| 📌 The essentials Opsumit (macitentan, Johnson & Johnson/Actelion) is an oral dual endothelin receptor antagonist (ERA) approved for the chronic treatment of adults with pulmonary arterial hypertension (PAH, WHO Group I) to delay disease progression. It generated $1.63 billion in U.S. sales in 2025. Annual costs for patients without adequate coverage can exceed $100,000. The clinical basis: the SERAPHIN trial (NCT00660179), a landmark Phase 3 study that was the first in PAH to use a morbidity and mortality composite as its primary endpoint. Key result: 45% risk reduction in the primary morbidity/mortality composite with macitentan 10 mg versus placebo (HR 0.55; 97.5% CI 0.39 to 0.76; p less than 0.001). Generic approvals: the FDA has approved at least five generic versions of macitentan 10 mg tablets, from manufacturers including Zydus Cadila (first approval), Alembic, MSN Pharmaceuticals, and Sun Pharmaceuticals. Launches were delayed by patent litigation; generic macitentan is now entering the U.S. market. LOE strategy to know: in March 2024, J&J received FDA approval for Opsynvi, a fixed-dose single tablet combining macitentan 10 mg and tadalafil 40 mg, with its own exclusivity period. REMS program: macitentan carries a boxed warning for embryo-fetal toxicity and is available only through the Macitentan-Containing Products REMS program. This requirement applies to all generic versions identically to the brand. Monthly pregnancy testing for females of reproductive potential is required throughout treatment. |
|---|
| 📚 About this series: the 2026 Loss of Exclusivity Watch This is Post 3 of HED’s 2026 Loss of Exclusivity series, tracking the ten major drugs losing U.S. exclusivity this year. The full series covers: Xolair (omalizumab) • Pomalyst (pomalidomide) • Opsumit (macitentan) • Januvia/Janumet (sitagliptin) • Simponi (golimumab) • Mavenclad (cladribine) • Gattex (teduglutide) • Trintellix (vortioxetine) • Briviact (brivaracetam) • Xeljanz (tofacitinib). Each post follows the same format: what the drug is and how it works, what the clinical evidence shows, who uses it and why, and what the entrance of competition means for patients, prescribers, and the market. |
|---|
Pulmonary arterial hypertension is a disease most people have never heard of. That obscurity is partly a function of its rarity, affecting somewhere between 15 and 50 people per 100,000 depending on the population studied, and partly a function of how it presents. The early symptoms are easy to attribute to something more common: shortness of breath on exertion, fatigue, occasional dizziness. By the time most patients receive a correct diagnosis, the disease has been progressing for months or years.
PAH is a rare, debilitating, progressive, and life-threatening disease of the pulmonary vasculature, characterized by vascular proliferation and remodeling of small pulmonary arteries. It is defined by a mean pulmonary arterial pressure of 25 mmHg or greater and a pulmonary wedge pressure of 15 mmHg or less. Left untreated, it leads to right heart failure and premature death. Prior to the availability of PAH drug therapies, median survival was 2.8 years, with survival rates of 68%, 48%, and 34% at one, three, and five years respectively.
Those pre-treatment survival figures tell you everything about why this disease matters clinically and why access to effective therapy is not academic. This is a condition where treatment makes the difference between years of functional life and rapid deterioration toward right heart failure.
Opsumit (macitentan), developed by Actelion and now owned by Johnson and Johnson following a $30 billion acquisition in 2017, generated $1.63 billion in U.S. sales in 2025. It is one of a small number of drugs with robust evidence of slowing PAH progression, based on a landmark clinical trial that was the first in this disease to use morbidity and mortality as its primary endpoint rather than the exercise-capacity surrogates that earlier trials relied upon.
The FDA has already approved five generic versions of macitentan 10 mg, with approvals beginning in 2023. However, none were available for sale in the U.S. as of early 2026, held back by patent litigation and settlement timelines. That is now changing.
