
| 📌 The essentials On February 13, 2025, the FDA approved an expanded label for IZERVAY (avacincaptad pegol intravitreal solution, Astellas Pharma), removing the 12-month treatment duration limit that was part of the original August 2023 approval. The drug is now approved without restriction on duration of treatment. The clinical basis: Two-year data from the GATHER2 Phase 3 trial (NCT04435366), published in Ophthalmology in December 2025, showing that the treatment benefit of IZERVAY more than doubled between year one and year two of continuous treatment. The year-two data also showed that every-other-month (EOM) dosing maintained efficacy comparable to monthly dosing, offering a meaningful reduction in treatment burden for patients who tolerate the drug. Who this matters for: Patients currently on IZERVAY approaching or past the previous 12-month ceiling, and patients with geographic atrophy (GA) secondary to AMD who have not yet started treatment and are weighing their options. |
|---|
Geographic atrophy is the advanced form of dry age-related macular degeneration, and until 2023, it had no approved treatments. Patients watched their central vision deteriorate with nothing to offer but AREDS2 vitamins to slow progression to the advanced stage. That changed when the FDA approved two complement inhibitors in the same year: pegcetacoplan (Syfovre, Apellis) in February 2023 and avacincaptad pegol (IZERVAY, Astellas) in August 2023. For the first time, retinal specialists had tools, modest ones but real ones, to slow the growth of GA lesions.
The original IZERVAY approval carried a limitation: the label authorized treatment for up to 12 months. That ceiling reflected the data available at the time of initial approval. But the GATHER2 Phase 3 trial continued beyond that point, and its two-year results are now in.
On February 13, 2025, the FDA approved an expanded label for IZERVAY, removing the 12-month dosing limit. The drug is now approved without a restriction on duration of treatment. The updated label is based on two-year data from GATHER2 showing that the benefit of IZERVAY continued to grow over time, more than doubling between year one and year two.
This post covers what geographic atrophy is and why treatment is difficult, how IZERVAY works, what the full GATHER2 data shows through two years, what the label change means in practice, and how IZERVAY sits in the context of the two available GA treatments.
Geographic Atrophy: The Disease Behind the Drug
Age-related macular degeneration (AMD) is the leading cause of central vision loss in adults over 50 in the developed world, affecting the macula, the small, high-acuity central area of the retina responsible for reading, recognizing faces, and driving. AMD progresses along a spectrum from early (drusen deposits, pigment changes) through intermediate to advanced forms.
Advanced AMD has two forms. Neovascular AMD (wet AMD) involves abnormal blood vessel growth beneath the retina, causing rapid vision loss that is treatable with anti-VEGF injections. Geographic atrophy (GA), the dry advanced form, involves progressive loss of retinal pigment epithelial (RPE) cells, photoreceptors, and the underlying choriocapillaris. The name comes from the appearance of the lesions on imaging: well-demarcated, map-like areas of atrophy that expand over time. GA progresses slowly but relentlessly, with no reversal of lost retinal tissue.
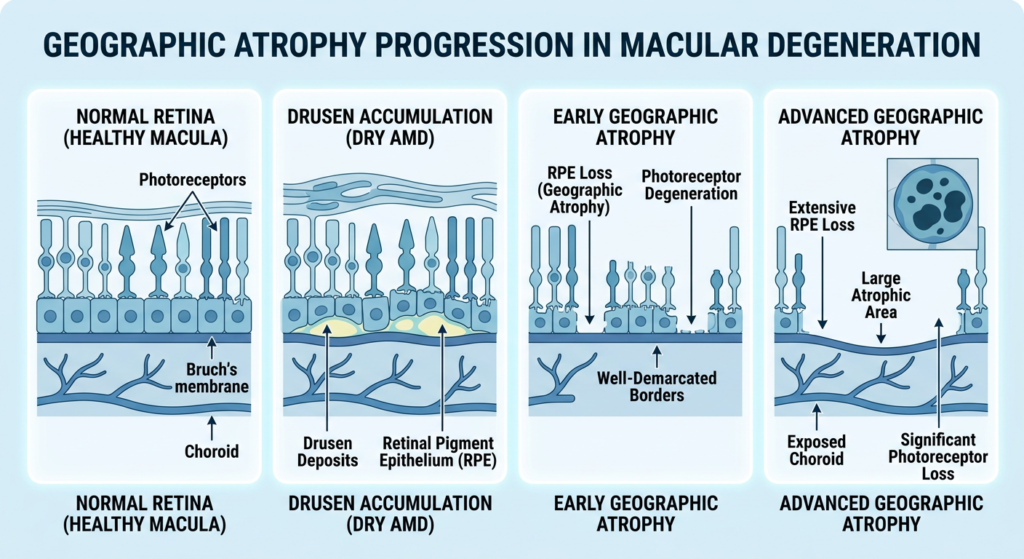
An estimated one million Americans have geographic atrophy. As GA expands toward the central fovea, it causes an increasingly large, permanent blind spot in central vision. The impact on reading, driving, and face recognition is severe. Because the process is slow and does not cause the sudden dramatic vision loss seen in wet AMD, patients sometimes do not realize the extent of their deterioration until it is substantial.
