| 📌 The essentials On May 8, 2026, the FDA approved Ocrevus (ocrelizumab, Genentech) for the treatment of relapsing-remitting multiple sclerosis (RRMS) in pediatric patients aged 10 years and older who weigh at least 25 kg (approximately 55 pounds). This is Ocrevus’s first pediatric indication, expanding its label beyond adults. Ocrevus becomes only the second FDA-approved disease-modifying therapy for pediatric RRMS, after fingolimod (Gilenya, Novartis), and the first approved high-efficacy anti-CD20 therapy for this population. The clinical basis: Phase 3 OPERETTA 2 trial (NCT05123703), 187 pediatric patients aged 10 to 17 years with RRMS, randomized double-blind comparison of ocrelizumab versus fingolimod. Primary endpoint: ocrelizumab was non-inferior to fingolimod in reducing annualized relapse rate. MRI superiority: 48% reduction in new or enlarging T2 lesions (p=0.001) and 87% reduction in gadolinium-enhancing T1 lesions (p=0.001) versus fingolimod. Safety: no adverse events led to treatment withdrawal in the ocrelizumab arm. How it is given: 600 mg intravenous infusion every 24 weeks (same dose and schedule as adults). Weight minimum: the drug is not known to be safe or effective in children under 10 years of age or weighing less than 25 kg. |
|---|
Multiple sclerosis in children and adolescents is a different clinical scenario than most people picture when they think of MS. Pediatric-onset MS (POMS) represents approximately 3 to 5% of all MS cases globally, with an estimated 5,000 to 10,000 children and adolescents affected in the United States. The condition is not mild: children with POMS typically have higher relapse rates than adults, more rapid accumulation of new brain lesions on MRI, and a relapsing disease course in the vast majority of cases. What they have historically had is very few approved treatment options.
Until May 8, 2026, fingolimod (Gilenya) was the only FDA-approved disease-modifying therapy for pediatric RRMS, a status it has held since its pediatric approval in 2018. Every other MS treatment used in children and adolescents was prescribed off-label, without the clinical trial evidence base that formal approval requires.
That changed when the FDA approved Ocrevus (ocrelizumab) for RRMS in patients aged 10 and older, based on the Phase 3 OPERETTA 2 trial. For the first time, a high-efficacy anti-CD20 B-cell depleting therapy is formally available for pediatric patients who have not responded adequately to first-line agents or whose disease activity warrants a more aggressive approach from the start.
What Pediatric-Onset Multiple Sclerosis Is and Why Treatment Is Urgent
Pediatric-onset MS is defined as MS with symptom onset before age 18. Children and adolescents with POMS experience the same types of episodes as adults, including optic neuritis, limb weakness, sensory disturbance, brainstem and cerebellar dysfunction, and cognitive slowing. But several features distinguish POMS from typical adult-onset disease.
Higher initial disease activity: Children with POMS typically have higher relapse rates than adult patients early in the disease course. Brain MRI at diagnosis often shows extensive T2 lesion burden. The inflammatory activity is often vigorous, reflecting the heightened immune responsiveness of the developing immune system.
Predominantly relapsing course: Nearly all pediatric MS cases are relapsing-remitting, not progressive, at onset. This is both a prognostic advantage (the disease course is more amenable to disease modification) and a treatment priority (relapses in developing brains carry distinct risks for cognitive and neurological development that are not fully quantified in adults).
Cognitive burden: Cognitive impairment is documented in a substantial proportion of children with MS, affecting processing speed, attention, memory, and executive function. Because POMS occurs during a critical period of brain development and education, the impact of unchecked disease activity on long-term cognitive trajectory is a distinct and serious concern.
Long disease duration ahead: A child diagnosed at age 12 faces potentially decades of living with MS before the disease is biologically comparable to someone diagnosed at 50. The cumulative burden of every avoided relapse, every suppressed lesion, and every year of preserved neurological function compounds over that longer horizon.
