| 📌 The essentials On April 16, 2026, the FDA cleared the ExaStim Stimulation System (ANEUVO) for use in the United States, marking the first FDA-cleared transcutaneous spinal cord stimulation device for home use in adults with incomplete spinal cord injury. Important terminology: this is an FDA 510(k) clearance, not a drug approval. The distinction matters and is explained below. What ExaStim is cleared for: improving hand sensation and strength in adults aged 18 to 75 with chronic, non-progressive neurological deficits resulting from incomplete spinal cord injury, when used in conjunction with functional task practice. Where it can be used: both clinical settings and at home, under a prescribing clinician’s supervision. The regulatory basis: ExaStim received FDA Breakthrough Device Designation, completed the ASPIRE clinical study at the Kennedy Krieger Institute and other sites, and received CE Mark certification in Europe in April 2025 before U.S. clearance. The broader context: ExaStim is entering a real but still-developing evidence base for transcutaneous spinal cord stimulation. What the clinical data shows, where it is strongest, and where legitimate gaps remain is what this post covers. |
|---|
Spinal cord injury (SCI) affects approximately 18,000 Americans each year and an estimated 302,000 people currently live with SCI in the United States. The consequences are not uniform. About 69% of new SCI cases are classified as incomplete, meaning some neural pathways across the injury site are preserved, and some degree of function below the level of injury remains possible. For people with cervical incomplete SCI specifically, the loss of hand and arm function is consistently ranked as the highest priority for recovery, above walking. Being able to hold a cup. Press a button. Open a door independently. These are not small things.
The standard rehabilitation toolkit for incomplete SCI, including physical therapy, occupational therapy, and conventional functional electrical stimulation, produces meaningful but limited gains for many patients. A growing body of research has been investigating whether non-invasive electrical stimulation of the spinal cord itself, delivered through electrodes placed on the skin rather than surgically implanted, can amplify the nervous system’s own residual capacity for recovery.
The FDA’s April 16 clearance of the ExaStim Stimulation System from ANEUVO represents the first time a transcutaneous spinal cord stimulation device has been cleared specifically for at-home use in incomplete SCI in the United States. This post covers what the device is, how it works, what the clinical evidence actually shows about transcutaneous spinal stimulation as a treatment class, what the ASPIRE study contributed, and what this clearance does and does not mean for patients navigating SCI rehabilitation.
What Is Transcutaneous Spinal Cord Stimulation and Why Is It Relevant to SCI?
To understand what ExaStim does, it helps to understand what happens at the neuromuscular level in incomplete spinal cord injury and why spinal stimulation might influence it.
The injured spinal cord is not simply broken
In a complete SCI, the neural pathways crossing the injury site are entirely severed, and no voluntary signal from the brain reaches muscles below the injury. In an incomplete SCI, some pathways remain partially intact. But “partially intact” does not mean “working normally.” The surviving connections often cannot generate sufficient neural drive on their own to produce coordinated voluntary movement. The circuits exist, but they are not generating enough signal to translate into function.
Neuroplasticity, the nervous system’s capacity to reorganize and strengthen connections through activity-based learning, is a central principle of SCI rehabilitation. The more consistently neural circuits are activated, the more the nervous system can reinforce and strengthen those connections over time. This is why task-specific training, where you practice the actual functional movement you are trying to recover, tends to outperform generalized exercise in SCI rehabilitation.