| Why GA is hard to treat and why lesion growth is the primary endpoint The complement system plays a central role in GA pathogenesis. Genome-wide association studies have identified complement factor H (CFH) variants as the strongest genetic risk factor for advanced AMD. Complement dysregulation causes chronic inflammation, drusen deposition, and formation of the membrane attack complex (MAC), which destroys RPE cells and photoreceptors. Because no treatment can restore dead retinal cells, approved therapies for GA are designed to slow the rate of lesion expansion, measured by area of GA on fundus autofluorescence imaging, rather than improve vision directly. Neither of the two approved GA drugs has demonstrated statistically significant improvement in best-corrected visual acuity (BCVA) in their pivotal trials. This is not a failure of the drugs; it reflects the biology of a slowly progressive disease where even a meaningful structural benefit may not translate to measurable visual gains over 12 to 24 months. The FDA accepted lesion growth rate as an acceptable primary endpoint for approval. The European Medicines Agency took a different position, declining to approve Syfovre on the grounds that lesion slowing was not sufficient evidence of clinically meaningful patient benefit. That regulatory distinction is worth understanding when comparing how this drug class is viewed globally. |
|---|
How IZERVAY Works: C5 Inhibition and the Complement Cascade
IZERVAY (avacincaptad pegol) is a pegylated RNA aptamer, a chemically modified oligonucleotide rather than a monoclonal antibody, that specifically inhibits complement protein C5. Understanding why C5 is the target and what an RNA aptamer is helps make sense of both the mechanism and the safety profile.
The complement cascade and C5’s role
The complement system is a network of proteins that form a critical arm of innate immunity. When activated, the cascade converges on two central reactions: cleavage of complement component C3 into C3a and C3b, and then cleavage of C5 into C5a and C5b. C5a is a potent pro-inflammatory mediator. C5b initiates assembly of the membrane attack complex (MAC), a protein complex that punches holes in cell membranes and destroys them. In GA, chronic overactivation of the complement pathway leads to persistent MAC formation and progressive destruction of RPE cells and photoreceptors.
IZERVAY blocks C5 cleavage, preventing formation of both C5a and C5b and therefore preventing downstream MAC assembly. Because C5 sits near the terminal end of the cascade, inhibiting it preserves upstream complement activity, including C3 function and opsonization, while specifically blocking the terminal destructive pathway implicated in GA.
What makes avacincaptad pegol an RNA aptamer
Unlike the monoclonal antibodies used in wet AMD (ranibizumab, bevacizumab, aflibercept), avacincaptad pegol is an RNA aptamer: a short, precisely folded strand of chemically modified RNA that binds its target protein, complement C5, with high specificity. The pegylation (attachment of polyethylene glycol chains) extends its half-life in the eye and improves stability. It is delivered as a 100 μL intravitreal injection directly into the vitreous humor of the eye.
| C5 vs. C3: Two targets, two drugs IZERVAY (avacincaptad pegol) targets C5, near the terminal end of the complement cascade. Syfovre (pegcetacoplan) targets C3, which sits upstream at the convergence of all three complement activation pathways (classical, alternative, and lectin). The theoretical advantage of C5 inhibition is that it preserves upstream C3 activity, including opsonization of pathogens and apoptotic cells, while blocking the terminal destructive MAC. The theoretical advantage of C3 inhibition is broader suppression of the cascade. Neither advantage has been definitively demonstrated to be clinically superior in head-to-head data. What is clear is that the two drugs have meaningfully different safety profiles, particularly regarding intraocular inflammation. Rare but serious cases of retinal vasculitis have been reported with pegcetacoplan in post-marketing surveillance. That signal has not been observed with avacincaptad pegol in clinical trials. |
|---|
The GATHER Trial Program: From Phase 2/3 to the Two-Year Label Change
The evidence base for IZERVAY rests on two Phase 3 trials: GATHER1 and GATHER2. Both evaluated monthly 2 mg intravitreal injections of avacincaptad pegol versus sham in patients with non-center-point-involving GA secondary to AMD. The primary endpoint in both was GA lesion growth rate measured by fundus autofluorescence.
