
| 📌 The essentials Drug: Beqalzi (sonrotoclax) — a next-generation, highly selective BCL-2 inhibitor. FDA approval type: Accelerated approval on May 13, 2026. Continued approval may depend on confirmatory clinical trial results. Developer: BeOne Medicines USA, Inc. (formerly BeiGene). Indication: Adults with relapsed or refractory mantle cell lymphoma (MCL) after at least two prior lines of systemic therapy, including a Bruton’s tyrosine kinase (BTK) inhibitor. What makes it first-in-class: First and only BCL-2 inhibitor specifically approved for MCL. Venetoclax (Venclexta) is approved for CLL and AML but not MCL. Key trial results (BGB-11417-201, n=103): ORR 52% (95% CI 42–62%), median duration of response 15.8 months, median time to response 1.9 months. Dosing: Oral tablet, once daily with food, following a 4-week dose ramp-up schedule. Target dose: 320 mg once daily. Critical warning: Tumor lysis syndrome (TLS) — potentially life-threatening. Requires risk assessment, prophylaxis, and close monitoring throughout the ramp-up phase. Regulatory designations: Breakthrough Therapy, Fast Track, Orphan Drug, Priority Review. Reviewed under Project Orbis. |
Mantle cell lymphoma does not follow the forgiving course of many lymphoma subtypes. It is aggressive. It responds to first-line therapy in many patients, but it almost always comes back. After a first relapse on BTK inhibitor therapy, which has been the most important treatment advance in MCL over the past decade, options narrow considerably. Response rates with available agents are often modest. Duration of response can be brief. A population of patients with limited alternatives and deteriorating disease has been waiting for something new to try.
On May 13, 2026, the FDA granted accelerated approval to Beqalzi (sonrotoclax) for adults with relapsed or refractory MCL after at least two prior lines of therapy including a BTK inhibitor. Beqalzi is a BCL-2 inhibitor, and it is the first drug in that class specifically approved for mantle cell lymphoma. The pivotal trial in 103 patients showed a 52% overall response rate and a median duration of response of 15.8 months, with a notably high response rate in TP53-mutant patients who typically fare poorly with existing options.
Mantle Cell Lymphoma: Why Post-BTK Relapse Is Such a Difficult Problem
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma that originates in the mantle zone of the lymph node. It accounts for approximately 5% of non-Hodgkin lymphoma cases globally, with roughly 3,300 new diagnoses annually in the United States. The median age at diagnosis is approximately 65, and the disease is more common in men.
MCL is characterized biologically by the t(11;14) chromosomal translocation, which places the CCND1 gene encoding cyclin D1 under the control of an immunoglobulin heavy chain promoter, driving overexpression of cyclin D1 and uncontrolled cell proliferation. Most MCL tumors also dysregulate the BCL-2 anti-apoptotic pathway, which helps cancer cells survive even when they should die. These two biological features, the proliferative driver and the survival mechanism, are both targets for therapy.
BTK inhibitors (ibrutinib, acalabrutinib, zanubrutinib) transformed the treatment of MCL at first and second relapse, producing high response rates in the 70-80% range. But responses are not permanent. Most patients eventually progress on BTK inhibitor therapy. At that point, the disease has developed resistance mechanisms, the patient has typically accumulated treatment-related organ stress, and available next-line options have produced response rates in the 20-40% range with short durations.
