contraindication in patients under 2 years of age
Linzess is absolutely contraindicated in patients younger than 2 years. In neonatal mouse studies, linaclotide caused increased fluid secretion through age-dependent elevated GC-C activity, which led to rapid and fatal dehydration. The 2-year minimum age reflects the human biological evidence that GC-C receptor expression does not show the same age-dependent elevation pattern in children 2 years and older, but insufficient data exists for those under 2 to confirm equivalent safety.
This is not a soft guideline. It is an absolute contraindication with an FDA boxed-equivalent warning.
Diarrhea: the most important adverse event to monitor
Diarrhea is the most commonly reported adverse reaction in both adult and pediatric clinical trials. In the pediatric 6-to-17 trial (Trial 7), diarrhea occurred in 4% of linaclotide-treated patients compared with lower rates in the placebo arm. In younger children, dehydration risk from diarrhea is proportionally higher than in older patients because of lower total body water reserves.
What to do if diarrhea occurs:
- Mild diarrhea: monitor hydration closely; ensure the child is drinking fluids
- Severe diarrhea: discontinue Linzess immediately and ensure adequate rehydration; contact the prescribing clinician
Parents should be counseled specifically about diarrhea recognition and the dehydration signs in young children before starting therapy: decreased urine output, dry mucous membranes, reduced tears, and decreased activity level are clinical indicators of dehydration requiring medical evaluation.
Mechanical obstruction: do not use in obstruction
Linzess is contraindicated in patients with known or suspected mechanical gastrointestinal obstruction. All patients should be evaluated for structural causes of constipation before initiating therapy.
Systemic absorption: minimal
Because linaclotide is minimally absorbed into the bloodstream, it does not produce systemic drug effects at therapeutic doses. The safety profile reflects predominantly local GI effects rather than systemic medication reactions.
What This Means for Parents Navigating Functional Constipation in a Young Child
When to consider discussing Linzess with your pediatrician
Linzess is a prescription medication intended for children with functional constipation who have not responded adequately to dietary and behavioral interventions and to over-the-counter laxative therapy (such as polyethylene glycol). It is not a first-line treatment for all constipation in young children, and most children will begin with simpler, less intensive approaches.
A conversation about Linzess is appropriate when:
- Your child ages 2 to 5 has been diagnosed with functional constipation by a pediatrician or pediatric gastroenterologist
- You have tried dietary modification (increased fluid and fiber intake), toilet training adjustments, and at least one course of over-the-counter osmotic laxative therapy
- Constipation continues to affect your child’s quality of life, comfort, or daily functioning despite these approaches
- Your pediatrician has excluded organic causes of constipation appropriate to your child’s age
How to administer to a toddler or preschooler
The applesauce administration method is typically easiest for most children ages 2 to 5. The granules from the capsule are nearly tasteless, and mixing them into a small amount of applesauce is usually well-accepted. If your child does not tolerate applesauce, the water slurry method is available. Consistency in daily timing (before breakfast each morning) helps establish the routine.
What to watch for during the first weeks of therapy
In the first 1 to 4 weeks, parents should monitor for:
- Improvement in bowel movement frequency and stool consistency (the expected benefit)
- Diarrhea or loose stools (the most common side effect; mild cases may not require stopping the drug)
- Signs of dehydration if diarrhea occurs (reduced wet diapers or urination, dry mouth, no tears when crying, unusual lethargy)
- Worsening of abdominal discomfort or new symptoms that were not present before starting
Keep your pediatrician informed of the response within the first 4 weeks. If your child has not shown improvement in spontaneous bowel movement frequency and stool consistency after a reasonable trial period, discuss with your provider whether continuing therapy is appropriate.
For related HED coverage of gastrointestinal health and gut-targeted drug approvals, see our post on Lynavoy (linerixibat) for cholestatic pruritus in primary biliary cholangitis, which covers another gut-targeted therapy approval, and our post on the Fasenra approval for hypereosinophilic syndrome as an example of how rare condition approvals are expanding across pediatric populations in 2026.
Sources
FDA approval announcement: FDA Approves Use of LINZESS (linaclotide) in Pediatric Patients Two Years of Age and Older with Functional Constipation (FC). FDA.gov. May 21, 2026.
Ironwood Pharmaceuticals press release: FDA Approves Use of LINZESS (linaclotide) in Pediatric Patients Two Years of Age and Older with Functional Constipation. investor.ironwoodpharma.com. May 27, 2026.
BioSpace press release: FDA Approves Use of LINZESS (linaclotide) in Pediatric Patients Two Years of Age and Older with Functional Constipation. biospace.com. May 2026.
Drugs.com approval news: FDA Approves Linzess (linaclotide) in Pediatric Patients Two Years of Age and Older with Functional Constipation. drugs.com. May 2026.
HCPLive clinical coverage: FDA Approves Linaclotide (Linzess) for Functional Constipation in Patients 2 Years and Older. hcplive.com. May 2026.
Conexiant/Pediatrics clinical news: FDA OKs Linaclotide in Young Children. conexiant.com. May 2026.
Phase 3 Trial 7 primary publication (Lancet GH): Di Lorenzo C, Khlevner J, Rodriguez-Araujo G, et al. Efficacy and safety of linaclotide in treating functional constipation in paediatric patients: a randomised, double-blind, placebo-controlled, multicentre, phase 3 trial. The Lancet Gastroenterology and Hepatology. 2023. doi:10.1016/S2468-1253(23)00396-8.
Trial 7 registration: NCT04026113. ClinicalTrials.gov.
FDA first pediatric FC approval press release (September 2023): FDA Approves First Treatment for Pediatric Functional Constipation. FDA.gov. September 2023.
FDA pediatric IBS-C approval (November 2025): FDA Approves First Drug for Children 7 Years and Older with Irritable Bowel Syndrome with Constipation. FDA.gov. November 2025.
Linzess prescribing information: LINZESS (linaclotide) Prescribing Information. Ironwood Pharmaceuticals/AbbVie. Updated 2026.
Functional constipation in children (NIDDK): Constipation in Children. niddk.nih.gov.
Functional constipation StatPearls: Functional Constipation. StatPearls. NCBI.
Linaclotide mechanism: Linaclotide. StatPearls. NCBI.
GC-C receptor biology: Guanylate Cyclase-C in GI Tract. PMC4415491.
Patient resources: North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) | NIDDK Constipation in Children | Linzess patient resources
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Linzess (linaclotide) is a prescription medication. Decisions about treatment for pediatric functional constipation, including the appropriateness of prescription therapy, should be made in consultation with a qualified pediatrician or pediatric gastroenterologist. Do not administer Linzess to children under 2 years of age. |
|---|