GATHER1: Initial evidence and original approval
GATHER1 (NCT02686658) enrolled 286 patients across 12 months of treatment. The trial evaluated doses of 2 mg and 4 mg versus sham. The 2 mg dose reduced GA lesion growth rate by 27.4% (p=0.0072) and the 4 mg dose by 27.8% (p=0.0051) compared with corresponding sham groups. The 2 mg dose was selected for further development based on its favorable benefit-risk profile. These data, combined with GATHER2, formed the basis of the original August 2023 FDA approval.
GATHER2: The Phase 3 confirmatory trial through two years
GATHER2 (NCT04435366) was a randomized, double-masked, sham-controlled, multicenter Phase 3 trial enrolling 448 patients. For the first 12 months, patients received monthly IZERVAY 2 mg or sham. At month 12, patients originally assigned to IZERVAY were re-randomized to continue monthly (EM, n=96) or switch to every-other-month dosing (EOM, n=93). Sham patients continued on sham through year two (n=203).
| Timepoint | IZERVAY vs. Sham: GA growth rate reduction | Statistical significance |
|---|---|---|
| Year 1 (Month 12) | 14% reduction in monthly group vs. sham | p less than 0.01 (primary endpoint met) |
| Year 2 (Month 24), every-month dosing (EM) | Treatment benefit continued; total benefit more than doubled vs. year 1 | Maintained vs. sham |
| Year 2 (Month 24), every-other-month (EOM) | Treatment benefit maintained at comparable level to EM | Maintained vs. sham |
| Onset of benefit | Observed as early as 6 months | Statistically significant from month 6 onward |
The two-year findings carry a clinically important message: the benefit of IZERVAY did not plateau or diminish with continued treatment. It grew. The reduction in GA growth rate more than doubled between year one and year two, suggesting that the treatment effect compounds over time as the drug continues to suppress terminal complement activation and MAC formation. This is consistent with the biology: continuous inhibition of the destructive pathway progressively spares more retinal tissue relative to an untreated eye.
The every-other-month data in year two is also practically significant. Reducing injection frequency from monthly to bimonthly without loss of efficacy substantially reduces the treatment burden for patients who are tolerating therapy. Fewer clinic visits and injections per year is a meaningful quality-of-life consideration for an older patient population managing multiple chronic conditions.
Safety Through Two Years: What the GATHER2 Data Shows
The safety profile of IZERVAY over two years in GATHER2 was consistent with year-one observations, with no new or significant signals. For patients and prescribers making long-term treatment decisions, the two-year safety picture matters as much as the efficacy data.
| Adverse event | IZERVAY (2-yr data) | Clinical note |
|---|---|---|
| Endophthalmitis (eye infection) | 1 case (culture-positive, non-serious) | Rare; inherent risk of any intravitreal injection |
| Intraocular inflammation (serious) | 0 cases | No serious IOI; no cases of retinal vasculitis |
| Ischemic optic neuropathy | 0 cases | Safety signal seen with Syfovre; absent here |
| Choroidal neovascularization (CNV)/wet AMD conversion | IZERVAY: 11.6% vs. Sham: 9.0% | Small numerical increase; class effect for complement inhibitors |
| Conjunctival hemorrhage (most common AE) | Common | Typical injection-site reaction; self-limiting |
| Increased intraocular pressure | Common | Transient; monitored post-injection |
| Blurred vision | Common | Typically transient |
The absence of serious intraocular inflammation, retinal vasculitis, and ischemic optic neuropathy over two years is a notable feature of the IZERVAY safety profile. These events have been reported in post-marketing surveillance with pegcetacoplan (Syfovre), and their absence in GATHER2 is meaningful context for the prescribing decision.
