
| 📌 The essentials On May 8, 2026, the FDA approved a label expansion for VYVGART (efgartigimod alfa-fcab, IV infusion) and VYVGART Hytrulo (efgartigimod alfa and hyaluronidase-qvfc, subcutaneous injection), making them the first and only FDA-approved treatments for ALL serotypes of adult generalized myasthenia gravis (gMG), including anti-AChR antibody positive (previously covered), anti-MuSK antibody positive (newly covered), anti-LRP4 antibody positive (newly covered, first approved therapy ever for this subtype), and triple seronegative (newly covered, first approved therapy ever for this subtype). The clinical basis: The Phase 3 ADAPT SERON trial (NCT06298552), the largest clinical study ever conducted specifically in seronegative gMG, met its primary endpoint with statistical significance (p=0.0068), showing a mean 3.35-point improvement in the MG-ADL (Activities of Daily Living) score at week 4 compared to placebo. Who this matters most for: The approximately 20% of gMG patients whose antibody tests come back negative, a population that has been systematically excluded from clinical trials and left with no indication-specific approved therapy until today. |
|---|
If you have been diagnosed with myasthenia gravis but your antibody test came back negative, you already know what it means to be told your disease is real while the treatment options designed around your specific diagnosis are not. Until May 8, 2026, no FDA-approved therapy carried an indication that specifically covered your form of the disease. That changed today.
Generalized myasthenia gravis (gMG) is a rare, chronic autoimmune disease of the neuromuscular junction, the connection point between nerve signals and muscle movement. When it malfunctions, the result is debilitating muscle weakness that can affect the ability to breathe, swallow, speak, see clearly, or move. For roughly 80% of patients, the diagnosis is confirmed by a blood test that detects antibodies against the acetylcholine receptor (AChR-Ab). For the remaining 20%, those tests come back negative or detect antibodies against different targets entirely.
That 20% has historically been a clinical blind spot: rarely included in the pivotal trials that generate approved indications, often managed with the same medications as antibody-positive patients but without the evidence base to support that approach formally, and excluded from having a therapy with their specific diagnosis on the label. The May 8 expansion closes that gap.
What Myasthenia Gravis Is and Why Serotype Matters
Myasthenia gravis is caused by pathogenic immunoglobulin G (IgG) antibodies that attack proteins at the neuromuscular junction, disrupting the transmission of nerve signals to muscles. The specific protein being attacked determines the serotype, and different serotypes can produce somewhat different clinical presentations.
| gMG Serotype | Target antibody | Prevalence in gMG | Pre-May 8 approved therapy with specific indication |
|---|---|---|---|
| Anti-AChR antibody positive | Acetylcholine receptor | ~80% of gMG patients | Yes (multiple approved therapies) |
| Anti-MuSK antibody positive | Muscle-specific tyrosine kinase | ~1 to 10% of gMG patients | None specific to this serotype |
| Anti-LRP4 antibody positive | Low-density lipoprotein receptor-related protein 4 | ~1 to 5% of gMG patients | None, ever |
| Triple seronegative | No detectable AChR, MuSK, or LRP4 antibodies | ~10% of gMG patients | None, ever |
The practical implications of serotype extend beyond treatment options. Triple seronegative patients historically have faced a longer and more complicated path to diagnosis because the standard antibody tests that confirm MG in most patients simply don’t help in their case. Diagnosis relies on clinical presentation, electrodiagnostic testing (repetitive nerve stimulation, single-fiber EMG), and expert clinical judgment. This difficulty getting to a confirmed diagnosis is part of why these patients have also been harder to enroll in clinical trials, which has in turn meant fewer trials designed to study them. It is a reinforcing cycle that the ADAPT SERON trial was specifically designed to break.
gMG as a Women’s Health Issue: Why This Approval Matters by Gender
Myasthenia gravis has a bimodal age distribution. In women, it peaks in the third and fourth decades of life, with women under 40 representing the highest-prevalence group in this earlier peak. This matters because the women most likely to be diagnosed with gMG are also in their reproductive years, and the intersection of this disease with pregnancy is clinically significant and underrecognized in mainstream health coverage.
