
| 📌 The essentials On May 13, 2026, the FDA approved Fasenra (benralizumab, AstraZeneca) for the treatment of adults and pediatric patients aged 12 years and older with hypereosinophilic syndrome (HES) without an identifiable non-hematologic secondary cause. This is Fasenra’s third FDA-approved indication, joining severe eosinophilic asthma (approved 2017) and eosinophilic granulomatosis with polyangiitis (EGPA, approved 2022). On May 21, 2026, the European Medicines Agency’s CHMP issued a positive opinion recommending EU approval of Fasenra for HES (as part of a label update also covering severe asthma and EGPA). The clinical basis: Phase 3 NATRON trial (NCT04191304), published in Nature Medicine on March 31, 2026, enrolling 133 patients with HES (67 benralizumab, 66 placebo), 24 weeks, randomized double-blind placebo-controlled. Primary endpoint: 65% reduction in risk of first HES flare (HR 0.35; 95% CI 0.18 to 0.69; p=0.0024). All secondary endpoints met, including 66% reduction in annualized flare rate (0.41 versus 1.23 flares/year), 92% reduction in risk of hematologic relapse (HR 0.08; p less than 0.0001), and significant improvement in patient-reported fatigue by week 4. Dosing: 30 mg subcutaneous injection once every 4 weeks (different from the loading dose schedule used in asthma). Fasenra is the second anti-eosinophil biologic approved for HES, after mepolizumab (Nucala, approved 2020). |
|---|
Hypereosinophilic syndrome (HES) is a condition most people have never heard of. Most primary care providers encounter it rarely if at all. And for the approximately 30,000 to 200,000 Americans estimated to be living with it, that relative unfamiliarity often means years of unexplained symptoms, difficult diagnoses, and limited treatment options.
On May 13, 2026, the FDA approved Fasenra (benralizumab) for HES, making it the second targeted biologic approved for this rare condition and the first approved for patients as young as 12. The pivotal trial behind the approval, NATRON, was published in Nature Medicine and met all of its endpoints, including a clinically meaningful reduction in flares, a striking near-elimination of hematologic relapse risk, and the first statistically significant improvement in fatigue ever demonstrated in a Phase 3 HES trial.
This post covers what HES is and why it is hard to diagnose and treat, how benralizumab works, what every NATRON endpoint showed, and what this approval means for patients and clinicians navigating this condition.
What Hypereosinophilic Syndrome Is
Eosinophils are a type of white blood cell that normally account for less than 5% of circulating leukocytes. They are part of the immune system’s response to parasitic infections and play a role in allergic inflammation. In healthy adults, the normal eosinophil count is below 500 cells per microliter of blood.
HES is defined by three criteria: a blood eosinophil count of 1,500 cells per microliter or higher, persisting for more than one month; evidence of eosinophil-mediated organ or tissue damage; and exclusion of identifiable secondary causes for the eosinophilia.
When eosinophils are persistently elevated and activated, they infiltrate tissues throughout the body and release toxic granule proteins that damage the organs they contact. The damage is cumulative and organ-agnostic: any tissue can be affected. The most common sites of involvement include the lungs, skin, gastrointestinal tract, and heart. Eosinophilic heart disease, including Loeffler endocarditis, is one of the most serious and potentially fatal complications, with thrombus formation, valvular damage, and restrictive cardiomyopathy all documented.
| HES is not one disease: the subtypes matter clinically HES is a heterogeneous group of disorders, not a single entity. The classification includes: myeloproliferative HES, driven by a clonal eosinophil proliferation (the FIP1L1::PDGFRA fusion gene is the most common driver); lymphocytic variant HES, where an abnormal T-cell clone produces excess IL-5; idiopathic HES, where no underlying driver is identified; familial HES; and HES associated with other conditions. The NATRON trial specifically excluded patients with FIP1L1::PDGFRA-positive myeloproliferative HES, because those patients typically respond to imatinib (a tyrosine kinase inhibitor) and represent a distinct pathophysiology. The trial also required patients to be corticosteroid-responsive. The approved indication similarly excludes patients with an identifiable non-hematologic secondary cause. Clinicians should confirm these criteria before prescribing. |
|---|
HES is rare, with an estimated U.S. prevalence of 0.3 to 6.3 cases per 100,000 persons, but the true prevalence is likely underestimated due to diagnostic challenges. The condition can present with a wide and non-specific symptom spectrum: weight loss, fever, cough, chest pain, abdominal pain, skin rash, and neurological symptoms are all documented. Many patients spend years cycling through specialist consultations before a diagnosis is established. In the NATRON trial population, the mean time from first HES symptom appearance to enrollment was more than 8 years.