| Why fingolimod was the only approved option for so long, and what its limitations are Fingolimod (Gilenya) was the first FDA-approved MS therapy for pediatric patients, receiving its pediatric RRMS approval in May 2018 based on the Phase 3 PARADIGMS trial. It works by sequestering lymphocytes in lymph nodes, preventing them from entering the central nervous system and causing inflammation. It is effective and its oral administration is an advantage for younger patients. But it carries significant safety concerns: a first-dose cardiac monitoring requirement (due to the risk of bradycardia and heart block), risk of serious infections including PML and cryptococcal meningitis, varicella zoster reactivation, and ophthalmologic monitoring requirements for macular edema. In a pediatric population, these monitoring requirements represent a real burden on families, schools, and clinical teams. Until OPERETTA 2, the absence of a high-efficacy alternative with a clinically distinct mechanism and monitoring profile left neurologists and families with limited flexibility. |
|---|
How Ocrelizumab Works and Why B-Cell Depletion Matters in MS
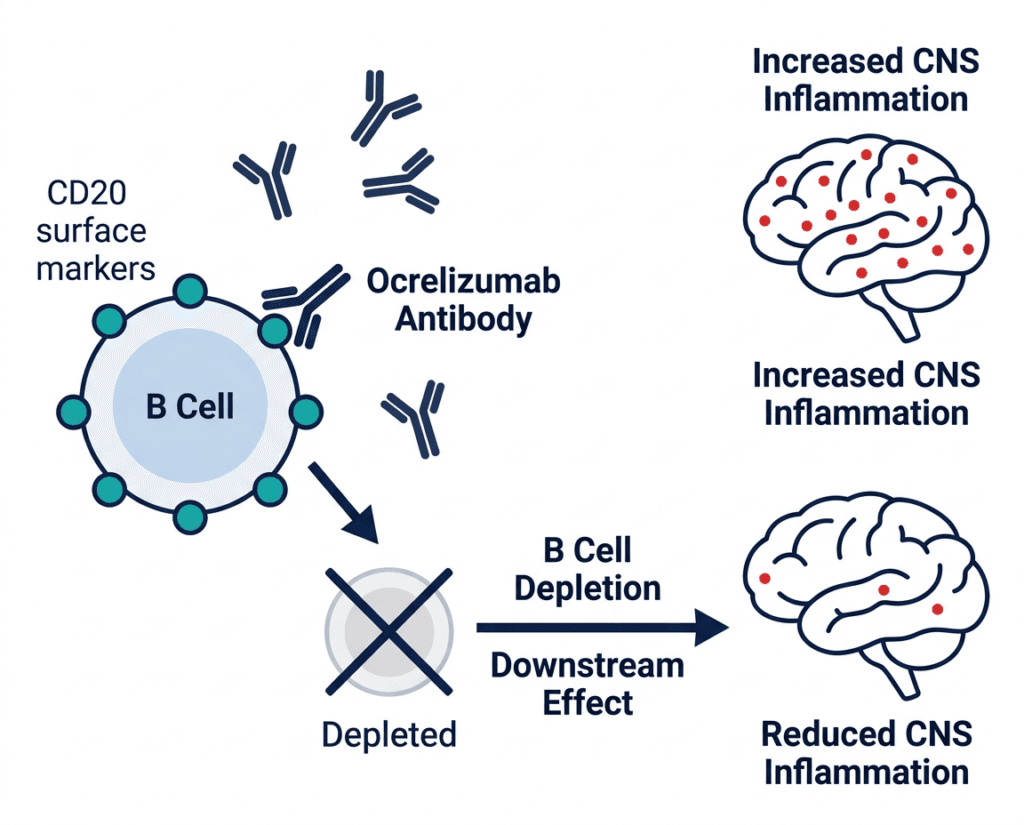
Ocrelizumab is a humanized anti-CD20 monoclonal antibody. CD20 is a surface protein expressed on B cells throughout most of their development, from pre-B cells through mature B cells, but not on plasma cells or hematopoietic stem cells. When ocrelizumab binds CD20, it triggers B-cell depletion through three mechanisms: antibody-dependent cellular cytotoxicity (ADCC), complement-dependent cytotoxicity (CDC), and direct apoptosis induction.
The role of B cells in MS pathogenesis has been substantially clarified in the decade since ocrelizumab’s original approval. B cells contribute to MS inflammation not just as antibody-producing cells but as antigen-presenting cells that activate CD4+ and CD8+ T cells, as producers of pro-inflammatory cytokines including TNF-alpha, IL-6, and IL-12, and as modulators of the inflammatory microenvironment within CNS lesions. Depleting B cells interrupts these multiple contributions to disease activity, producing the robust efficacy on both relapse rates and MRI lesion accumulation that has made ocrelizumab one of the most effective MS therapies in adult practice.
