| 📌 The essentials On July 7, 2026, the FDA granted accelerated approval to Trutakna (atacicept-vymj, Vera Therapeutics) to reduce proteinuria in adults with primary IgA nephropathy (IgAN) at risk for disease progression. Trutakna is a recombinant fusion protein that simultaneously inhibits both B-cell activating factor (BAFF) and A proliferation-inducing ligand (APRIL), two cytokines that drive the B-cell activity responsible for producing the abnormal IgA antibodies that cause this disease. It is the first and only FDA-approved therapy to block both BAFF and APRIL, making it mechanistically distinct from every other approved IgAN therapy. It is the sixth drug approved for IgAN in the United States, joining Tarpeyo (budesonide EC, Calliditas, 2021), Filspari (sparsentan, Travere, 2023), Voyxact/Fabhalta (iptacopan, Novartis, 2024), Vanrafia (atrasentan, Otsuka, 2024), and Kinpeygo (budesonide, released outside U.S.). Administration: 150 mg subcutaneous injection once weekly, self-administered by the patient at home using a pre-filled autoinjector. No infusion center required. The clinical basis: prespecified 36-week interim analysis of the ongoing Phase 3 ORIGIN 3 trial (NCT04716231), enrolling 431 adults with biopsy-confirmed IgAN. Analysis population: first 203 participants who received at least 1 dose. Primary endpoint: change in 24-hour urine protein-to-creatinine ratio (UPCR) compared to placebo at 36 weeks. Results: 46% reduction from baseline in UPCR (atacicept arm); 42% reduction versus placebo (p less than 0.0001). Important caveat: this is an accelerated approval based on reduction of proteinuria as a surrogate endpoint. It has not yet been established whether Trutakna slows kidney function decline over the long term, as measured by eGFR. Continued approval may be contingent on confirmatory eGFR data from the ongoing ORIGIN 3 trial, which Vera Therapeutics and the FDA have agreed to analyze earlier than originally planned. eGFR results are anticipated in Q3 2026. An sBLA for full approval is targeted for Q4 2026. BLA accepted with Priority Review in January 2026. Safety signals: infections in 32% (atacicept) versus 28% (placebo); injection site reactions in 30% (atacicept) versus 5% (placebo); live vaccines are contraindicated during treatment. |
|---|
IgA nephropathy is the most common biopsy-proven primary glomerulonephritis worldwide, yet most patients who have it don’t know for years. The disease begins silently, with abnormal IgA antibodies depositing in the glomeruli of the kidneys and slowly damaging the filtering units that keep waste in the urine and protein in the bloodstream. The first sign is often blood in the urine after an upper respiratory infection, or protein showing up on a routine urinalysis. The diagnosis requires a kidney biopsy. And between 30% and 50% of untreated patients will progress to kidney failure within 20 to 25 years.
For most of the history of nephrology, treatment consisted of blood pressure control, RAAS blockade to reduce proteinuria, and in some patients a course of systemic corticosteroids with their accompanying side effects and limited long-term efficacy. Then, between 2021 and 2024, the IgAN treatment landscape transformed rapidly as the FDA approved five drugs targeting different aspects of the disease’s pathophysiology.
Trutakna (atacicept-vymj, Vera Therapeutics), approved July 7, 2026, is the sixth. What makes it mechanistically important within this crowded field is that it targets the disease earlier in its pathogenic cascade than any of the others: at the B-cell cytokine level where the abnormal IgA antibody production begins, using a dual-target approach that blocks both BAFF and APRIL simultaneously. No other approved IgAN drug does this. The 36-week Phase 3 interim data showed a 42% reduction in proteinuria versus placebo. Whether that proteinuria reduction translates into preserved kidney function over years is the critical question, and the answer is coming soon.
What IgA Nephropathy Is: The Four-Hit Disease
IgA nephropathy, also known as Berger’s disease after the French nephrologist Jean Berger who first described it in 1968, is defined by mesangial deposits of IgA-dominant immune complexes in the kidney. Understanding what goes wrong requires following a sequence of immunological events that researchers now describe as the “four-hit hypothesis.”