The Disease Burden That NATRON Was Designed to Measure
The NATRON trial population reflects what HES looks like in clinical practice. Of the 133 enrolled patients (median age 51, range 14 to 87 years, 61.7% female):
- Most commonly involved organs were the lungs (35.6%), skin (25.3%), and gastrointestinal tract (21.8%)
- 39.1% had experienced 2 HES flares in the prior 12 months; 36.8% had experienced 3 or more
- Mean time since first HES symptoms was more than 8 years; mean time since diagnosis was nearly 5 years
- Mean baseline PROMIS Fatigue T-score was 55.1, a score indicating clinically significant fatigue burden (population mean is 50; higher scores indicate worse fatigue)
- Mean blood eosinophil count at baseline was 1,960 cells per microliter
The flare definition used in NATRON is clinically meaningful: a flare required evidence of new or worsening HES clinical manifestations or laboratory abnormalities that resulted in hospitalization, or an increase in oral corticosteroid dose of at least 10 mg per day for at least 2 days, or the addition of new cytotoxic or immunosuppressive therapy. These are genuine clinical events with real consequences, not surrogate biomarker changes.
How Benralizumab Works in HES
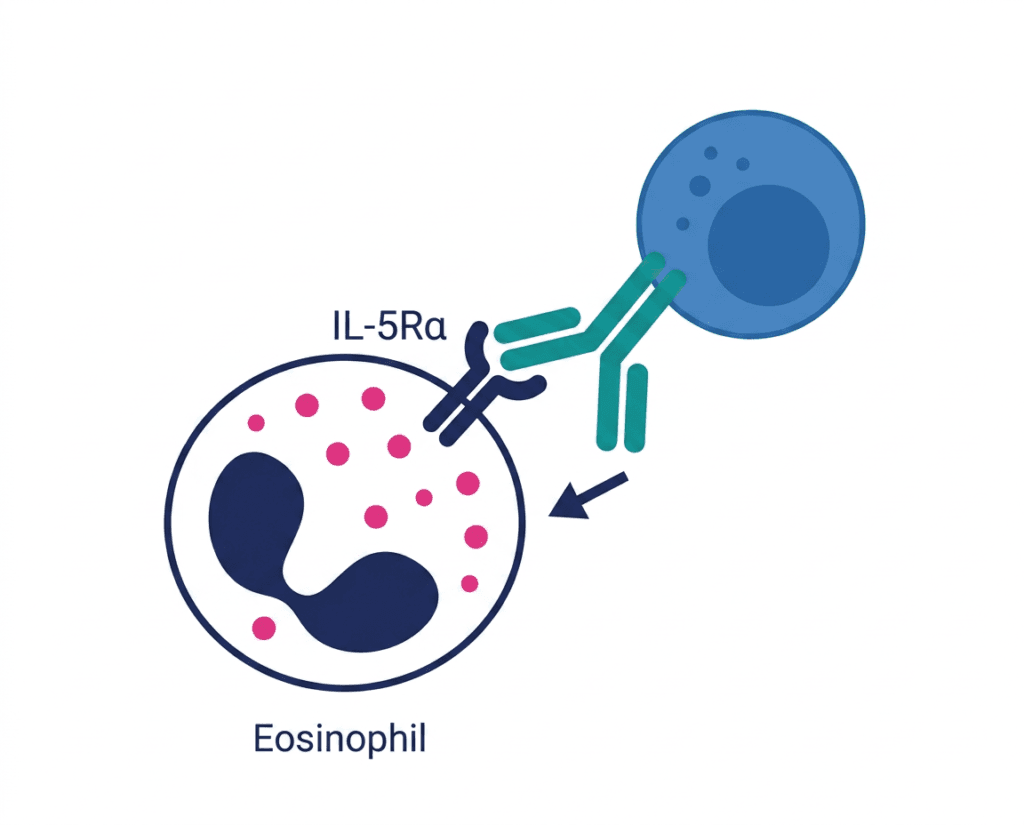
Benralizumab is a humanized, afucosylated monoclonal antibody targeting the alpha subunit of the interleukin-5 receptor (IL-5Rα). IL-5 is the primary cytokine driving eosinophil production, maturation, survival, and activation. By binding IL-5Rα directly on eosinophils and their precursors (rather than binding the IL-5 ligand itself, as mepolizumab does), benralizumab triggers antibody-dependent cell-mediated cytotoxicity (ADCC) through natural killer cells, producing rapid and near-complete depletion of blood and tissue eosinophils within days of the first injection.