This post covers what pulmonary arterial hypertension is, how the endothelin system drives its progression, what made the SERAPHIN trial design genuinely different from what came before, what the data shows, where Opsumit fits in today’s treatment landscape alongside the newer Opsynvi fixed-dose combination, what the REMS requirements mean for patients, and what the entrance of generic competition is likely to mean for a patient population that has faced enormous access barriers for over a decade.
What Pulmonary Arterial Hypertension Is and Why It Is Not the Same as Regular High Blood Pressure
The word “hypertension” creates confusion. Pulmonary arterial hypertension has nothing to do with the systemic high blood pressure managed with lisinopril, amlodipine, or hydrochlorothiazide. It is a fundamentally different condition affecting a different vascular bed with different pathological mechanisms and a far more serious prognosis.
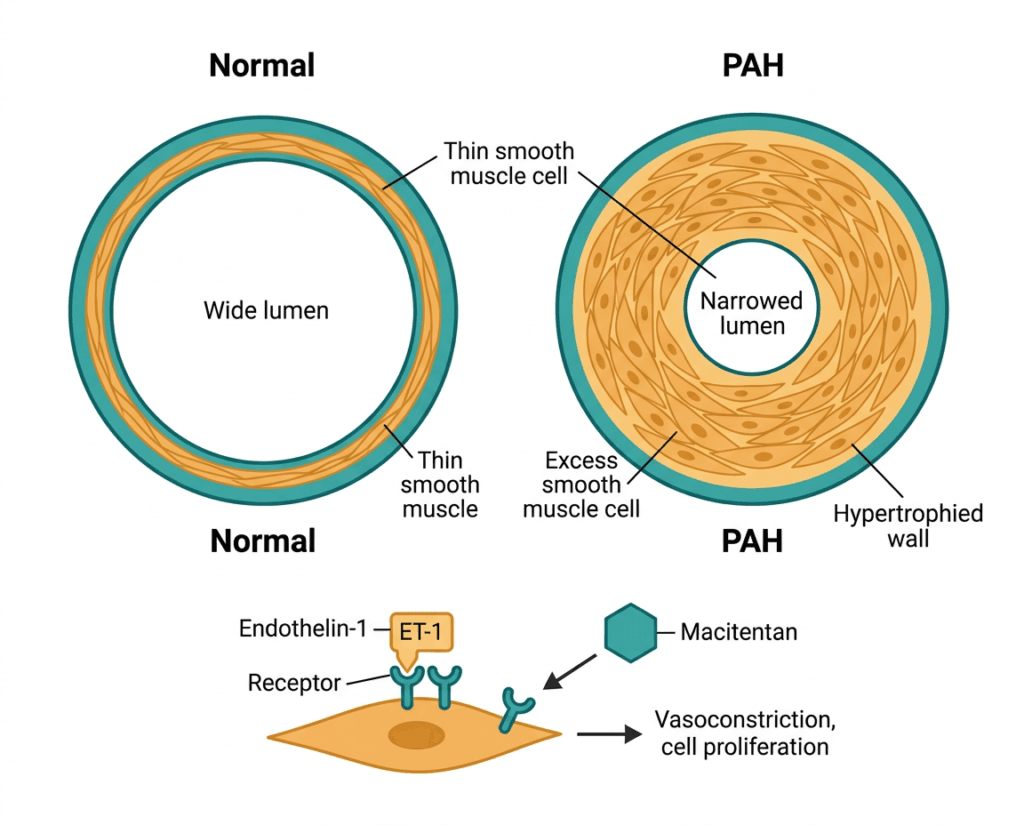
In PAH, the small pulmonary arteries, the vessels carrying blood from the right side of the heart through the lungs to pick up oxygen, undergo progressive structural remodeling. The vessel walls thicken. The lumens narrow. Abnormal cell proliferation, vasoconstriction, thrombosis, and inflammation converge to create a situation where the right ventricle must work against massively increased resistance to push blood through the lungs. Over time, the right ventricle enlarges and begins to fail.