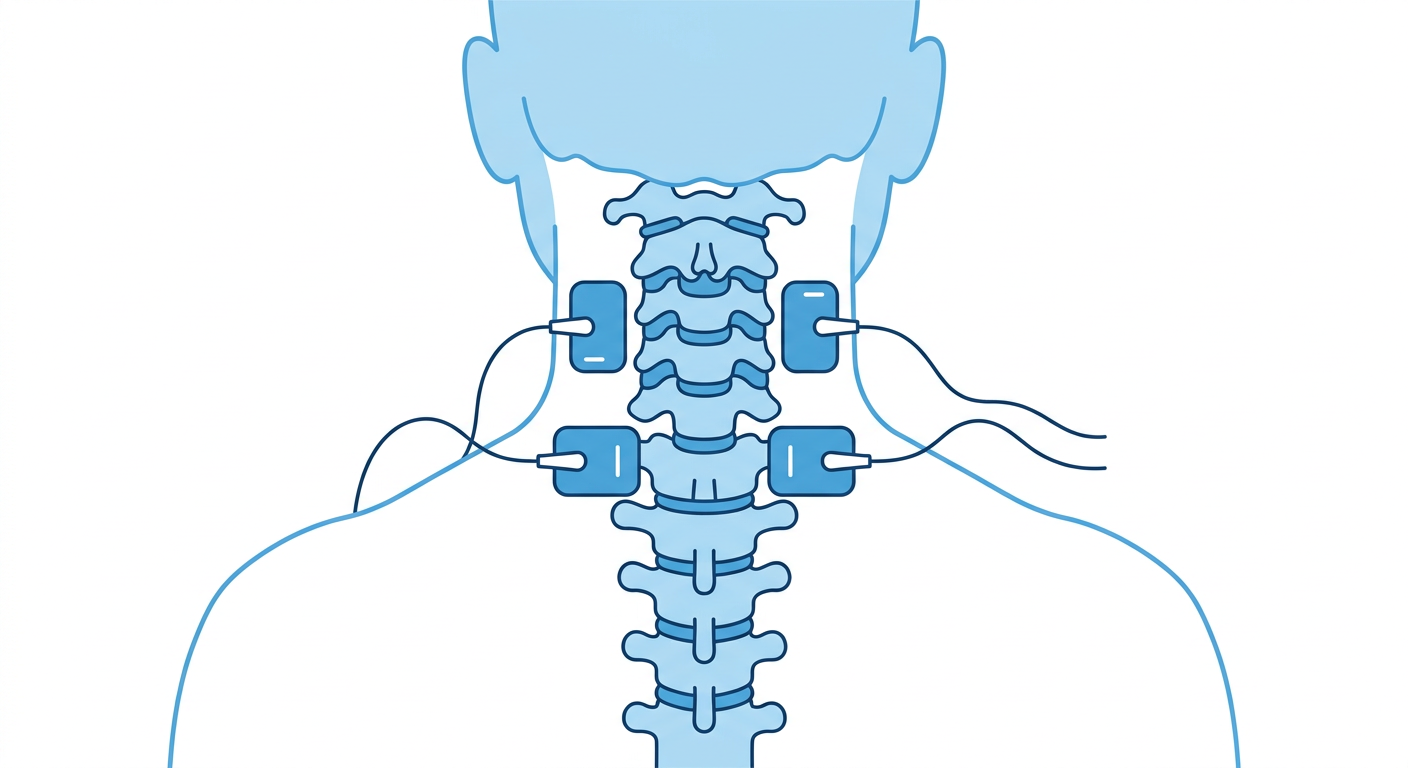
Transcutaneous spinal cord stimulation (tSCS) delivers low-level electrical current through electrodes placed on the skin over the spinal cord, at the level corresponding to the neural circuits being targeted. For upper extremity function in cervical SCI, electrodes are typically placed at the cervical spinal level, approximately C4 to C7. The proposed mechanism is that tSCS increases the excitability of surviving neural pathways and the motor neuron pools they connect to, making it easier for the brain’s residual descending signals to produce muscle activity. In effect, it lowers the threshold for the injured circuits to fire, potentially unlocking function that exists but cannot be accessed without facilitation.
What distinguishes ExaStim within the tSCS category
ExaStim uses a multi-electrode array rather than the single-pair electrode configurations used in earlier-generation tSCS research. This matters because different muscle groups in the arm and hand are controlled by different spinal cord segments and fiber pathways. A multi-electrode system allows the stimulation to be spatially targeted and the parameters personalized to an individual patient’s injury level, neurological profile, and therapy goals, rather than delivering a single undifferentiated current across the whole area. The system is controlled via a mobile digital device, enabling flexible parameter adjustment in clinical and home settings.
ExaStim received FDA Breakthrough Device Designation, a designation reserved for devices that provide more effective treatment or diagnosis of a serious condition compared to available options and where no approved alternative exists. This designation preceded the FDA clearance and provided an expedited review pathway.