The afucosylation engineering is the key pharmacological innovation that distinguishes benralizumab from mepolizumab within the anti-IL-5 class. By removing a fucose sugar from the antibody’s Fc region, the modified antibody binds Fc-gamma receptor IIIa on NK cells with much higher affinity, dramatically enhancing the ADCC-driven cell killing. This mechanism produces a more rapid and more complete eosinophil depletion than IL-5 ligand blocking alone.
In HES, the downstream consequence of this eosinophil depletion is reduced tissue infiltration, less release of eosinophil granule proteins that damage organs, and a lower risk of the inflammatory flares that drive clinical worsening and organ damage. The NATRON data confirms that this biological effect translates to clinically meaningful outcomes.
The NATRON Trial: All the Numbers
Design
NATRON (NCT04191304) was a Phase 3, multicenter, randomized, double-blind, placebo-controlled study. Eligible patients were aged 12 years and older, FIP1L1::PDGFRA-negative, with HES flare signs or symptoms at screening or at least 2 flares in the prior year, and confirmed corticosteroid-responsive disease. Patients were randomized 1:1 to benralizumab 30 mg or placebo subcutaneously every 4 weeks, on top of stable background HES therapy, for a 24-week double-blind treatment period.
Primary endpoint
| Outcome | Benralizumab (n=67) | Placebo (n=66) |
|---|---|---|
| Patients with first HES flare | 19.4% | 42.4% |
| Risk of first flare (HR) | 0.35 (95% CI 0.18 to 0.69) | Reference |
| p-value | 0.0024 | — |
| Flare risk reduction | 65% | — |
The primary endpoint was met with a hazard ratio of 0.35, meaning patients on benralizumab had only 35% of the flare risk of placebo-treated patients. The Kaplan-Meier curves separated early and continued to diverge, with benralizumab-treated patients maintaining lower flare risk throughout the 24-week observation period.
Key secondary endpoints (all statistically significant)
| Outcome | Benralizumab | Placebo | Effect size and significance |
|---|---|---|---|
| Proportion with HES flares | 22.4% | 45.5% | OR 0.31 (95% CI 0.14 to 0.69); p=0.0033 |
| Annualized flare rate | 0.41 flares/year | 1.23 flares/year | RR 0.34 (95% CI 0.18 to 0.63); p=0.0008 |
| Risk of hematologic relapse | HR 0.08 (95% CI 0.03 to 0.20) | Reference | p less than 0.0001; 92% risk reduction |
| PROMIS Fatigue improvement at Week 24 | LS mean difference vs placebo: −4.72 | Reference | 95% CI −7.64 to −1.80; p=0.0017 |
| Fatigue improvement onset | By Week 4 | — | Sustained to Week 24 |
Source: Ogbogu PU, Roufosse F, Akuthota P, et al. Benralizumab versus placebo for hypereosinophilic syndrome: a randomized, placebo-controlled phase 3 trial. Nat Med. Published online March 31, 2026. doi:10.1038/s41591-026-04315-8. NATRON NCT04191304.
The hematologic relapse endpoint, defined as blood eosinophil count rising above 1,000 cells per microliter after confirmed depletion, showed a 92% risk reduction with benralizumab. This near-elimination of hematologic relapse reflects the drug’s mechanism: near-complete eosinophil depletion from the first dose, sustained throughout the dosing period.
The fatigue endpoint is clinically important and worth highlighting. HES-related fatigue is one of the most commonly reported and most disabling symptoms in the condition. The NATRON PROMIS Fatigue results are the first statistically significant improvement in patient-reported fatigue from a Phase 3 HES trial. The fact that the improvement was detectable by week 4, after just the first monthly injection, and sustained to week 24, is a meaningful signal that the biological effect is rapid and durable.