Hit 1: Aberrant IgA1 glycosylation. IgA1, one of the two subclasses of IgA antibody, has a hinge region with multiple O-linked glycan chains. In patients with IgAN, these glycans are incompletely formed: they lack the normal galactose residues and are described as galactose-deficient IgA1 (Gd-IgA1). Gd-IgA1 is produced in higher quantities in IgAN patients than in healthy individuals and is the molecular abnormality that drives the entire downstream cascade.
Hit 2: Autoantibody production. The body recognizes the aberrant Gd-IgA1 as foreign and produces anti-glycan autoantibodies (IgG and IgA) directed against the abnormal sugar residues. These autoantibodies are the second abnormality.
Hit 3: Immune complex formation. The autoantibodies bind to circulating Gd-IgA1 to form large immune complexes. These complexes circulate in the bloodstream and are too large to be efficiently cleared by normal mechanisms.
Hit 4: Mesangial deposition and kidney injury. The immune complexes deposit in the mesangium, the connective tissue between the glomerular capillaries. Mesangial cells respond by proliferating and producing inflammatory cytokines and extracellular matrix proteins. The complement system is activated through the lectin and alternative pathways. The resulting glomerular inflammation and fibrosis progressively damage the kidney’s filtering function, reflected clinically as proteinuria, hematuria, and eventually declining eGFR.
The critical insight from this four-hit model is that hit 1, the overproduction of Gd-IgA1, is fundamentally a B-cell problem. The abnormal antibodies come from B cells and plasma cells that have been inappropriately activated by cytokines in the mucosa and lymphoid tissue. This is where BAFF and APRIL become central to the pathophysiology and where Trutakna’s mechanism fits.
| Why IgAN is more common in some populations than others IgAN is the most common primary glomerulonephritis worldwide, but its distribution is uneven. Prevalence is highest in East Asia, where IgAN accounts for 40% to 50% of biopsy-proven glomerulonephritis cases. In Europe it accounts for 20% to 30%, and in North America 10% to 20%. The higher prevalence and more aggressive disease course in East Asian populations likely reflects both genetic susceptibility variants and differences in mucosal immune activation. Overall incidence is at least 2.5 cases per 100,000 adults per year. In practical terms, given that kidney biopsies are not performed as readily in all healthcare systems, IgAN is almost certainly substantially underdiagnosed, with many patients carrying the disease without a confirmed pathological diagnosis. |
|---|
How Atacicept Works: Dual BAFF and APRIL Inhibition
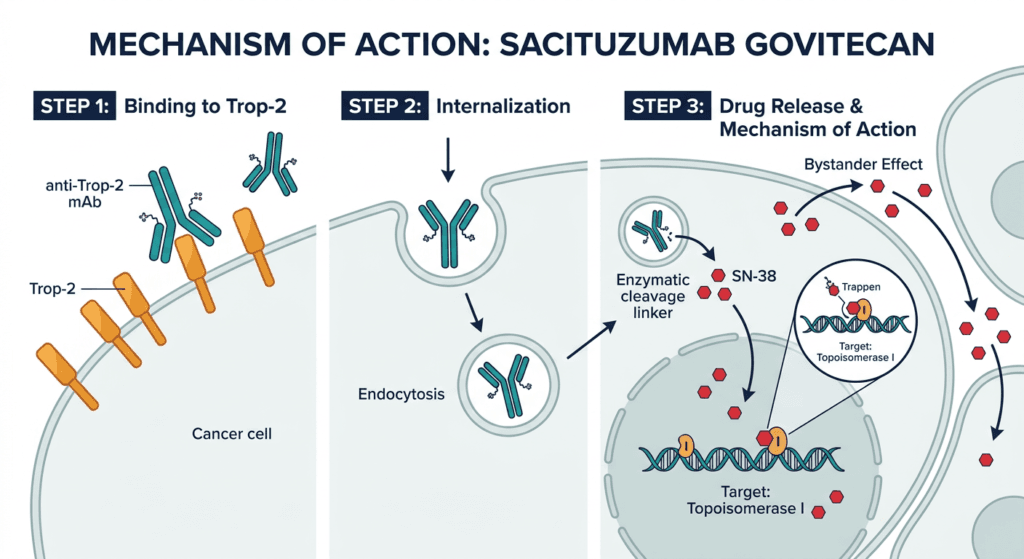
BAFF (B-cell activating factor, also known as BLyS) and APRIL (A proliferation-inducing ligand) are two cytokines produced primarily by innate immune cells, dendritic cells, macrophages, and epithelial cells in response to mucosal immune stimulation. Both act on receptors expressed on B cells and plasma cells (the antibody-secreting cell type that B cells mature into) to promote their survival, proliferation, and differentiation into antibody-producing cells.