Women are more likely to have PAH, with registries reporting a 65 to 80% female predominance. Earlier studies suggested a mean diagnosis age in the 30s; more recent registries suggest a mean age of diagnosis in the 50s. U.S. registry data suggest a 5-year survival rate of approximately 57% from the time of diagnostic right-heart catheterization without treatment.
The WHO functional classification used in PAH captures the clinical reality of the disease’s progression:
| WHO functional class | Description | Clinical relevance |
|---|---|---|
| Class I | No limitation of physical activity; ordinary activity causes no symptoms | Rare at diagnosis; goal of aggressive treatment |
| Class II | Slight limitation of physical activity; comfortable at rest; ordinary activity causes dyspnea, fatigue, or presyncope | Common presentation; treatment initiation typically begins here |
| Class III | Marked limitation of physical activity; comfortable at rest; less-than-ordinary activity causes symptoms | Most patients present here; disease significantly limits daily life |
| Class IV | Inability to carry out any physical activity without symptoms; signs of right heart failure may be present at rest | Late-stage; high mortality risk; often requires IV prostacyclin therapy |
PAH has multiple subtypes. Idiopathic PAH, where no underlying cause is identified, accounts for roughly 39 to 46% of cases. Other forms are associated with connective tissue diseases (particularly systemic sclerosis), congenital heart disease, HIV infection, portal hypertension, and drug or toxin exposures. All share the same pathological vascular remodeling process and are treated with similar targeted therapies.
The Endothelin System: Why It Matters in PAH
Three main molecular pathways are dysregulated in PAH and serve as targets for approved therapies: the endothelin pathway, the nitric oxide/cGMP pathway, and the prostacyclin pathway. Macitentan targets the first.
Endothelin-1 (ET-1) is a peptide produced by vascular endothelial cells. Under normal circumstances, ET-1 plays a regulatory role in vascular tone. In PAH, ET-1 levels in pulmonary arterial tissue are markedly elevated, and the ET-1 system becomes a driver of both vasoconstriction and the abnormal smooth muscle cell proliferation that progressively narrows pulmonary vessels.
ET-1 exerts its effects through two receptor subtypes: endothelin receptor A (ETA) and endothelin receptor B (ETB). ETA receptors on smooth muscle cells mediate vasoconstriction and proliferation. ETB receptors on endothelial cells mediate ET-1 clearance and nitric oxide release, a vasodilatory signal. This creates a pharmacological distinction between selective ETA blockade (preserving ETB-mediated clearance) and dual ETA/ETB blockade. Ambrisentan is a selective ETA antagonist; bosentan and macitentan are dual antagonists.
Macitentan was developed by modifying the structure of bosentan to increase efficacy and tissue penetration. Endothelin-1 acts primarily in tissues, in the walls of pulmonary vessels, rather than in the bloodstream. By increasing lipophilicity and receptor affinity, macitentan achieves deeper tissue penetration at a distribution coefficient ratio of 800:1 (lipid phase to aqueous phase), compared with 20:1 for bosentan. Because of its lower dissociation rate, macitentan behaves as what researchers call an insurmountable antagonist in functional assays of pulmonary arterial smooth muscle cells: it holds onto the receptor even when ET-1 concentrations are high. Its predecessors could be displaced from the receptor when ET-1 levels rose, precisely the situation in high-pressure PAH tissue. Macitentan’s pharmacological profile also includes an active metabolite, ACT-132577, that contributes to its prolonged duration of action. The slow receptor dissociation kinetics that differentiate macitentan from other ERAs were demonstrated in pulmonary arterial smooth muscle cell-based assays and were central to its development rationale.