| What PROMIS Fatigue measures and why a difference of 4.72 points is clinically meaningful The PROMIS (Patient-Reported Outcomes Measurement Information System) Fatigue Short Form 7a is a validated, standardized questionnaire assessing fatigue severity and impact over the previous 7 days. Scores are T-scored to a general population mean of 50, with higher scores indicating worse fatigue. The NATRON population had a mean baseline score of 55.1, indicating a clinically significant fatigue burden above population norms. A difference of 4.72 points is consistent with published minimally important difference thresholds for PROMIS Fatigue in chronic disease populations, generally estimated at 4 to 6 points. The improvement therefore exceeds the threshold for clinical meaningfulness, not just statistical significance. |
|---|
Safety
The safety profile of benralizumab in NATRON was consistent with its well-established profile from seven years of use in severe asthma. Crucially, the overall adverse event rate was similar between groups: 64.2% in the benralizumab arm versus 66.7% with placebo, and serious adverse events occurred at virtually identical rates (7.5% versus 7.6%). This parity in overall adverse event burden, combined with a substantially better efficacy profile, is what the FDA reviewed in establishing a favorable benefit-risk balance.
The most common adverse reactions in the HES population (occurring in 5% or more of benralizumab-treated patients and more frequently than placebo) were headache, hypersensitivity reactions (including urticaria, papular urticaria, and rash), and influenza-like illness. The adolescent patients (aged 12 to 17) in the trial had safety and tolerability results consistent with adults.
Where Benralizumab Fits in HES Treatment
Before discussing how benralizumab fits into HES management, it is worth acknowledging that the treatment landscape for HES remains relatively underdeveloped compared to more common eosinophilic conditions.
The standard treatment for HES has historically been high-dose oral corticosteroids, which effectively suppress eosinophils and reduce symptoms but carry well-known long-term toxicity including osteoporosis, weight gain, diabetes, infections, and adrenal suppression. Patients on chronic steroids for HES accumulate organ damage from both the disease and the treatment.
Imatinib (Gleevec) is the first-line agent for FIP1L1::PDGFRA-positive myeloproliferative HES, which is excluded from both the Fasenra and Nucala approvals.
Mepolizumab (Nucala, GSK) was approved for HES in adults in 2020, as the first targeted anti-IL-5 agent for this indication, based on the Phase 3 EXPLORER trial showing a 50% reduction in the risk of HES worsening.
Benralizumab now adds a second biologic option, with a 65% flare risk reduction and the additional advantages of near-complete eosinophil depletion (versus partial reduction with mepolizumab), once-monthly dosing throughout treatment (versus monthly loading then quarterly dosing with mepolizumab after the first three doses), and a pediatric indication down to age 12 (mepolizumab is approved for adults only in HES).
| Benralizumab vs. mepolizumab in HES: what the data comparison suggests No head-to-head trial comparing benralizumab and mepolizumab in HES has been conducted, and cross-trial comparisons are methodologically unreliable. The EXPLORER trial (mepolizumab) enrolled 108 patients and showed 50% reduction in HES worsening; NATRON enrolled 133 patients and showed 65% reduction in flare risk. The patient populations, flare definitions, and time periods differed in ways that make numerical comparison inappropriate. What is appropriate to note is that both drugs reduce eosinophils via the IL-5 pathway and both have demonstrated meaningful clinical benefit in HES. The mechanistic distinction (receptor blockade with direct eosinophil depletion versus ligand blockade with partial reduction) may matter more in individual patients with high eosinophil burden or disease that is incompletely controlled on mepolizumab. The choice between them will ultimately depend on prescriber experience, patient-specific factors, and in some cases prior response to one agent. |
|---|
Dosing: An Important Difference From the Asthma and EGPA Schedule
Clinicians already prescribing Fasenra for severe asthma or EGPA should note that the dosing schedule for HES is different.
For severe asthma: 30 mg every 4 weeks for the first 3 doses, then 30 mg every 8 weeks thereafter.
For EGPA and HES: 30 mg once every 4 weeks throughout treatment. No switch to an every-8-week schedule.
This distinction matters for prescription writing, patient counseling, and specialty pharmacy dispensing. Patients should receive a clear explanation that their dosing schedule differs from what they may have read about Fasenra in the asthma context.
Administration: subcutaneous injection into the upper arm, thigh, or abdomen. Can be administered by a healthcare provider or by self-injection after proper training.
What Patients and Caregivers Should Know
Who is this approval for?
Adults and pediatric patients aged 12 years and older with HES that does not have an identifiable non-hematologic secondary cause, and specifically FIP1L1::PDGFRA-negative disease. If you have been diagnosed with HES and are currently managing the condition with oral corticosteroids or other systemic therapies with inadequate control or significant side effects, Fasenra is now an FDA-authorized option to discuss with your hematologist or allergist-immunologist.