The Regulatory Distinction: Clearance Versus Approval
The original post on this site described ExaStim as “approved,” which is not technically accurate and is worth correcting explicitly. This distinction matters on a health evidence site.
FDA clearance (510(k)) means the FDA has determined that a device is substantially equivalent to a legally marketed predicate device in terms of its intended use and technological characteristics. It is the standard pathway for medical devices. The clearance process does not require the same level of randomized controlled trial evidence as a drug approval. It requires demonstration of safety and effectiveness sufficient to establish substantial equivalence.
FDA approval (PMA or BLA) is the more rigorous pathway used for higher-risk devices or drugs, requiring independent demonstration of safety and effectiveness through controlled clinical trials.
ExaStim was cleared through the 510(k) pathway. This is normal and appropriate for this category of device. It does not mean the device lacks evidence. It means the evidence standard is different from what would be required for a drug approval. The distinction is important for patients and clinicians evaluating the strength of the regulatory basis.
What the Evidence Shows: The Broader tSCS Literature
ExaStim’s clearance builds on a growing but still-developing body of research on transcutaneous spinal cord stimulation for SCI. The most important thing to understand about this evidence base is where it is genuinely strong and where gaps remain.
What the peer-reviewed literature shows
A 2024 meta-analysis published in Neurorehabilitation and Neural Repair pooled results from six randomized controlled trials of transcutaneous spinal cord stimulation in SCI patients. The analysis found that tSCS combined with conventional rehabilitation significantly improved limb strength (mean difference 4.82, p=0.004) and reduced spasticity (MD 0.40, p=0.02) compared to conventional rehabilitation alone. Walking speed and distance also improved significantly. The upper-extremity motor function composite endpoint did not reach statistical significance in this specific pooled analysis (p=0.75), though individual studies have shown gains in grip strength and hand function.
A 2024 review published in the Journal of Neurotrauma examining transcutaneous stimulation specifically for upper extremity function in cervical SCI reviewed studies involving 55 participants across multiple research groups. The review found that tSCS combined with task-specific training “consistently improved voluntary control of arm and hand function and sensation,” though noting the studies were limited in number and sample size.
A 2026 systematic review in Life covering cervical spinal cord stimulation through July 2025, including epidural, intraspinal, and transcutaneous approaches, synthesized preclinical and clinical evidence and found consistent evidence of functional improvement across approaches, while noting substantial heterogeneity across study designs that precluded meta-analysis of the combined dataset.
A systematic review in PMC covering electrical stimulation modalities for motor recovery in SCI synthesized 37 clinical trials and found consistent evidence of functional improvement, with transcutaneous approaches showing promise as a non-invasive alternative to epidural stimulation.
| What the evidence supports and what it does not yet confirm The evidence for transcutaneous spinal cord stimulation in incomplete SCI supports the following conclusions: tSCS combined with task-specific training improves motor neuron excitability and can augment voluntary movement in incomplete SCI. Limb strength and spasticity improvements are the most consistently demonstrated outcomes across RCTs. Hand and upper extremity function improvements have been shown in multiple studies, though the evidence base here is smaller and more heterogeneous than for lower extremity outcomes. The technology is safe and well-tolerated based on available data, with no major safety signals identified across the clinical trial literature. What the evidence does not yet confirm: long-term durability of functional gains after treatment ends, optimal stimulation parameters (frequency, intensity, electrode placement) for different injury levels and patient profiles, whether benefits generalize across the full spectrum of incomplete SCI severity, and how ExaStim’s specific multi-electrode platform compares to single-electrode systems used in most published research. These are legitimate open questions that the post-clearance clinical data and the ASPIRE long-term follow-up will need to address. |
|---|
The ASPIRE Study: ANEUVO’s Foundational Clinical Evidence
The ASPIRE (Assessing non-invasive spinal Stimulation and PT/OT for motor Improvement Response with ExaStim) study was ANEUVO’s registrational clinical program, conducted at the International Center for Spinal Cord Injury at Kennedy Krieger Institute, affiliated with Johns Hopkins University School of Medicine, and at additional sites across the United States.