The SERAPHIN Trial: Why This Was a Different Kind of Evidence
Most PAH drug trials before SERAPHIN were short, typically 12 to 16 weeks, and used a single surrogate endpoint: the six-minute walk distance (6MWD), a measure of how far a patient can walk in six minutes. 6MWD is a reasonable proxy for functional capacity, but it is not a clinical outcome. Patients can walk further and still progress to clinical worsening, hospitalization, or death.
SERAPHIN (NCT00660179) was designed differently. It enrolled 742 patients and was the first PAH trial to use a morbidity and mortality composite as its primary endpoint rather than a surrogate. Patients were randomized to macitentan 3 mg, macitentan 10 mg, or placebo for a median duration of approximately 100 weeks. The primary endpoint was a composite of: worsening of PAH (defined by specific criteria), initiation of intravenous or subcutaneous prostanoid therapy, atrial septostomy, lung transplantation, or death from any cause. These are real clinical events, not surrogate measures.
| Endpoint | Placebo | Macitentan 3 mg | Macitentan 10 mg |
|---|---|---|---|
| Primary morbidity/mortality event (% of patients) | 46.4% | 38.0% | 31.4% |
| Hazard ratio versus placebo | — | 0.70 (97.5% CI 0.52 to 0.96) | 0.55 (97.5% CI 0.39 to 0.76) |
| Risk reduction versus placebo | — | 30% | 45% |
| p-value (10 mg) | — | — | p less than 0.001 |
| Change in 6MWD at Month 6 | — | +7.4 m | +12.5 m |
| Median treatment duration | — | approximately 99.5 weeks | approximately 103.9 weeks |
Source: Pulido T et al. Macitentan and Morbidity and Mortality in Pulmonary Arterial Hypertension. NEJM. 2013;369(9):809–818. doi:10.1056/NEJMoa1213917. SERAPHIN trial, NCT00660179.
Two sub-analyses from SERAPHIN are particularly important for clinical practice. For patients already on background PAH therapy at baseline, macitentan 10 mg reduced the primary endpoint risk by 38% versus placebo. For treatment-naive patients, the risk reduction was 55%. The benefit existed whether or not patients were already being treated with another PAH agent, which validated macitentan’s use in both combination and monotherapy settings.
One caveat: there was a trend toward a macitentan-related reduction in death, but this was not statistically significant. SERAPHIN was not powered to detect a difference in mortality alone, and in a progressive disease where clinical deterioration likely precedes death, mortality was unlikely to be recorded as the first event. SERAPHIN proved macitentan reduces clinical worsening. It did not individually establish a mortality benefit, though the overall composite is clinically meaningful.
Dr. Sanjay Mehta, MD, FRCPC, FCCP, Professor of Medicine at the University of Western Ontario and SERAPHIN investigator, has described the study as demonstrating that macitentan significantly reduced the risk of morbidity and mortality in both treatment-naive patients and patients already on background therapy, with the benefit observed for several important indicators of PAH progression.
Where Macitentan Fits in Today’s PAH Treatment Landscape
The PAH treatment landscape in 2026 is considerably more complex than it was when Opsumit was approved in October 2013. Current guidelines recommend combination therapy targeting multiple pathways simultaneously as the standard approach for most patients, rather than sequential monotherapy as was the norm for the first decade of targeted PAH treatment.
| Pathway | Drug class | Approved agents |
|---|---|---|
| Endothelin pathway | Endothelin receptor antagonists (ERAs) | Bosentan (Tracleer), Ambrisentan (Letairis), Macitentan (Opsumit) |
| Nitric oxide/cGMP pathway | PDE5 inhibitors | Sildenafil (Revatio), Tadalafil (Adcirca) |
| Nitric oxide/cGMP pathway | Soluble guanylate cyclase stimulators | Riociguat (Adempas) |
| Prostacyclin pathway | Prostacyclin analogues and receptor agonists | Epoprostenol (IV), Treprostinil (IV/SC/inhaled/oral), Iloprost (inhaled), Selexipag (Uptravi) |
Current guidelines from the European Society of Cardiology and the American Heart Association/American Thoracic Society recommend starting most patients with at least dual combination therapy at diagnosis, typically an ERA plus a PDE5 inhibitor. Macitentan and tadalafil have become one of the most commonly prescribed combination regimens, which is precisely the clinical rationale behind J&J’s development of Opsynvi.