In the pediatric setting, ocrelizumab’s mechanism offers specific theoretical advantages: because POMS is characterized by highly active inflammatory disease, the near-complete B-cell depletion produced by ocrelizumab (blood B-cell counts typically fall to undetectable levels within 2 weeks of the first infusion and remain suppressed for the 24-week dosing interval) may be particularly well-matched to the disease biology. The OPERETTA 2 data tests this hypothesis directly.
The OPERETTA 2 Trial: Full Results
Design
OPERETTA 2 (NCT05123703) was a randomized, double-blind, double-dummy, multicenter Phase 3 noninferiority trial. The double-dummy design means that all patients received both an IV infusion and an oral daily capsule, with one being the active drug and the other a matching placebo, ensuring neither patients nor investigators knew which treatment was assigned.
The trial enrolled 187 pediatric patients aged 10 to 17 years with RRMS, randomized 1:1 to:
- Ocrelizumab 600 mg intravenous infusion every 24 weeks, plus oral placebo daily (n approximately 94)
- Fingolimod 0.5 mg oral capsule daily, plus intravenous placebo infusion every 24 weeks (n approximately 93)
OPERETTA 2 was designed to demonstrate non-inferiority of ocrelizumab to fingolimod. The dose of ocrelizumab (600 mg every 24 weeks) is the same as the approved adult dose, a decision supported by pharmacokinetic and pharmacodynamic data from the companion OPERETTA 1 study that characterized ocrelizumab’s PK profile in the pediatric age range and confirmed that the adult dose produces comparable drug exposure in children aged 10 and older weighing at least 25 kg.
Primary endpoint
| Outcome | Ocrelizumab | Fingolimod | Comparison |
|---|---|---|---|
| Annualized relapse rate (ARR) | Significantly reduced | Reference | Non-inferior (rate ratio 0.52; 95% CI 0.19 to 1.33) |
| Primary non-inferiority endpoint | Met | Reference | p-value consistent with non-inferiority |
MRI endpoints (superiority)
| MRI Outcome | Ocrelizumab | Fingolimod | Comparison |
|---|---|---|---|
| New or enlarging T2 hyperintense lesions per MRI scan | 3.778 | 7.235 | Relative reduction 47.8%; p=0.001 |
| Mean T1 gadolinium-enhancing lesions at week 12 | 0.031 | 0.243 | Relative reduction 87.2%; p=0.001 |
Source: OPERETTA 2 trial, NCT05123703. Genentech/FDA press release, May 8, 2026. Presented at AAN 2026 and published in advance of peer-reviewed journal publication.
Interpreting the results
The primary non-inferiority finding means ocrelizumab reduced annualized relapse rates in a manner that was statistically no worse than fingolimod, the current standard of care for this population. The 95% confidence interval for the rate ratio (0.19 to 1.33) is wide, reflecting the challenge of powering pediatric trials with small populations, but the point estimate (0.52) suggests that relapses were approximately 48% less frequent with ocrelizumab, a numerically superior result that did not reach formal superiority on the relapse endpoint.
The MRI superiority findings are the more clinically discriminating results. A 48% reduction in new or enlarging T2 lesions and an 87% reduction in gadolinium-enhancing lesions versus fingolimod at week 12 are substantial advantages on the imaging markers that most directly reflect ongoing inflammatory disease activity. These MRI findings align with what was observed in adult comparisons of ocrelizumab versus other MS therapies: the anti-CD20 mechanism produces particularly deep suppression of new lesion formation, which correlates with long-term disability protection in adult studies.
Safety in OPERETTA 2
The safety profile of ocrelizumab in pediatric patients in OPERETTA 2 was consistent with its well-established nine-year adult safety record. The most commonly reported adverse events were infusion reactions, infections, and decreases in immunoglobulin levels, identical in type to what is documented in adult trials.
Notably, no adverse events led to treatment withdrawal in the ocrelizumab arm during the double-blind period. This finding on discontinuation due to adverse events is clinically meaningful given that tolerability-driven discontinuation is one of the practical challenges of fingolimod’s first-dose cardiac monitoring requirement and ongoing ophthalmologic surveillance.
MSBase Registry real-world data presented at the 2026 CMSC Annual Meeting further supports the OPERETTA 2 findings: an analysis of pediatric-onset MS patients in the registry showed that ocrelizumab maintained similar effectiveness and safety in pediatric-onset disease compared to young-adult onset disease, providing external validation from clinical practice in countries where ocrelizumab has been used off-label or under compassionate access in pediatric patients.