The study enrolled adults with upper extremity paralysis due to chronic, traumatic incomplete SCI. Participants received ExaStim tSCS therapy in combination with traditional physical and occupational therapy (PT/OT) rehabilitation as an adjunct treatment. The FDA designated the study as non-significant risk (NSR), meaning the agency determined that the risk profile did not warrant the oversight requirements applied to significant-risk device studies.
ANEUVO completed the ASPIRE study and has stated that results will be shared in early 2026. The full peer-reviewed publication of ASPIRE data has not yet been publicly available at the time of this post. The clearance was supported by the ASPIRE dataset alongside the preceding pilot study and the broader tSCS literature.
The pilot study that preceded ASPIRE, published in the Archives of Physical Medicine and Rehabilitation in 2023, evaluated ExaStim in a small group of participants with incomplete SCI and found preliminary evidence of treatment safety and possible effectiveness in improving upper limb function. The authors, who included both ANEUVO employees and independently funded investigators, noted that further investigation in a larger trial was warranted, which the ASPIRE study was designed to provide.
Important disclosure context: Several investigators in the ExaStim research program, including the ASPIRE principal investigator Dr. Rebecca Martin and others, received research funding from ANEUVO. Dr. Yi-Kai Lo and Rachel Yung are ANEUVO employees. This does not invalidate the research, but it is relevant context for interpreting company-funded data pending independent replication.
What FDA Clearance for Home Use Means in Practice
The clearance of ExaStim for both clinical and at-home use is notable. Most rehabilitation neurostimulation devices are limited to clinical or supervised settings. ExaStim’s home-use clearance means that once prescribed by a clinician, patients can continue therapy in their own home environment, extending the treatment dose beyond what clinic visits alone allow.
This matters because neuroplasticity-based rehabilitation for SCI appears to be dose-dependent: more frequent, consistent activation of the target neural circuits tends to produce better outcomes. Clinic-only therapy typically means two to three sessions per week. Home use could mean daily therapy, compressing the treatment timeline and potentially improving outcomes.
The practical requirements for home use include:
- The device must be prescribed by a qualified clinician
- Initial setup, parameter programming, and training occur in a clinical setting
- Patients must be trained on electrode placement, device operation, and recognition of adverse effects
- Ongoing clinical oversight continues throughout the home therapy period
- The therapy is used in conjunction with functional task practice, not as a standalone intervention
The home-use clearance also has implications for access. Clinic-based rehabilitation is limited by geography, transportation, and appointment availability. For patients in rural or underserved areas, a home-based tSCS system potentially removes a significant logistical barrier to consistent rehabilitation. Whether insurance coverage follows the clearance is a separate and clinically important question. Home medical device coverage under Medicare, Medicaid, and private insurance for novel neuromodulation systems varies and requires prior authorization. Clinicians prescribing ExaStim should be prepared to support patients through the coverage determination process.
Where ExaStim Fits in the SCI Rehabilitation Landscape
Spinal cord injury rehabilitation encompasses a wide range of interventions. Here is where transcutaneous spinal cord stimulation, and ExaStim specifically, sits relative to other approaches:
| Approach | How it works | FDA status | Evidence level |
|---|---|---|---|
| Physical and occupational therapy | Task-specific training, strength, and function | Standard of care, no device clearance needed | Strong; foundational |
| Functional electrical stimulation (FES) | Stimulates peripheral nerves/muscles directly to produce movement | Multiple FDA-cleared devices exist | Established; strongest for lower extremity |
| Epidural spinal cord stimulation | Surgically implanted electrodes deliver continuous or patterned stimulation to dorsal spinal cord | FDA cleared/approved for pain; investigational for SCI motor function | Growing; invasive |
| Transcutaneous spinal cord stimulation (tSCS) | Non-invasive surface electrodes deliver stimulation to spinal cord | ExaStim now FDA-cleared for incomplete SCI upper extremity | Emerging; consistent signals, limited large RCTs |
| Robotic exoskeletons | Mechanically assisted movement training | Multiple FDA-cleared devices | Established for gait training |
ExaStim is positioned as an adjunct to, not a replacement for, physical and occupational therapy. The clearance language requires its use “in conjunction with functional task practice,” which is consistent with how tSCS has been used across the clinical trial literature and with the neuroplasticity rationale for the therapy.