In IgAN, both BAFF and APRIL are overexpressed, particularly in mucosal sites including the gut-associated lymphoid tissue and tonsils, which are thought to be the primary sites of Gd-IgA1 production. The elevated BAFF and APRIL levels drive excessive B-cell and plasma cell survival, amplifying the production of both Gd-IgA1 itself and the autoantibodies that bind it to form immune complexes. Reducing BAFF and APRIL levels should reduce this aberrant B-cell activity, lower Gd-IgA1 and autoantibody production, and thereby reduce the formation and mesangial deposition of pathogenic immune complexes.
Atacicept is a recombinant fusion protein combining the extracellular domain of the transmembrane activator and calcium modulator and cyclophilin ligand interactor (TACI) receptor with the Fc portion of human IgG1. TACI is the receptor that naturally binds both BAFF and APRIL. By mimicking this receptor in soluble form, atacicept acts as a decoy: it captures both BAFF and APRIL in the circulation before they can bind to B cells and plasma cells, neutralizing both cytokines simultaneously.
This dual neutralization is the key mechanistic distinction from the only other APRIL-directed therapy approaching approval for IgAN: sibeprenlimab (Vertex Pharmaceuticals), which targets only APRIL. Whether blocking both BAFF and APRIL provides additive clinical benefit over blocking APRIL alone is a question that current trial programs will ultimately need to address through comparative data or head-to-head studies. The available data suggest meaningful clinical activity for both approaches; which performs better in the long term remains to be established.
Other approved IgAN therapies address the disease through entirely different mechanisms: Tarpeyo and Kinpeygo target mucosal IgA production through gut-targeted corticosteroid action; Filspari combines endothelin A receptor blockade with angiotensin receptor blockade (sparsentan); Vanrafia blocks the endothelin A receptor (atrasentan); and Fabhalta inhibits complement factor B (iptacopan). The mechanistic diversity of the approved IgAN landscape reflects the multiple pathogenic pathways contributing to the four-hit cascade and provides clinicians and patients with options targeting different aspects of the disease.
The ORIGIN 3 Trial: What the Data Shows and What It Does Not Yet Establish
Trial design
ORIGIN 3 (NCT04716231) is an ongoing global, multicenter, randomized, double-blind, placebo-controlled Phase 3 trial enrolling 431 adults with biopsy-confirmed primary IgAN. Patients were randomized 1:1 to atacicept 150 mg administered subcutaneously once weekly via autoinjector or placebo. The trial is still running in its placebo-controlled, blinded phase to evaluate the primary long-term efficacy endpoint of change in eGFR.
The accelerated approval was based on a prespecified interim analysis of the first 203 patients who received at least 1 dose of atacicept or placebo and had reached the 36-week assessment point. The primary endpoint of this interim analysis was change in 24-hour urine protein-to-creatinine ratio (UPCR) from baseline to week 36.
Efficacy results at 36 weeks
| Endpoint | Atacicept (n=approximately 101) | Placebo (n=approximately 102) | Result |
|---|---|---|---|
| UPCR reduction from baseline | 46% | Reference | Statistically significant and clinically meaningful |
| UPCR reduction versus placebo | 42% | Reference | p less than 0.0001 |
| Analysis timing | 36-week prespecified interim | 36-week prespecified interim | Per prespecified analysis plan |
Source: Vera Therapeutics FDA approval press release. GlobeNewswire. July 7, 2026. ORIGIN 3 NCT04716231.
A 42% reduction in UPCR compared to placebo at 36 weeks is a clinically meaningful reduction in proteinuria. In IgAN clinical trials and regulatory frameworks, proteinuria measured by UPCR is now an accepted surrogate endpoint for predicting long-term kidney outcomes, based on consistent observational data showing that proteinuria reduction correlates with slower eGFR decline over years of follow-up. The FDA accepted proteinuria reduction as the basis for accelerated approval across multiple prior IgAN approvals, including Tarpeyo, Filspari, and Fabhalta.