| TP53 mutations: the highest-risk subgroup in MCL TP53 encodes p53, the tumor suppressor protein that normally triggers cell death when DNA damage occurs. TP53 mutations are present in approximately 20–30% of MCL patients and are strongly associated with chemotherapy resistance, shorter remission durations, and worse overall survival. Patients with TP53-mutant MCL represent one of the highest-unmet-need populations in hematologic oncology. Standard chemotherapy regimens, which work partly through DNA damage that requires functional p53 to trigger apoptosis, are less effective when p53 is mutated. In the BGB-11417-201 trial supporting Beqalzi’s approval, the TP53-mutant subgroup achieved an ORR of 59.1%, numerically higher than the 52% overall population response rate. This is the opposite of what is typically seen with chemotherapy-based regimens in this subgroup, and it supports the mechanistic hypothesis that BCL-2 inhibition can bypass p53-dependent pathways to induce cancer cell death. |
How BCL-2 Inhibition Works and What Makes Sonrotoclax Different from Venetoclax
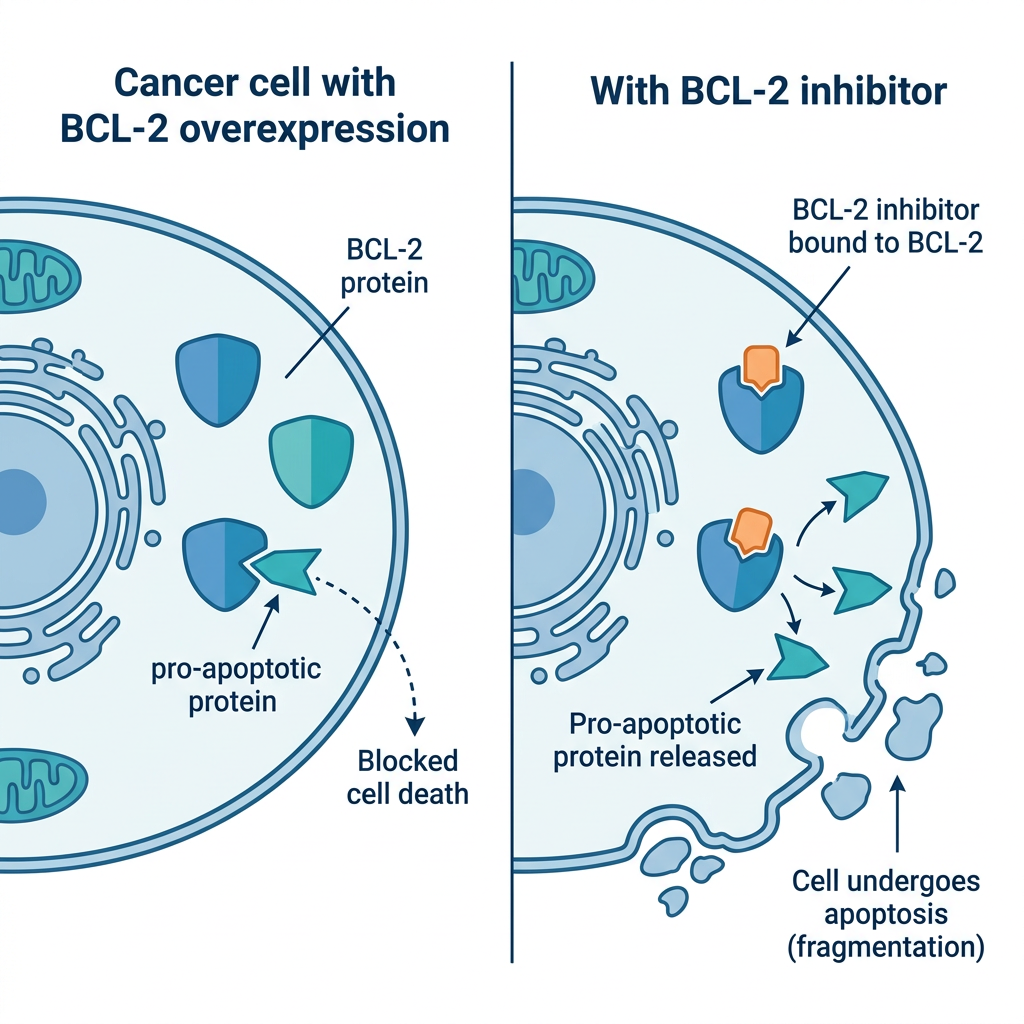
BCL-2 (B-cell lymphoma 2) is a protein that promotes cell survival by blocking apoptosis, the programmed cell death process that the body uses to eliminate damaged, aged, or abnormal cells. In normal cells, BCL-2 is part of a balanced system of pro- and anti-apoptotic proteins. In many B-cell malignancies, BCL-2 is overexpressed, tipping the balance toward survival and allowing cancer cells to accumulate rather than die.
BCL-2 inhibitors work by occupying the BH3-binding groove of the BCL-2 protein and displacing the pro-apoptotic proteins it normally sequesters. When these pro-apoptotic proteins are released, they activate the mitochondrial apoptosis cascade, triggering cell death. This mechanism is independent of TP53 function, which explains why BCL-2 inhibitors can be active in TP53-mutant tumors that resist DNA-damaging chemotherapy.