Ocrevus’s Full Approved Indication Picture After May 2026
With the pediatric RRMS approval, Ocrevus now carries the following FDA-approved indications:
| Indication | Population | Approval date |
|---|---|---|
| Relapsing forms of MS (CIS, RRMS, active SPMS) | Adults | March 2017 |
| Primary progressive MS | Adults | March 2017 |
| RRMS | Pediatric patients aged 10 years and older weighing at least 25 kg | May 8, 2026 |
Ocrevus also has a subcutaneous formulation, Ocrevus Zunovo (ocrelizumab and hyaluronidase-ocsq), approved in September 2024 for adults, which delivers the same dose subcutaneously in 10 minutes rather than the 3.5-hour intravenous infusion. The subcutaneous formulation is currently approved for adults only; the pediatric indication uses the intravenous formulation.
Safety Considerations for the Pediatric Population
The safety profile of ocrelizumab is well-established from more than nine years of adult use and now confirmed in OPERETTA 2 for the pediatric setting. Key considerations for parents and pediatric neurologists:
Infusion reactions: The most common adverse event during ocrelizumab treatment is infusion-related reactions occurring during or within 24 hours of infusion. Pre-medication with corticosteroids, antihistamines, and analgesics is administered before each infusion per protocol. These reactions are typically mild to moderate and manageable.
Infections: Because B-cell depletion reduces one component of humoral immunity, patients on ocrelizumab are at modestly increased risk of respiratory infections, particularly upper respiratory tract infections. Serious infections occurred at low rates in both adult and pediatric trials. Opportunistic infections including PML (caused by JC virus) have been reported rarely in adult patients, primarily in those with additional immunocompromising factors.
Decreasing immunoglobulins: Long-term B-cell depletion leads to gradual decline in IgG and IgM levels over years of treatment. Monitor immunoglobulin levels periodically. Significant hypogammaglobulinemia may require dose adjustment or management in some patients.
Vaccinations: Live vaccines should not be administered during treatment or until B cells have reconstituted after stopping treatment. All recommended immunizations should be completed before initiating Ocrevus. This is particularly important in the pediatric setting where routine childhood vaccination schedules need to be coordinated with treatment initiation.
PML risk: Ocrevus carries a boxed warning for progressive multifocal leukoencephalopathy (PML), though the absolute risk appears substantially lower than with natalizumab (Tysabri). No cases of PML were reported in OPERETTA 2.
Dosing and Administration for Pediatric Patients
| Parameter | Details |
|---|---|
| Approved dose (ages 10 and older, weight at least 25 kg) | 600 mg IV every 24 weeks |
| First dose | Two 300 mg infusions given 2 weeks apart |
| Subsequent doses | Single 600 mg infusion every 24 weeks |
| Pre-medication required | Methylprednisolone (or equivalent corticosteroid) IV, antihistamine, and optional antipyretic before each infusion |
| Infusion duration (600 mg) | Approximately 3.5 hours |
| Setting | Healthcare facility with emergency equipment and resuscitation capability available |
| Weight requirement | At least 25 kg (approximately 55 lbs) |
| Age lower limit | 10 years and older |
| Not for | Children under 10 years of age or weighing less than 25 kg |
What This Approval Means for Families and Pediatric Neurologists
For families of children with RRMS
For the first time, a family whose child has RRMS has a choice between two FDA-approved treatment options rather than only one. Ocrevus, administered every six months as an intravenous infusion, offers a different monitoring profile, mechanism of action, and efficacy signal than daily oral fingolimod.
Practical considerations for families when discussing this option with your child’s neurologist:
- Ocrevus is infused twice a year. Fingolimod is taken daily. For some families, twice-yearly clinic visits for infusion are more manageable than ensuring daily adherence; for others, the infusion schedule is a barrier.
- The first-dose cardiac monitoring requirement with fingolimod is not required with Ocrevus.
- The ophthalmologic monitoring required with fingolimod is not required with Ocrevus.
- The 87% reduction in gadolinium-enhancing lesions at week 12 versus fingolimod in OPERETTA 2 indicates a measurably deeper suppression of active inflammation with Ocrevus in the pediatric trial.
- All immunizations should be current and any live vaccines completed before starting Ocrevus. This timing requires planning with your child’s pediatrician and neurologist.