What is not yet established
The prescribing label for Trutakna includes a critical qualification that patients and clinicians should understand directly:
“This indication is approved under accelerated approval based on a reduction of proteinuria. It has not been established whether Trutakna slows kidney function decline over the long-term in patients with IgAN. Continued approval for this indication may be contingent upon verification and description of clinical benefit in the ongoing ORIGIN 3 trial.”
In plain terms: the drug reduces proteinuria, and proteinuria is a surrogate marker for kidney health. But the confirmatory evidence showing that this proteinuria reduction actually translates into slower kidney function loss over years, as measured by eGFR trajectory, has not yet been generated. That evidence is coming from the ongoing ORIGIN 3 trial, and Vera Therapeutics has stated it reached agreement with the FDA to conduct the eGFR analysis earlier than originally planned. Results are anticipated in Q3 2026, and a supplemental BLA for full approval is targeted for Q4 2026.
This is the standard accelerated approval pathway in IgAN and is not unique to atacicept. The entire recent IgAN drug approval wave has followed this same proteinuria-first-then-eGFR framework. The precedent for conversion to full approval on confirmatory eGFR data in IgAN has been established by prior approvals in this space. Whether ORIGIN 3’s eGFR data confirms the expected clinical benefit is the question that matters most for long-term prescribing confidence.
The IgAN Treatment Landscape After July 2026
Understanding where Trutakna fits requires seeing the full current picture of approved IgAN therapies and their distinct mechanisms:
| Drug | Company | Mechanism | FDA approval | Approval type |
|---|---|---|---|---|
| Tarpeyo (budesonide EC) | Calliditas | Gut-targeted corticosteroid (reduces mucosal IgA production) | December 2021 | Accelerated; full approval 2023 |
| Filspari (sparsentan) | Travere | Dual endothelin A and angiotensin receptor antagonist | February 2023 | Accelerated; full approval 2024 |
| Fabhalta (iptacopan) | Novartis | Complement factor B inhibitor | August 2024 | Accelerated |
| Vanrafia (atrasentan) | Otsuka | Selective endothelin A receptor antagonist | August 2024 | Full approval (ALIGN trial) |
| Voyxact (iptacopan) | Novartis | Complement factor B inhibitor | Full complement indication | Overlapping with Fabhalta |
| Trutakna (atacicept) | Vera Therapeutics | Dual BAFF and APRIL inhibitor | July 7, 2026 | Accelerated |
Note: Sibeprenlimab (Vertex), targeting APRIL only, is in Phase 3 and has not yet been approved.
The mechanistic diversity of this landscape matters clinically. Patients with IgAN may benefit from different approaches depending on where in the four-hit cascade their disease is most driven, their comorbidities and contraindications, and the specific features of their disease at the time of treatment initiation. Atacicept’s upstream B-cell cytokine targeting provides an option that addresses the source of Gd-IgA1 production, which is distinct from the complement inhibition, hemodynamic, and mucosal corticosteroid approaches of other approved drugs.
The competitive landscape also creates questions about combination therapy: could addressing multiple pathogenic steps simultaneously, such as reducing Gd-IgA1 production with atacicept while blocking complement activation with iptacopan, provide additive benefit? These are questions that ongoing research will address but that are outside the current label for any of these agents.
Dosing and Administration
Trutakna is administered as a 150 mg subcutaneous injection once weekly. The injection is self-administered by the patient at home using a pre-filled autoinjector. Injection sites include the abdomen, thigh, or upper arm, rotating sites with each weekly injection.
The home self-administration model is a meaningful practical advantage for a drug intended for long-term use in a patient population managing a chronic progressive kidney disease. Patients receive training on autoinjector technique before beginning self-injection, typically through Vera Therapeutics’ patient support program.
No dose adjustment is specified for mild to moderate renal impairment, which is relevant because many IgAN patients present with some degree of kidney function reduction at the time of treatment initiation. Prescribing information should be reviewed for guidance in patients with more severe renal impairment.