Opsynvi: J&J’s LOE response strategy
On March 22, 2024, the FDA approved Opsynvi, a single-tablet combination of macitentan 10 mg and tadalafil 40 mg, for the chronic treatment of adults with PAH (WHO Group I and WHO Functional Class II to III). Opsynvi may be used in patients who are treatment-naive or who are already on an ERA, PDE5 inhibitor, or both.
The Opsynvi fixed-dose combination carries its own unique period of exclusivity, giving Johnson and Johnson a commercial product intended to mitigate revenue loss from generics of macitentan alone. This is a well-established pharmaceutical lifecycle strategy: develop a fixed-dose combination with its own patent protection before the individual component loses exclusivity. For patients, Opsynvi represents a simpler regimen, one tablet once daily instead of two separate pills, which has clinical value when guidelines call for dual-pathway treatment regardless of risk stratification.
The approval was based on data from the Phase 3 A DUE study, in which the single-pill macitentan and tadalafil combination outperformed either drug as monotherapy, showing greater reductions in pulmonary vascular resistance from baseline to 16 weeks.
For patients currently on separate macitentan and tadalafil tablets, a transition to Opsynvi is worth discussing with a specialist. For patients where cost is a barrier, generic macitentan used alongside generic or branded tadalafil may be a more accessible path, but that conversation requires specialist guidance on regimen coordination and monitoring.
The REMS Program: What It Requires and Why It Applies to Generics
Like pomalidomide (covered in Post 2 of this series), macitentan carries a boxed warning for embryo-fetal toxicity and is available only through a REMS program. The mechanism differs from pomalidomide’s teratogenicity: macitentan causes fetal harm based on animal reproduction studies showing abnormal fetal development at exposures below the human therapeutic dose. The regulatory framework is comparable.
The Macitentan-Containing Products REMS, covering Opsumit, Opsynvi, and all generics, requires:
- Females of reproductive potential must enroll in the REMS and comply with monthly pregnancy testing throughout treatment
- Two forms of contraception are required during treatment and for one month after the last dose
- Prescribers must be certified to prescribe macitentan-containing products
- Pharmacies must be certified to dispense them
These requirements do not disappear when a generic version launches. Generic manufacturers are required to operate under the same REMS framework as the brand-name product. For patients, this means the process of obtaining generic macitentan will not feel substantially different from obtaining Opsumit in terms of safety checkpoints. If you have been on Opsumit for any length of time, you are already enrolled in the program. The brand name changes; the safety process does not.
The Safety Profile: What the Trial Data and Prescribing Information Show
A network meta-analysis comparing ERAs in PAH found that compared with placebo, macitentan significantly increased the risk of anemia (RR 3.42; 95% CI 1.65 to 7.07). Within the ERA class, bosentan carried the highest risk of abnormal liver function; ambrisentan carried the highest risk of peripheral edema; and macitentan carried the highest risk of anemia. These distinctions inform drug selection and monitoring choices.