gMG can worsen during pregnancy. The physiological changes of pregnancy, including shifts in immune regulation, can affect disease activity in either direction, but exacerbation during pregnancy is well documented and requires careful co-management with neurology and maternal-fetal medicine. Importantly, gMG can cause neonatal myasthenia gravis in newborns: maternal antibodies cross the placenta and temporarily affect the newborn’s neuromuscular function, causing transient muscle weakness, feeding difficulties, and in severe cases, respiratory compromise. Neonatal MG typically resolves as maternal antibodies are cleared, but it requires neonatal monitoring and sometimes intervention.
For women with seronegative gMG in particular, pregnancy planning has been especially complex because of the lack of approved options with a safety and efficacy record in their specific form of the disease. The VYVGART label includes a pregnancy exposure registry (VYVGARTPregnancy.com, 1-855-272-6524), and the prescribing information notes that it is not known whether VYVGART or VYVGART Hytrulo will harm an unborn baby. This should be a direct conversation between patients and their neurologist before and during pregnancy planning.
For women navigating other autoimmune conditions alongside reproductive health decisions, our post on GLP-1 medications and PCOS fertility research addresses a similar intersection of systemic disease management and reproductive planning.
The Mechanism: What Is an FcRn Blocker and Why Does It Work Across All Serotypes?
To understand why efgartigimod works regardless of which antibody is causing the disease, it helps to understand the biology it targets.
In gMG, the damaging agents are IgG autoantibodies. The specific target those antibodies attack determines the serotype. A drug designed to block AChR-Ab specifically (like eculizumab, which targets complement downstream of AChR-Ab) or MuSK-Ab specifically will only help patients with those particular antibodies. This target-specific approach is why earlier approved therapies couldn’t cover all serotypes: they worked downstream of one antibody type, not upstream of all of them.
Efgartigimod takes a fundamentally different approach. Rather than blocking a specific pathogenic antibody, it reduces the total circulating pool of all IgG antibodies, including the pathogenic ones, regardless of which protein they are targeting.
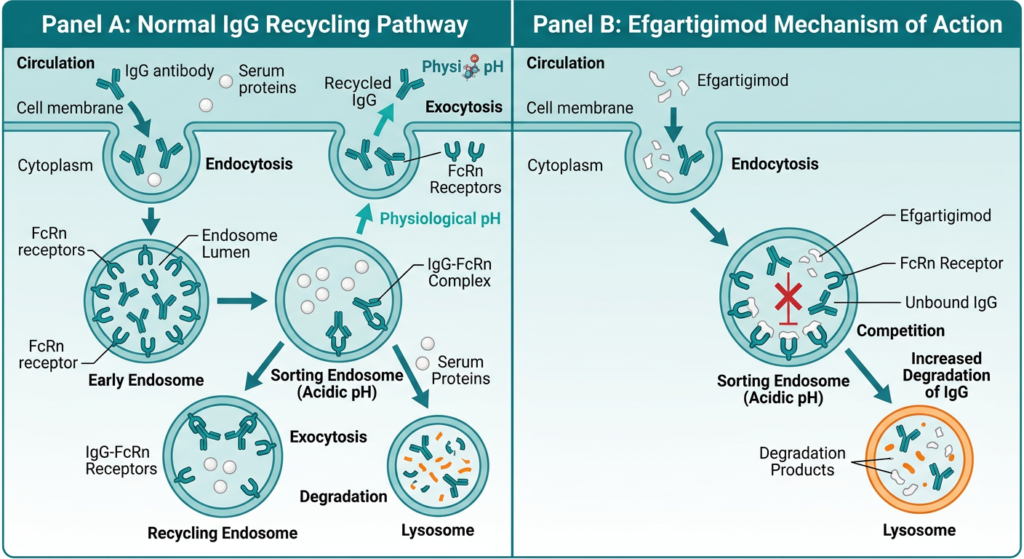
The FcRn pathway
FcRn (neonatal Fc receptor) is a protein expressed in many cell types throughout the body. Its normal function is to protect IgG antibodies from degradation, extending their half-life in circulation. When an IgG antibody is taken up by a cell, FcRn binds to it in the endosome and recycles it back to the cell surface, releasing it back into circulation rather than allowing it to be degraded. This recycling mechanism is why IgG antibodies have such long half-lives compared to other proteins.