Safety: What the ORIGIN 3 Data Covers
The safety profile from the ORIGIN 3 interim analysis was broadly consistent with the class-level risks of BAFF and APRIL inhibition, reflecting their roles in B-cell homeostasis and immune function.
Key safety findings from ORIGIN 3 interim:
| Safety item | Atacicept | Placebo | Clinical relevance |
|---|---|---|---|
| Any infection | 32% | 28% | Modest increase; B-cell suppression reduces immune competence |
| Injection site reactions | 30% | 5% | The most distinct adverse event profile for atacicept; predominantly mild local reactions |
| Serious infections | Low absolute rate | Low absolute rate | Monitor for serious or unusual infections throughout treatment |
Warnings and precautions from the Trutakna prescribing information:
Serious infections: BAFF and APRIL support B-cell survival and function. By inhibiting both, atacicept reduces B-cell populations and the antibodies they produce, including normal protective antibodies. This creates a degree of immunosuppression that increases infection susceptibility. Serious infections requiring hospitalization have been reported. Clinicians should assess for active infection before initiating Trutakna and should not initiate in patients with active infections. Patients should be monitored for infection throughout treatment and instructed to report new symptoms promptly.
Live vaccines contraindicated: Because Trutakna suppresses B-cell function and antibody responses, live attenuated vaccines should not be administered to patients receiving the drug. Vaccinations with live vaccines should be completed before initiating treatment. Non-live vaccines may have reduced efficacy during treatment; the timing of non-live vaccinations relative to atacicept dosing should be discussed with the prescriber.
Hypogammaglobulinemia: Sustained BAFF and APRIL inhibition can reduce immunoglobulin levels over time. Monitoring of immunoglobulin levels is recommended. Patients with pre-existing hypogammaglobulinemia may be at higher risk for infectious complications.
Hypersensitivity reactions: Serious hypersensitivity reactions have been reported with atacicept. Patients should be observed after injection for signs of hypersensitivity and instructed to seek medical attention for any serious reaction.
Embryo-fetal toxicity: Atacicept can cause fetal harm based on its mechanism of action affecting B-cell development. Females of reproductive potential should use effective contraception during treatment and for a specified period after the last dose. Pregnancy testing before initiating treatment is recommended for females of reproductive potential.
What This Means for Patients and Clinicians
For patients with primary IgAN
Trutakna adds a meaningful new option to the IgAN treatment landscape, particularly for patients who have not achieved adequate proteinuria control on existing therapies, who are intolerant to current options, or whose disease is driven primarily by the upstream B-cell cytokine pathways that BAFF and APRIL regulation addresses.
The practical advantages of Trutakna for patients include once-weekly home self-administration (eliminating infusion center visits), a well-defined and manageable side effect profile, and a mechanism that targets the immunological source of the disease rather than its downstream consequences.
The important transparency point every patient deserves: the approval is based on reducing proteinuria, a surrogate marker. The evidence that this proteinuria reduction translates into slower progression to kidney failure, the outcome that matters most, is currently awaited from the ongoing ORIGIN 3 confirmatory analysis. This is not a reason to avoid the drug, because every other recently approved IgAN drug followed the same pathway, and the proteinuria-to-eGFR correlation is well-established. But it is information that should be part of a shared decision-making conversation with your nephrologist.
The confirmatory eGFR data expected in Q3 2026 will be one of the most watched datasets in nephrology this year. If ORIGIN 3 shows preserved kidney function alongside the proteinuria reduction, the case for Trutakna in the IgAN treatment algorithm will strengthen considerably.
For nephrologists
Trutakna’s dual BAFF/APRIL mechanism fills a specific niche in the IgAN therapeutic landscape: upstream B-cell cytokine targeting for patients where reducing aberrant Gd-IgA1 production is the primary therapeutic goal. The 42% placebo-adjusted UPCR reduction at 36 weeks is consistent with the proteinuria reduction seen with other approved IgAN agents and provides a basis for use in clinical practice pending confirmatory eGFR data.