| Safety item | Details | Clinical guidance |
|---|---|---|
| Embryo-fetal toxicity (boxed warning) | Macitentan causes fetal harm based on animal data. Contraindicated in pregnancy. | REMS enrollment required. Monthly pregnancy testing for females of reproductive potential. Two forms of contraception during treatment and for 1 month after the last dose. |
| Anemia | More common with macitentan than with bosentan or ambrisentan; observed in approximately 13% of SERAPHIN patients versus 3% with placebo. | CBC monitoring at baseline, 1 month, and periodically thereafter. Dose reduction or discontinuation may be required for significant anemia. |
| Nasopharyngitis and upper respiratory infections | Most common adverse event overall; reported in approximately 14% of SERAPHIN patients. | Generally mild; monitor and manage symptomatically. |
| Headache and flushing | Common ERA class effects from peripheral vasodilation. | Typically mild and usually resolves with continued treatment. |
| Hepatotoxicity | Less common than with bosentan, which carries a specific liver function monitoring requirement. Liver enzyme elevations reported. | Periodic liver function monitoring recommended. |
| Peripheral edema | Less common than with ambrisentan. | Particularly relevant in patients with right heart failure who may have baseline fluid retention. |
| Pulmonary edema in PVOD | ERA therapy can precipitate acute pulmonary edema in patients with pulmonary veno-occlusive disease (PVOD), a related but distinct condition. | Macitentan is contraindicated in PVOD. Accurate diagnosis before initiating therapy is essential. |
| Drug interactions | Macitentan is metabolized primarily by CYP3A4. Strong CYP3A4 inhibitors (ketoconazole, ritonavir) increase exposure; strong inducers (rifampin) decrease it. | Review all concurrent medications before initiating. |
The Generic Landscape: Five Approved, Now Entering the Market
Orphan disease drug pricing reflects the reality of small patient populations: manufacturers price to recoup development costs over a limited commercial base. Monthly costs for Opsumit run into the thousands of dollars, with annual costs for patients without adequate coverage potentially exceeding $100,000.
The manufacturers with FDA-approved generic macitentan 10 mg tablets as of 2026:
| Manufacturer | Approval notes |
|---|---|
| Zydus Cadila | First approval |
| Alembic Pharmaceuticals | Approved August 2025 |
| MSN Pharmaceuticals | Approved August 2025 |
| Sun Pharmaceuticals | Approved August 2025 |
| Additional manufacturers | Further approvals expected as remaining patent disputes resolve |
Market entry for generic macitentan has been delayed relative to the FDA approval dates because of patent litigation. Johnson and Johnson holds multiple layers of patent protection on macitentan, including compound, formulation, and method-of-use patents, and has used settlement agreements to control generic entry timing. This is a common dynamic in the rare disease pharmaceutical market and is not unique to macitentan.
Several factors specific to PAH as a disease category shape the generic transition differently from more common conditions:
PAH treatment is managed by specialists at certified PAH centers, and those specialists are appropriately conservative about switching stable patients to alternative formulations. In a disease where clinical worsening can progress rapidly and hospitalizations carry serious mortality risk, treatment changes are never made casually.
PAH patients are typically on multiple medications simultaneously, an ERA, a PDE5 inhibitor, and sometimes a prostacyclin agent. Coordinating a generic switch across a complex regimen requires specialist oversight.
The Opsynvi combination product creates a commercial counterweight: patients already on both macitentan and tadalafil have a clinically reasonable path to consolidate onto a single branded pill rather than take two generic pills separately. Whether that simplification justifies the price difference is a judgment that will play out differently across payer and patient circumstances.
What This Means for Patients
If you are currently taking Opsumit, do not make any changes to your regimen without discussing it with your PAH specialist. In a disease this serious, where treatment interruption or dosing errors carry real clinical risk, the appropriate channel for a formulary transition is through your prescribing center, not a pharmacist acting unilaterally.
What should prompt that conversation: if your insurer notifies you of a formulary change toward generic macitentan, ask your specialist to review the transition with you. The clinical content of the treatment is identical. The REMS enrollment carries over. The switch should be medically straightforward, but any change in an active PAH regimen is worth documenting in your clinical record.
For patients who have been diagnosed with PAH but face barriers to accessing Opsumit through inadequate insurance coverage, prior authorization hurdles, or cost-sharing burdens: the arrival of generic competition over the next 12 to 24 months should create new formulary access opportunities. The Pulmonary Hypertension Association maintains a patient services team and can assist with navigating access and financial assistance resources. Johnson and Johnson’s patient assistance program for Opsumit also remains available while the brand is on the market.