Sonrotoclax versus venetoclax
Venetoclax (Venclexta) is the established BCL-2 inhibitor in the market, approved for chronic lymphocytic leukemia (CLL) and acute myeloid leukemia (AML). It has been used off-label in MCL with modest activity. Sonrotoclax was engineered with greater potency and selectivity for BCL-2 compared to venetoclax, targeting BCL-2 more precisely while having less activity against the related BCL-XL protein.
| Feature | Sonrotoclax (Beqalzi) | Venetoclax (Venclexta) |
| BCL-2 selectivity | Higher selectivity for BCL-2; reduced BCL-XL activity | BCL-2 selective; BCL-XL activity also noted |
| FDA-approved for MCL | Yes — May 13, 2026 (accelerated) | No — approved for CLL and AML only |
| Approved indications | R/R MCL after ≥2 lines including BTK inhibitor | CLL (with obinutuzumab or ibrutinib), R/R AML (with azacitidine or decitabine) |
| Target dose | 320 mg once daily (after 4-week ramp-up) | 400 mg once daily (after 5-week ramp-up for CLL) |
| Tumor lysis syndrome risk | Yes — requires ramp-up and prophylaxis | Yes — requires ramp-up and prophylaxis |
| Route | Oral, once daily with food | Oral, once daily with food |
The BGB-11417-201 Trial: Design and Results
Trial design
BGB-11417-201 (NCT05471843) is a single-arm, multicenter, open-label Phase 1/2 trial. Part 1 established the safety, tolerability, and recommended Phase 2 dose (RP2D) of sonrotoclax through dose escalation. No dose-limiting toxicities were observed during this phase, and 320 mg once daily was identified as the RP2D. Part 2 evaluated sonrotoclax at the 320 mg RP2D following a 4-week dose ramp-up schedule in patients with relapsed or refractory MCL.
Eligibility for the efficacy-evaluable population required: histologically confirmed MCL, at least one prior anti-CD20-based therapy, at least one prior BTK inhibitor, ECOG performance status 0-2, adequate organ function, and no prior BCL-2 inhibitor therapy.
Efficacy results
| Endpoint | Result |
| Study population (Part 2) | 103 adults with R/R MCL; median age 68; all received prior anti-CD20 and BTK inhibitor |
| Prior lines of therapy (median) | 3 (range 2–9) |
| Overall response rate (ORR) | 52% (95% CI 42–62%; 1-sided p<0.0001) |
| Complete response (CR) rate | 15.5% (95% CI 9.1–24.0%) |
| Partial response (PR) rate | 36.9% |
| Median time to first response | 1.9 months (range 1.6–6.2 months) |
| Median duration of response (DOR) | 15.8 months (95% CI 7.4 months to not estimable) |
| Median follow-up (efficacy analysis) | 11.9 months (per IRC) / 14.2 months (per Targeted Oncology) |
| TP53-mutant subgroup ORR | 59.1% |
| Assessment method | Independent review committee (IRC) using Lugano criteria |
Source: FDA press release May 13, 2026. AJMC, ASCO Post, CancerNetwork, Targeted Oncology. BGB-11417-201, NCT05471843.
A 52% ORR in a heavily pre-treated population, many of whom had BTK inhibitor-resistant disease after a median of three prior lines of therapy, is a meaningful result. The 15.8-month median DOR is also notable in a disease where post-BTK responses often last only a few months. The upper bound of the DOR confidence interval (not estimable) at a median follow-up of approximately 12 months suggests that a proportion of responses were still ongoing at the time of analysis.
The TP53-mutant subgroup ORR of 59.1% is the most clinically significant finding for oncologists. Standard chemotherapy regimens are typically less effective in TP53-mutant MCL, and a response rate numerically higher in this subgroup than in the overall population suggests that BCL-2 inhibition may offer the most value precisely where current options are least effective.