Efgartigimod is an engineered fragment of a human IgG1 antibody that binds to FcRn with high affinity. By occupying FcRn, it competes with endogenous IgG antibodies for receptor binding. IgG antibodies that cannot bind FcRn during the recycling process are instead routed to degradation. The result is a significant reduction in total circulating IgG levels, including the pathogenic IgG autoantibodies responsible for gMG across all serotypes.
Because this mechanism does not depend on which specific IgG antibody is causing the disease, it works whether the target is AChR, MuSK, LRP4, or an antibody that hasn’t been identified yet. This is why the ADAPT SERON trial showed improvements across all three previously excluded serotypes, and why the FDA’s label expansion covers all adult gMG patients rather than requiring serotype-specific subgroup analysis to drive the approval.
| How efgartigimod compares mechanistically to other approved gMG treatments Prior to this approval, the main classes of approved or widely used therapies for gMG worked through different and more targeted mechanisms. Acetylcholinesterase inhibitors (pyridostigmine/Mestinon) don’t address the autoimmune cause at all; they work by slowing acetylcholine breakdown at the NMJ to compensate for the reduced receptor availability. Corticosteroids and general immunosuppressants (azathioprine, mycophenolate) broadly suppress the immune system, which reduces antibody production but also carries long-term systemic effects. Complement inhibitors (eculizumab/Soliris, ravulizumab/Ultomiris) target the complement pathway that AChR antibodies activate, which is why they work in anti-AChR positive patients but not in MuSK or seronegative patients, where complement is not the primary mechanism of damage. B-cell depleting therapies (rituximab, used off-label in MuSK-positive disease) work by eliminating the B cells that produce pathogenic antibodies, which can be particularly effective in MuSK-positive disease but requires significant immunosuppression. FcRn blockade with efgartigimod works upstream of all of these mechanisms, directly depleting the pathogenic antibodies themselves rather than compensating for their effects or blocking their downstream consequences. |
|---|
The ADAPT SERON Trial: What the Evidence Shows
Trial design
ADAPT SERON (NCT06298552) was a randomized, double-blind, placebo-controlled, multicenter Phase 3 study, conducted across North America, Europe, China, and the Middle East. It enrolled 119 adults with anti-AChR antibody negative gMG, spanning all three seronegative serotypes: anti-MuSK antibody positive, anti-LRP4 antibody positive, and triple seronegative.
This was the largest clinical trial ever conducted specifically in seronegative gMG. Every enrolled participant had a confirmed MG diagnosis verified by an independent panel of experts and an MG-ADL total score of 5 or higher at enrollment, indicating meaningful functional impairment. Participants were on stable background therapy prior to randomization, including acetylcholinesterase inhibitors, corticosteroids, or other immunosuppressive drugs.
Part A of the study randomized participants 1:1 to receive either 4 once-weekly IV infusions of efgartigimod or placebo, followed by a 5-week follow-up period. The primary endpoint was the change in MG-ADL total score from baseline to week 4 (day 29) in Part A. Part B is an open-label extension in which participants receive ongoing efgartigimod cycles with cycle initiation guided by clinical status from cycle 3 onward.
What the MG-ADL score measures
The MG-ADL (Myasthenia Gravis Activities of Daily Living) scale is an 8-item validated measure of the functional impact of myasthenia gravis symptoms on daily life. It evaluates: talking, chewing, swallowing, breathing, brushing teeth or combing hair, arising from a chair, double vision, and drooping eyelids. Each item is scored 0 to 3, with higher scores indicating greater impairment. A total score of 5 or higher at baseline indicates meaningful functional impairment. A reduction of 2 or more points is generally considered clinically meaningful.