What This Means for Patients and Clinicians
For patients with incomplete cervical SCI and their families

The ExaStim clearance represents a genuine expansion of the non-invasive rehabilitation toolkit. The device is the first of its kind cleared for home use in the United States, and the clinical evidence for tSCS as a class supports cautious optimism for upper extremity functional gains when combined with task-specific therapy.
What to realistically expect: ExaStim is a rehabilitation adjunct. It is designed to improve outcomes when used alongside physical and occupational therapy, not to produce dramatic recovery on its own. The evidence base shows meaningful improvements in grip strength and upper extremity function in incomplete SCI patients, with a good safety profile. The magnitude and durability of individual outcomes will vary.
What to discuss with your rehabilitation team: whether the degree of incompleteness and level of your injury makes you a candidate for upper extremity tSCS therapy; how ExaStim compares to other FES and neurostimulation devices your team has experience with; what the coverage situation is for your specific insurance; and how home-based ExaStim therapy would be integrated with your current PT/OT program.
The Christopher and Dana Reeve Foundation and the United Spinal Association both maintain current, clinician-reviewed resources on rehabilitation options for SCI. The Model Systems Knowledge Translation Center at the University of Washington maintains evidence-based SCI rehabilitation guides for patients and families. Clinical trials evaluating transcutaneous spinal cord stimulation can be found at ClinicalTrials.gov.
For rehabilitation clinicians
ExaStim’s clearance for home use creates a new prescribing and follow-up responsibility. The device integrates with a mobile platform for parameter management. ANEUVO is building out its clinical partnership program, and training and onboarding support is available through the company. Given that the ASPIRE full dataset has not yet been peer-reviewed and published, clinicians should follow the literature for independent replication of the company-funded results as they become available.
The tSCS class as a whole has a favorable safety profile across the published literature. The main clinical considerations for patient selection are injury completeness level (incomplete is required; complete injury is outside the cleared indication), chronicity of injury, and upper extremity functional baseline. Patients with implanted electronic devices (pacemakers, deep brain stimulators) are generally not candidates for transcutaneous spinal stimulation.
Sources
ANEUVO FDA clearance press release: ANEUVO Receives FDA Clearance for ExaStim Stimulation System. GlobeNewswire. April 16, 2026.
ASPIRE clinical study registration: NCT05294237. ClinicalTrials.gov.
ExaStim pilot study: Lo YK et al. A Pilot Study Using ExaStim to Restore Upper Limb Function After Spinal Cord Injury. Archives of Physical Medicine and Rehabilitation. 2023.
2024 tSCS meta-analysis: Shi C et al. Transcutaneous spinal cord stimulation on motor function in patients with spinal cord injury: A meta-analysis. Neurorehabilitation and Neural Repair. 2024.
2024 cervical SCI upper extremity review: Singh G et al. Spinal Cord Transcutaneous Stimulation in Cervical Spinal Cord Injury: A Review Examining Upper Extremity Neuromotor Control, Recovery Mechanisms, and Future Directions. Journal of Neurotrauma. 2024.
2026 systematic review cervical SCS: Cervical Spinal Cord Stimulation for Functional Rehabilitation After Spinal Cord Injury: A Systematic Review. Life. 2026;16(1):179.
Electrical stimulation systematic review (PMC): Electrical Stimulation and Motor Function Rehabilitation in Spinal Cord Injury: A Systematic Review. PMC11214755.
SCI statistics: National Spinal Cord Injury Statistical Center. Facts and Figures 2023.
FDA 510(k) clearance explained: Premarket Notification 510(k). FDA.gov.
FDA Breakthrough Device Designation: Breakthrough Device Program. FDA.gov.
Patient resources: Christopher and Dana Reeve Foundation | United Spinal Association | Model Systems Knowledge Translation Center | ClinicalTrials.gov: SCI transcutaneous stimulation
| Disclaimer: Health Evidence Digest provides general information about FDA clearances and health research for educational purposes. This content is not a substitute for professional medical advice. ExaStim was cleared through the FDA’s 510(k) pathway. Decisions about rehabilitation technology and treatment approaches for spinal cord injury should be made in consultation with a qualified physiatrist, physical therapist, or occupational therapist experienced in SCI rehabilitation. |
|---|
Leave a Reply