| What accelerated approval means for this drug The FDA’s accelerated approval pathway allows earlier approval of drugs for serious conditions based on a surrogate endpoint (in this case, ORR and DOR) that is reasonably likely to predict clinical benefit, while requiring the sponsor to conduct confirmatory trials demonstrating actual clinical benefit such as overall survival. For Beqalzi, continued approval may depend on the results of confirmatory studies. BeOne Medicines is conducting a broader clinical program for sonrotoclax, including combination studies with BTK inhibitors (notably zanubrutinib, also a BeOne Medicine product) in MCL and other B-cell malignancies. If those studies demonstrate clinical benefit, the accelerated approval pathway to full approval becomes available. For patients with relapsed or refractory MCL who have exhausted prior lines of therapy, accelerated approval provides access to an investigational drug that has demonstrated meaningful activity now, rather than waiting for the confirmatory trial to complete. This is the intended purpose of the pathway for serious, life-threatening conditions. |
Safety: The TLS Warning That Requires Proactive Management
Tumor lysis syndrome: the primary safety concern
Tumor lysis syndrome is the most serious safety concern for Beqalzi, shared with venetoclax and other potent agents that rapidly kill large numbers of cancer cells. When cancer cells die quickly, they release their contents into the bloodstream: potassium, phosphate, nucleic acids, and uric acid. The kidneys may not be able to clear this influx quickly enough, leading to a metabolic emergency that can cause kidney failure, life-threatening cardiac arrhythmias, seizures, and death.
Beqalzi’s prescribing information requires the following TLS management steps:
- Pre-treatment risk assessment: Evaluate the patient’s baseline risk of TLS based on tumor bulk, renal function, and uric acid levels before starting Beqalzi.
- Prophylactic hydration: Patients should drink 6 to 8 glasses (approximately 1.5 to 2 liters) of water daily starting 1 to 2 days before the first dose, on the day of the first dose, on any day the dose is increased, and when restarting treatment.
- Anti-hyperuricemic agents: Healthcare providers may prescribe allopurinol or rasburicase before and during the dose ramp-up to reduce uric acid levels.
- Blood monitoring: Blood tests for TLS markers (potassium, phosphate, uric acid, creatinine) are required before and during treatment, especially during the 4-week ramp-up.
- 4-week ramp-up schedule: Doses are increased stepwise over 4 weeks to reach the 320 mg target dose, reducing the rate of cell death at any one time and lowering TLS risk. Strong CYP3A inhibitors are contraindicated during the ramp-up phase as they increase sonrotoclax exposure.
Other important safety findings from the trial
Serious adverse reactions occurred in 37% of patients in the trial, with pneumonia the most common serious adverse reaction at 10%. Grade 3 or 4 laboratory abnormalities occurring in at least 15% of patients included decreased lymphocyte counts and decreased neutrophil counts. The most common adverse reactions overall were pneumonia, fatigue, edema, diarrhea, and upper respiratory tract infection.
The prescribing information also carries warnings for serious infections (including fatal infections) and neutropenia, both of which require monitoring. Patients on Beqalzi who develop fever, chills, or other signs of infection should contact their oncology team promptly.
Beqalzi carries an embryo-fetal toxicity warning. Women of childbearing potential and male patients with female partners who could become pregnant must use effective contraception during treatment and for one week after the last dose.
Dosing and Administration: The 4-Week Ramp-Up Schedule
| Ramp-up week | Daily dose | Key requirement |
| Week 1 (days 1–7) | 20 mg once daily | TLS monitoring; avoid strong CYP3A inhibitors |
| Week 2 (days 8–14) | 80 mg once daily | TLS monitoring; hydration continued |
| Week 3 (days 15–21) | 160 mg once daily | Blood tests for TLS markers |
| Week 4 (days 22–28) | 240 mg once daily | Continue monitoring |
| Week 5 onward | 320 mg once daily | Target dose reached; once-daily dosing with food continues |
Beqalzi tablets are available in four strengths (1 mg, 5 mg, 20 mg, and 80 mg) to allow precise dosing throughout the ramp-up schedule. All doses should be taken with food. If a dose is missed and it is more than 8 hours since the scheduled time, skip that dose and take the next scheduled dose at the regular time.