Results
| Outcome | Efgartigimod (VYVGART) | Placebo |
|---|---|---|
| Primary endpoint met | Yes (p=0.0068) | Reference |
| Mean change in MG-ADL at week 4 | 3.35-point improvement | Less than efgartigimod arm |
| Meaningful improvements across serotypes | Yes, all three: anti-MuSK, anti-LRP4, triple seronegative | — |
| QMG score improvement | Yes (Quantitative Myasthenia Gravis scale) | — |
| Sustained improvements through subsequent cycles | Yes, observed in Part B (open-label extension) | — |
| Safety profile | Consistent with established efgartigimod profile | — |
| New safety signals | None identified | — |
Source: ADAPT SERON, NCT06298552. argenx press release, May 8, 2026. Presented at the 2026 MDA Clinical and Scientific Conference.
A 3.35-point improvement on the MG-ADL scale is clinically meaningful. To put that in concrete terms: it represents measurable improvement across the specific tasks, breathing, swallowing, speaking, seeing clearly, and performing basic physical movements, that gMG takes away from patients. In a population that had no indication-specific approved therapy before today, this result represents the first formal evidence of efficacy derived from a study built specifically around their diagnosis.
The improvement was observed across all three serotypes studied, which is the key finding from a regulatory standpoint. The FDA’s label expansion to cover all seronegative gMG is grounded in subgroup consistency: anti-MuSK, anti-LRP4, and triple seronegative patients all showed benefit in ADAPT SERON.
Safety: What Patients and Providers Need to Know
The safety profile in ADAPT SERON was consistent with efgartigimod’s established profile from prior trials in anti-AChR positive gMG and from its existing approvals for gMG and CIDP. No new safety signals were identified.
The most common adverse effects of VYVGART and VYVGART Hytrulo include:
- Respiratory tract infection
- Headache
- Urinary tract infection
- Injection site reactions (VYVGART Hytrulo only)
Important safety considerations from the prescribing information:
- Infection risk: Because efgartigimod reduces total IgG levels (not just pathogenic antibodies), it also reduces some of the IgG antibodies that contribute to normal immune defense. Providers should delay treatment if a patient has an active infection. Patients should report any signs of infection promptly.
- Allergic reactions: Serious hypersensitivity reactions can occur during or after infusion or injection. Patients should be monitored accordingly.
- Infusion/injection-related reactions: Including elevated blood pressure, chills, and chest or back pain. These can occur during or shortly after administration.
- Vaccinations: Live vaccines should be avoided during treatment. Discuss vaccination timing with your neurologist.
- Pregnancy: Safety in pregnancy is not established. A pregnancy exposure registry is available at VYVGARTPregnancy.com or by calling 1-855-272-6524.
The full prescribing information for VYVGART and VYVGART Hytrulo is available through the FDA.
Two Administration Options: IV Infusion and Subcutaneous Injection
One practical note for patients navigating the treatment decision is that efgartigimod is now available in two administration formats, which differ in setting and convenience.
VYVGART (IV infusion): Administered intravenously in a clinical setting (infusion center or office). Each treatment cycle consists of 4 once-weekly infusions, approximately one hour per infusion.
VYVGART Hytrulo (subcutaneous injection): Administered as a subcutaneous injection, which can be self-administered at home with a prefilled syringe. This option uses Halozyme’s ENHANZE drug delivery technology to allow subcutaneous delivery of the same efgartigimod. For patients who prefer to avoid the infusion center setting, this represents a meaningful quality-of-life difference.
Both formulations are now approved for all adult gMG serotypes. The choice between them is made with a treating neurologist based on patient preference, access, and clinical circumstances.
The Equity Dimension: Why a Trial Built Around Seronegative Patients Matters
The structural problem that ADAPT SERON addressed is worth naming plainly. For decades, the way pivotal gMG trials were designed reflected and reinforced the treatment gap. Enrollment criteria typically required detectable anti-AChR antibodies for confirmation of diagnosis. This made sense from a scientific standpoint at the time: it reduced diagnostic uncertainty and created a more homogeneous trial population. But the effect was that seronegative patients, who make up roughly 20% of gMG cases and share the same debilitating disease, were systematically excluded from the evidence base that generated approved indications.