The comparative effectiveness question between atacicept and sibeprenlimab (APRIL-only inhibition), and between both of these upstream B-cell targeting approaches and the complement, hemodynamic, and mucosal corticosteroid approaches, will take years of real-world experience and potentially head-to-head trials to fully resolve. In the meantime, the mechanistic diversity of the approved IgAN landscape supports individualized treatment selection based on patient disease characteristics, comorbidities, and prior therapy history.
The infection monitoring consideration and the live vaccine contraindication are the most practically important safety management points for ongoing surveillance in atacicept-treated patients.
For related HED coverage on rare kidney disease and immunology drug approvals, see our post on Tregzi (marnetegragene autotemcel-vldq) receiving FDA approval as the first precision-engineered cell therapy for allogeneic stem cell transplantation and our coverage of the Lumvoa (veligrotug-vvze) approval for thyroid eye disease across both active and chronic disease phases.
If you or a family member has been diagnosed with IgA nephropathy, the National Kidney Foundation (kidney.org; 1-800-622-9010) and the IgA Nephropathy Foundation maintain current patient resources, treatment information, and clinical trial directories.
Sources
Vera Therapeutics FDA approval press release: Vera Therapeutics Receives FDA Accelerated Approval for TRUTAKNA for Adult Patients with Primary IgA Nephropathy. GlobeNewswire. July 7, 2026.
Drugs.com approval news: FDA Grants Accelerated Approval for Trutakna (atacicept-vymj) for Adult Patients with Primary IgA Nephropathy. drugs.com. July 7, 2026.
HCPLive clinical summary (ORIGIN 3 data, safety profile): FDA Approves Atacicept (Trutakna) for IgA Nephropathy. hcplive.com. July 2026.
AJMC clinical and competitive landscape analysis: FDA Approves Atacicept for IgA Nephropathy. ajmc.com. July 2026.
Fierce Pharma (competitive landscape, sibeprenlimab context): Vera’s dual-target atacicept wins FDA approval for IgAN. fiercepharma.com. July 2026.
Pharmaceutical Commerce (specialty launch context): What Trutakna’s Approval Means for Specialty Launches. pharmaceuticalcommerce.com. July 2026.
Trutakna approval history: Trutakna FDA Approval History. drugs.com.
ORIGIN 3 trial registration: NCT04716231. ClinicalTrials.gov.
BAFF and APRIL role in IgAN pathogenesis: The role of BAFF and APRIL in IgA nephropathy: pathogenic mechanisms and targeted therapies. PMC10867227.
IgAN four-hit pathophysiology: The Pathophysiology of IgA Nephropathy. PMC3892742.
Gd-IgA1 and immune complex formation: The Origin and Activities of IgA1-Containing Immune Complexes in IgA Nephropathy. PMC4828451.
IgAN clinical trials overview: IgA Nephropathy: An Overview of the Clinical Trials. Kidney Medicine. 2025.
IgAN StatPearls overview: IgA Nephropathy (Berger Disease). StatPearls. NCBI.
Tarpeyo FDA approval: FDA approves budesonide for IgA nephropathy. FDA.gov.
Filspari FDA approval: FDA approves sparsentan for IgA nephropathy. FDA.gov.
Fabhalta/Voyxact FDA approval: FDA approves iptacopan for IgA nephropathy. FDA.gov.
Vanrafia FDA approval: FDA approves atrasentan for IgA nephropathy. FDA.gov.
Trutakna prescribing information: TRUTAKNA (atacicept-vymj) Prescribing Information. Vera Therapeutics. 2026.
KDIGO 2025 IgAN guideline: Executive summary of the KDIGO 2025 Clinical Practice Guideline for the Management of IgA Nephropathy and IgA Vasculitis. Kidney Int. 2025;108(4):548-554.
Patient resources: National Kidney Foundation: 1-800-622-9010 | IgA Nephropathy Foundation | American Kidney Fund | Vera Therapeutics patient support
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice. Trutakna received accelerated approval based on reduction of proteinuria as a surrogate endpoint; it has not yet been established that the drug slows long-term kidney function decline. Decisions about initiating Trutakna for primary IgA nephropathy should be made in close consultation with a board-certified nephrologist who can evaluate proteinuria levels, eGFR trajectory, kidney biopsy findings, and all treatment options in the context of each individual patient’s disease characteristics. |
|---|