The small numerical increase in choroidal neovascularization (wet AMD conversion) with IZERVAY, 11.6% versus 9% in the sham group, is a known class effect of complement inhibition shared to some degree by both approved GA drugs. Complement pathway suppression may alter the balance of angiogenic regulation in the retina. Patients receiving IZERVAY should be monitored for signs of wet AMD conversion: visual distortions, straight lines appearing bent, or new deterioration in central vision.
| Key contraindications and precautions for IZERVAY Do not use IZERVAY in patients with: Active ocular or periocular infection; Active intraocular inflammation; History of or active choroidal neovascularization (wet AMD). Monitor for and counsel patients to report: Redness, pain, increased discomfort, worsening redness, or decreased/blurred vision after injection, which may be signs of endophthalmitis or retinal detachment; Visual distortions or new central vision changes, which may be signs of wet AMD conversion; Flashes of light or increased floaters, which may be signs of possible retinal complications. Patients should not drive or use machinery until vision has recovered after each injection. Full prescribing information is available at accessdata.fda.gov. |
|---|
What Removing the 12-Month Cap Means in Practice
The original IZERVAY approval in August 2023 included a duration limitation: the label authorized use for up to 12 months. This ceiling was not arbitrary. It reflected the controlled trial data available at the time of the initial BLA, which covered only year-one efficacy and safety from GATHER2.
Following a regulatory path that included a supplemental NDA submission, an initial Complete Response Letter from the FDA in November 2024, a rapid resubmission in December 2024, and FDA approval on February 13, 2025, the label no longer carries that limitation.
| Before (original label) | After (updated label, Feb 2025) |
|---|---|
| Duration of treatment limited to 12 months | No limitation on duration of treatment |
| Patients approaching the 12-month mark faced uncertainty about continuation | Ongoing treatment can continue without an administrative ceiling |
| Physicians managing longer-term patients had limited label support | Full prescribing information now covers two years of documented efficacy and safety |
| Every-other-month dosing option in year 2 not formally labeled | GATHER2 year-2 EOM data incorporated; flexible dosing schedules now supported by label |
The label change also has implications for the roughly 210,000 vials of IZERVAY distributed through December 2024. Patients already on therapy who were managed month-to-month under the year-one framework can now continue with the support of two-year efficacy and safety data in the formal prescribing information.
Post-marketing safety reporting through the time of the label update remained consistent with the clinical trial program. No new or significant safety signals were identified in commercial use.
IZERVAY in Context: Two Approved Drugs for a Disease Once Left Untreated
The GA treatment landscape currently consists of two FDA-approved intravitreal complement inhibitors. No head-to-head clinical trial comparing them has been conducted. Here is a plain-language comparison of where they stand:
| Feature | IZERVAY (avacincaptad pegol) | Syfovre (pegcetacoplan) |
|---|---|---|
| Developer | Astellas Pharma | Apellis Pharmaceuticals |
| Mechanism | Complement C5 inhibitor (RNA aptamer) | Complement C3 inhibitor (pegylated peptide) |
| Original FDA approval | August 2023 | February 2023 |
| Duration restriction | None, removed Feb 2025 | None |
| Dosing | Monthly or every other month (EOM) | Monthly or every other month (EOM) |
| Pivotal trial primary endpoint (yr 1) | GATHER1: 27% reduction (2 mg); GATHER2: 14% reduction | OAKS: 21% reduction (monthly); DERBY: 12% reduction (not statistically significant) |
| Statistically significant primary endpoint | Met in both Phase 3 trials (GATHER1 and GATHER2) | Met in OAKS; not met in DERBY |
| Post-marketing retinal vasculitis signal | Not observed in clinical trials | Rare cases reported in post-marketing surveillance |
| Intraocular inflammation | No serious cases in GATHER2 through 2 years | Reported in post-marketing; retinal vasculitis cases |
| EU regulatory status | EMA application withdrawn by Astellas (Oct 2024) | Refused marketing authorization by EMA (Sep 2024) |
| Patient population studied | Non-center-point-involving GA only | Both subfoveal and non-subfoveal GA (broader population) |
A few contextual points are worth understanding:
Neither drug has demonstrated improvement in best-corrected visual acuity (BCVA) in their pivotal trials, which is a genuine limitation and the source of ongoing debate in the retinal community. The EMA declined to approve both drugs on the grounds that lesion slowing without demonstrated functional benefit did not meet the European standard for clinical meaningfulness. The FDA, evaluating the same data, reached a different conclusion, accepting lesion growth rate as a valid surrogate endpoint for GA progression.