| The CYP3A inhibitor contraindication during ramp-up: a clinically important interaction Sonrotoclax is metabolized by CYP3A4. Strong CYP3A inhibitors, including azole antifungals (fluconazole, voriconazole, itraconazole), certain macrolide antibiotics (clarithromycin), and HIV protease inhibitors, significantly increase sonrotoclax exposure. This dramatically increases TLS risk during the ramp-up phase when doses are already being escalated. Starting Beqalzi or increasing the dose while a patient is taking a strong CYP3A inhibitor is contraindicated. Moderate CYP3A inhibitors require dose reduction. Patients and prescribers should review all concomitant medications carefully before initiating and during the ramp-up phase. If a patient needs to restart Beqalzi after a treatment break, the full ramp-up schedule must be repeated. This is an important point for patients who interrupt treatment due to adverse events or procedures. |
| 🔗 Also on HED: The FDA’s Real-Time Clinical Trials Initiative: AstraZeneca’s TRAVERSE Trial Involves the Same Drug Class Our post on the FDA’s April 2026 real-time clinical trials pilot covers the TRAVERSE trial, which studies acalabrutinib + venetoclax + rituximab in treatment-naive MCL at MD Anderson and UPenn. The combination of BTK inhibition and BCL-2 inhibition in the same patient population where Beqalzi is now approved for later lines illustrates how the MCL treatment landscape is being built out. |
What This Means for Patients with Relapsed Mantle Cell Lymphoma
Beqalzi is specifically for patients who have already received at least two prior lines of therapy including a BTK inhibitor. It is not a first-line or second-line therapy. For patients currently in earlier stages of MCL treatment, this approval does not change the immediate treatment path.
For patients who have received both a chemoimmunotherapy regimen and a BTK inhibitor and whose disease has progressed, Beqalzi now provides an FDA-approved BCL-2 inhibitor option with a 52% response rate and a median response duration of 15.8 months in a clinical trial population that closely reflects this setting.
Questions to discuss with your hematologist or oncologist if you or a family member is in this situation:
- Am I eligible for Beqalzi based on my treatment history? The requirement is at least two prior lines including a BTK inhibitor, with no prior BCL-2 inhibitor.
- What is my TLS risk profile, and what monitoring and prophylaxis will I need before and during the ramp-up?
- Are there clinical trials of sonrotoclax in combination with other agents that might be appropriate for my specific situation?
- Are there confirmatory trials I could participate in that would contribute to the evidence base for this drug?
Resources for patients with mantle cell lymphoma
For patients navigating MCL treatment decisions, the Lymphoma Research Foundation maintains patient education resources on MCL specifically, including information on clinical trial participation. The NCI’s Cancer Center directory can help identify centers with dedicated lymphoma programs and access to the newest approved therapies. For Beqalzi specifically, BeOne Medicines’ patient support program information will be available through the treating oncologist or hematologist at prescribing.
Sources
FDA accelerated approval announcement: FDA grants accelerated approval to sonrotoclax (Beqalzi) for relapsed or refractory mantle cell lymphoma. FDA.gov. May 13, 2026.
AJMC coverage: Sonrotoclax Granted Accelerated Approval for R/R Mantle Cell Lymphoma. ajmc.com. May 13, 2026.
Hematology Advisor: FDA Grants Accelerated Approval to Beqalzi for R/R Mantle Cell Lymphoma. hematologyadvisor.com. May 2026.
OncLive: FDA Approves Sonrotoclax for Relapsed/Refractory Mantle Cell Lymphoma. onclive.com. May 13, 2026.
CancerNetwork: FDA Approves Sonrotoclax in Relapsed/Refractory Mantle Cell Lymphoma. cancernetwork.com. May 2026.
Targeted Oncology: FDA Approves Next-Gen BCL2 Inhibitor Sonrotoclax for R/R Mantle Cell Lymphoma. targetedonc.com. May 2026.
CURE Today: FDA Approves Beqalzi for Relapsed Mantle Cell Lymphoma. curetoday.com. May 2026.
ASCO Post: Sonrotoclax Receives Accelerated Approval in Relapsed or Refractory MCL. ascopost.com. May 2026.
Oncology Nursing News: FDA Approves Sonrotoclax for R/R Mantle Cell Lymphoma. oncnursingnews.com. May 2026.
Drugs.com drug information: Beqalzi (sonrotoclax): Uses, Dosage, Side Effects, Warnings. drugs.com.
Trial registration: BGB-11417-201. A Study of Sonrotoclax (BGB-11417) in Participants With B-Cell Malignancies. NCT05471843. clinicaltrials.gov.
Patient resources: Lymphoma Research Foundation: lymphoma.org; NCI Cancer Centers: cancer.gov/research/nci-role/cancer-centers
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice. Beqalzi is approved under the accelerated approval pathway, and continued approval may depend on confirmatory trial results. All treatment decisions for mantle cell lymphoma should be made in close consultation with a qualified hematologist or oncologist. |
Leave a Reply