For patients not yet on PAH-targeted therapy who may have been waiting for cost reasons: the right starting point is always a referral to a center with PAH expertise, not a generic launch. PAH management requires right-heart catheterization for definitive diagnosis, risk stratification, and an individualized treatment plan that accounts for disease severity, associated conditions, and treatment goals.
For related HED coverage on how biosimilar and generic market entry intersects with complex disease management, see Post 2 of this series on generic pomalidomide (Pomalyst) and the persistent REMS requirements that apply across brand and generic versions, and our post on Immgolis and Immgolis Intri, the first biosimilars to golimumab (Simponi), which also covers why FDA approval does not equal immediate commercial availability when patent litigation is involved.
Sources
SERAPHIN primary publication: Pulido T et al. Macitentan and Morbidity and Mortality in Pulmonary Arterial Hypertension. New England Journal of Medicine. 2013;369(9):809–818. doi:10.1056/NEJMoa1213917.
SERAPHIN trial registration: NCT00660179. ClinicalTrials.gov.
Opsynvi FDA approval (March 2024): FDA approves macitentan and tadalafil (Opsynvi) for pulmonary arterial hypertension. FDA.gov.
A DUE trial registration: NCT03903172. ClinicalTrials.gov.
Opsynvi A DUE trial coverage: FDA Approves Macitentan, Tadalafil Combination Tablet for PAH. AJMC. March 2024.
Opsumit FDA approval: FDA approves macitentan (Opsumit) for pulmonary arterial hypertension. FDA.gov. October 2013.
Optum LOE market context: Blockbuster drug patent expirations in 2026 and what they mean. business.optum.com. April 2026.
Generic macitentan approvals: Is there a generic for Opsumit? MedxDrg. December 2025.
Macitentan mechanism and tissue penetration review: Treatment of PAH with the dual ERA macitentan: clinical evidence and experience. PMC6376529.
ERA slow receptor dissociation kinetics: Gatfield J et al. Slow Receptor Dissociation Kinetics Differentiate Macitentan from Other ERAs. PLOS ONE. 2012. PMC3471877.
ERA comparative safety network meta-analysis: Comparative safety of endothelin receptor antagonists in PAH. Pulmonary Circulation. 2018. PMID 30069483.
PAH survival statistics and epidemiology: Emmons-Bell S et al. Prevalence, incidence, and survival of PAH: a systematic review for the GBD 2020 study. Pulmonary Circulation. 2022. doi:10.1002/pul2.12020.
PAH pathophysiology: Pulmonary Arterial Hypertension. StatPearls. NCBI.
WHO functional classification in PAH: WHO Functional Classification in Pulmonary Hypertension. PMC6195065.
SERAPHIN landmark context (PMC): Macitentan in PAH: the SERAPHIN trial. PMC4220429.
ESC PAH guidelines: ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension. escardio.org.
Right-heart catheterization: Right Heart Catheterization. StatPearls. NCBI.
NHLBI PAH overview: Pulmonary Hypertension. NHLBI.
FDA REMS resources: REMS Program Resources. FDA.gov.
Opsumit prescribing information: Opsumit (macitentan) Prescribing Information. Johnson & Johnson/Actelion.
Janssen patient assistance: Janssen CarePath. janssencarepath.com.
Patient resources: Pulmonary Hypertension Association | American Thoracic Society patient education | NHLBI Pulmonary Hypertension
| Disclaimer: Health Evidence Digest provides general information about FDA approvals, loss of exclusivity events, and health research for educational purposes. This content is not a substitute for professional medical advice. Pulmonary arterial hypertension is a serious, progressive disease requiring management by specialist physicians at certified PAH centers. Patients should not make any changes to their PAH treatment regimen without consulting their prescribing specialist. Drug pricing information reflects figures at time of publication and is subject to change. |
|---|
Leave a Reply