IZERVAY’s pivotal trials enrolled patients with non-center-point-involving GA, meaning GA that had not yet reached the central fovea. Syfovre’s trials enrolled a broader population including patients with subfoveal GA. This enrollment difference means the two trials are not directly comparable, and patients with subfoveal involvement are outside the population studied in GATHER1 and GATHER2.
No randomized head-to-head comparison has been conducted. The right drug for an individual patient involves shared decision-making with a retinal specialist considering both efficacy and safety, individual risk factors, and payer formulary.
Both drugs require indefinite monthly or bimonthly intravitreal injections, a significant treatment burden for an older patient population, many of whom have bilateral GA.
What This Means for Patients with Geographic Atrophy
The removal of the 12-month dosing limit is straightforward good news for patients already on IZERVAY who are tolerating the drug and want to continue. It is also good news for prescribers who can now manage GA patients on a longer-term basis with full label support and two years of documented efficacy and safety data.
What this approval does not change is the fundamental nature of GA treatment: these drugs slow the progression of an irreversible disease. They do not restore lost vision. The decision to start, continue, or stop treatment involves weighing modest lesion-growth benefit against the burden of indefinite injections, the small risk of wet AMD conversion, and the individual patient’s preferences, disease location, and visual function goals.
For patients with GA who have not yet been treated, the conversation with a retinal specialist should now include the full picture of two-year data, the flexibility of monthly or every-other-month dosing, and the comparative safety and efficacy profiles of the two available treatments.
The American Academy of Ophthalmology and the BrightFocus Foundation maintain current patient resources on geographic atrophy and AMD treatment options. For patients interested in clinical trials evaluating next-generation GA therapies, ClinicalTrials.gov lists open enrollment studies.
For related coverage of how FDA label updates are expanding treatment options across multiple specialties in 2026, see our post on Nexplanon’s FDA-approved extension from 3 years to 5 years and our analysis of the first approved immunotherapy for ovarian cancer.
Sources
Astellas press release: U.S. FDA Approves Expanded Label for IZERVAY (avacincaptad pegol intravitreal solution) for Geographic Atrophy. February 13, 2025. newsroom.astellas.com.
GATHER1 Phase 2/3 results: Jaffe GJ et al. C5 Inhibitor Avacincaptad Pegol for Geographic Atrophy Due to Age-Related Macular Degeneration: A Randomized Pivotal Phase 2/3 Trial (GATHER1). Ophthalmology. 2021;128(4):576–586.
GATHER2 12-month results: Khanani AM et al. Efficacy and safety of avacincaptad pegol in patients with geographic atrophy (GATHER2): 12-month results from a randomised, double-masked, phase 3 trial. The Lancet. September 2023.
GATHER2 trial registration: NCT04435366. ClinicalTrials.gov.
GATHER1 trial registration: NCT02686658. ClinicalTrials.gov.
IZERVAY original FDA approval: FDA approves avacincaptad pegol for geographic atrophy secondary to age-related macular degeneration. FDA.gov. August 2023.
IZERVAY prescribing information: IZERVAY (avacincaptad pegol intravitreal solution). FDA.gov.
Ophthalmology Advisor label update coverage: Izervay Label Update Removes Limit on Treatment Duration for Geographic Atrophy. ophthalmologyadvisor.com. February 2025.
Applied Clinical Trials: Two Year Trial Data Show Long-Term Efficacy of Izervay. appliedclinicaltrialsonline.com.
AAO IZERVAY/Syfovre overview: What to Know About Syfovre and Izervay for Geographic Atrophy. aao.org. April 2025.
EMA Syfovre refusal: Syfovre: Final opinion confirming refusal of marketing authorisation. EMA. September 2024.
FDA Syfovre retinal vasculitis safety communication: FDA Drug Safety Communication: FDA warns about rare but serious risk of vision loss from retinal vasculitis associated with Syfovre. FDA.gov.
Patient resources: American Academy of Ophthalmology | BrightFocus Foundation | NEI AMD overview | ClinicalTrials.gov: geographic atrophy studies
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice. Treatment decisions regarding IZERVAY or any other geographic atrophy therapy should be made in consultation with a qualified, board-certified ophthalmologist or retinal specialist who can evaluate individual disease characteristics, risk factors, and treatment goals. |
|---|
Leave a Reply