When to involve a specialist
HES is a rare condition that requires specialist expertise for accurate diagnosis and management. Hematologists, allergist-immunologists, and in some cases rheumatologists or pulmonologists depending on organ involvement are the specialists most experienced with HES diagnosis and treatment. Because the condition is rare, specialized centers with multi-disciplinary eosinophilia programs (several are affiliated with academic medical centers in the United States) often have the most experience with the full diagnostic workup, including genetic testing for FIP1L1::PDGFRA and lymphocytic variant HES markers.
Patient support
The American Partnership for Eosinophilic Disorders (APFED) is the primary patient advocacy organization for eosinophilic conditions in the United States and maintains updated resources on HES including a specialist referral network. The Hypereosinophilic Syndrome Research Program at NIH through the National Institute of Allergy and Infectious Diseases has been a leading center for HES research and may have open clinical trials. The National Organization for Rare Disorders (NORD) maintains a current clinical overview of HES.
For related HED coverage on other biologic approvals in eosinophilic conditions, see our post on Trimbow, the first single-inhaler triple therapy for uncontrolled asthma, and our post on Fasenra’s companion indication in EGPA and the broader role of anti-IL-5 biologics in eosinophilic inflammation.
Sources
FDA approval announcement: FDA approves benralizumab (Fasenra) for hypereosinophilic syndrome. FDA.gov. May 13, 2026.
AstraZeneca US press release: FASENRA approved in US for hypereosinophilic syndrome. astrazeneca-us.com. May 14, 2026.
NATRON primary publication (Nature Medicine): Ogbogu PU, Roufosse F, Akuthota P, et al. Benralizumab versus placebo for hypereosinophilic syndrome: a randomized, placebo-controlled phase 3 trial. Nat Med. Published online March 31, 2026. doi:10.1038/s41591-026-04315-8.
NATRON ACAAI 2025 abstract (Annals of Allergy): Benralizumab for patients with hypereosinophilic syndrome: A randomized, double-blind, placebo-controlled phase 3 trial (NATRON). Ann Allergy Asthma Immunol. November 2025.
NATRON full results (AstraZeneca press release, November 2025): Statistically significant NATRON Phase III trial results for hypereosinophilic syndrome show Fasenra delayed time to first flare. astrazeneca.com.
NATRON trial registration: NCT04191304. ClinicalTrials.gov.
EMA CHMP positive opinion (May 21, 2026): Fasenra. EMA. ema.europa.eu.
PharmExec FDA approval coverage: FDA Approves Fasenra for Hypereosinophilic Syndrome. pharmexec.com. May 2026.
Pulmonology Advisor NATRON coverage: Add-On Benralizumab Effective in Hypereosinophilic Syndrome. pulmonologyadvisor.com.
NATRON design paper (Blood/ASH 2023): The Phase 3 NATRON Study Evaluating Benralizumab in Patients with Hypereosinophilic Syndrome: Study Design and Patient Characteristics. Blood. 2023.
HES GARD overview: Hypereosinophilic Syndrome. rarediseases.info.nih.gov.
HES StatPearls: Hypereosinophilic Syndrome. StatPearls. NCBI.
Eosinophil biology: Eosinophils. StatPearls. NCBI.
Benralizumab mechanism (afucosylation and ADCC): Anti-IL-5 and IL-5Rα biologics: mechanisms and clinical evidence. PMC7186825.
Eosinophilic heart disease: Cardiac Manifestations in Hypereosinophilic Syndrome. PMC5454610.
Mepolizumab HES FDA approval: FDA approves mepolizumab for treatment of hypereosinophilic syndrome. FDA.gov.
PROMIS Fatigue instrument: PROMIS Adult Measures: Fatigue. healthmeasures.net.
Corticosteroids overview: Corticosteroids. StatPearls. NCBI.
Fasenra prescribing information: FASENRA (benralizumab) Prescribing Information. AstraZeneca. 2026.
Patient resources: American Partnership for Eosinophilic Disorders (APFED) | NIH HES Research Program (NIAID) | NORD: Hypereosinophilic Syndrome | ClinicalTrials.gov: HES
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Hypereosinophilic syndrome requires accurate diagnosis and specialist management. Treatment decisions should be made in consultation with a qualified allergist-immunologist or hematologist experienced in eosinophilic conditions. |
|---|