The consequence is not abstract. An FDA approval requires indication-specific evidence. Without trials that enrolled seronegative patients, no drug could carry an indication specific to their form of the disease. Without an indication, prescribing for this population operated in a gray zone, even when the same drugs were being used. For triple seronegative patients in particular, no approved drug had ever been studied or indicated specifically for them before today.
ADAPT SERON was built from the ground up to generate that evidence. The result is not just a label expansion for one drug. It is the first Phase 3 clinical evidence generated specifically for this population that has successfully supported FDA approval.
What Patients With gMG Should Know Right Now
If you have been diagnosed with gMG and your serotype is MuSK-positive, LRP4-positive, or triple seronegative
VYVGART and VYVGART Hytrulo are now FDA-approved for your specific serotype. This means they can be prescribed by your treating neurologist with an approved indication covering your diagnosis. The label expansion took effect May 8, 2026. Talk to your neurologist about whether this treatment is appropriate for your situation, including your current medication regimen, your disease activity, and whether the IV or subcutaneous administration option is a better fit for your circumstances.
If your antibody status is unknown or your diagnosis has not been fully characterized serologically
The expanded label means that clinicians can now prescribe efgartigimod based on a confirmed gMG diagnosis without requiring full serological characterization first. If your diagnosis has not included complete antibody testing (AChR, MuSK, and LRP4), discuss with your neurologist whether additional testing would be informative for your treatment planning.
Insurance coverage and access
Coverage decisions by insurers typically follow FDA approvals for rare disease treatments, but prior authorization requirements can create delays. The argenx patient support program, My VYVGART Path, provides access support, benefits verification, and financial assistance for eligible patients. More information is available at VYVGART.com.
For patients without insurance or with limited coverage, discuss options with your treatment center’s patient services team and review the argenx access support resources.
Finding a specialist
gMG is a rare disease and is ideally managed by or in consultation with a neurologist with expertise in neuromuscular disease. The Myasthenia Gravis Foundation of America (MGFA) maintains a physician directory and patient resources. The Muscular Dystrophy Association (MDA) also provides care resources, including MDA Care Centers with neuromuscular specialists. The National Organization for Rare Disorders (NORD) maintains a patient-facing overview of the disease and available resources.
Sources
argenx FDA approval press release: argenx Announces U.S. FDA Approval Expanding VYVGART and VYVGART Hytrulo for Use in All Adult Patients Living with gMG. GlobeNewswire. May 8, 2026.
MDA welcome statement: FDA Expands Approval of VYVGART and VYVGART Hytrulo to All Adults Living with Generalized Myasthenia Gravis. Muscular Dystrophy Association. May 8, 2026.
ADAPT SERON trial registration: NCT06298552. ClinicalTrials.gov.
NeurologyLive sBLA coverage: sBLA Acceptance Positions Efgartigimod as Potential First Therapy for Seronegative Myasthenia Gravis. NeurologyLive. February 2026.
Clinical Trial Vanguard analysis: FDA Expands Efgartigimod Approval to All Adult Generalized Myasthenia Gravis Patients. clinicaltrialvanguard.com. May 8, 2026.
FcRn biology: The neonatal Fc receptor (FcRn): a misnomer? PMC7211387.
MG-ADL scale reference: Validation of the MG-ADL scale. PMC6527389.
Neonatal myasthenia gravis: Neonatal Myasthenia Gravis. StatPearls. NCBI.
NINDS gMG overview: Myasthenia Gravis. National Institute of Neurological Disorders and Stroke.
MGFA patient resources: Myasthenia Gravis Foundation of America.
Patient resources: MGFA | MDA | NORD | VYVGART.com | VYVGARTPregnancy.com
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes only. Nothing on this site constitutes medical advice, diagnosis, or treatment. Decisions about myasthenia gravis treatment, including whether efgartigimod (VYVGART/VYVGART Hytrulo) is appropriate for your situation, should be made in consultation with a qualified neurologist or neuromuscular disease specialist who can evaluate your individual diagnosis, serotype, and treatment history. |
|---|