For pediatric neurologists
OPERETTA 2 provides the first randomized head-to-head controlled evidence comparing a high-efficacy anti-CD20 therapy to fingolimod in pediatric RRMS. The non-inferiority on ARR combined with superiority on both MRI endpoints justifies positioning ocrelizumab as a strong option for treatment-naive patients with active disease, not just as a step-up therapy after fingolimod failure.
The absence of treatment withdrawal due to adverse events in the ocrelizumab arm is a meaningful tolerability signal in a population where treatment persistence over years and decades is the goal. Monitoring requirements for ocrelizumab are primarily infusion reaction surveillance, immunoglobulin levels, and standard infection monitoring, rather than the cardiac and ophthalmologic monitoring that fingolimod requires.
The American Academy of Neurology and the International Pediatric MS Study Group will be updating their guidance frameworks in response to this approval. The National MS Society’s healthcare providers section provides updated clinical resources.
For families: the National MS Society and Can Do MS both maintain dedicated pediatric MS resources. The International Pediatric MS Study Group connects families with specialized clinical expertise.
For related HED coverage of other neurological condition approvals and anti-CD20 therapy advances in 2026, see our post on Fasenra (benralizumab) approved for hypereosinophilic syndrome as another example of a biologic agent expanding from adult to pediatric and rare disease settings, and our post on VYVGART and the first approval covering all forms of myasthenia gravis.
Sources
FDA approval announcement: FDA approves ocrelizumab for relapsing-remitting multiple sclerosis in pediatric patients 10 years of age and older. FDA.gov. May 8, 2026.
Genentech press release: FDA Approves Ocrevus for Relapsing-Remitting Multiple Sclerosis in Pediatric Patients 10 Years of Age and Older. gene.com. May 8, 2026.
Drugs.com approval news: FDA Approves Ocrevus for Relapsing-Remitting Multiple Sclerosis In Pediatric Patients 10 Years of Age and Older. drugs.com. May 2026.
NeurologyLive clinical summary: FDA Approves Ocrelizumab for Pediatric Patients With Relapsing-Remitting Multiple Sclerosis. neurologylive.com. May 2026.
Neurology Advisor detailed coverage: Ocrevus Approved for Pediatric Relapsing-Remitting Multiple Sclerosis. neurologyadvisor.com. May 2026.
Pharmacy Times clinical review: FDA Approves Ocrelizumab for Pediatric Relapsing-Remitting Multiple Sclerosis. pharmacytimes.com. May 2026.
Medscape coverage: FDA Approves Ocrelizumab for Pediatric Relapsing MS. medscape.com. May 2026.
MS News Today coverage: In ‘landmark’ approval, FDA OKs Ocrevus for kids 10 and older with RRMS. multiplesclerosisnewstoday.com. May 2026.
CMSC 2026 real-world data: CMSC 2026: Real-World Analysis Supports Ocrelizumab Use in Pediatric-Onset Multiple Sclerosis. neurologylive.com. May 2026.
Practical Neurology: FDA Approves Ocrevus for Pediatric Relapsing-Remitting MS. practicalneurology.com. May 2026.
OPERETTA 2 trial registration: NCT05123703. ClinicalTrials.gov.
Ocrevus original FDA approval: FDA approves ocrelizumab for multiple sclerosis. FDA.gov. March 2017.
Fingolimod pediatric approval: FDA approves fingolimod for pediatric patients with multiple sclerosis. FDA.gov. 2018.
Ocrevus prescribing information: OCREVUS (ocrelizumab) Prescribing Information. Genentech. 2026.
Ocrelizumab mechanism review: CD20-directed B-cell depleting therapies in MS. PMC6369883.
Pediatric MS StatPearls: Pediatric Multiple Sclerosis. StatPearls. NCBI.
Pediatric MS cognitive effects: Cognitive Impairment in Pediatric Multiple Sclerosis. PMC7897219.
ADCC mechanism: Antibody-Dependent Cell-Mediated Cytotoxicity. StatPearls. NCBI.
National MS Society pediatric resources: Pediatric MS. nationalmssociety.org.
Patient resources: National MS Society: Pediatric MS | International Pediatric MS Study Group | Can Do MS | American Academy of Neurology
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Decisions about MS treatment, including the choice of disease-modifying therapy for pediatric patients, should be made in close consultation with a pediatric neurologist or MS specialist experienced in pediatric-onset multiple sclerosis. |
|---|