
| 📌 The essentials On June 26, 2026, the FDA approved Lumvoa (veligrotug-vvze, Viridian Therapeutics) for the treatment of thyroid eye disease (TED) in adults. Lumvoa is the second FDA-approved pharmacologic therapy for TED, following teprotumumab (Tepezza, Amgen/Horizon), which was approved in 2020 for active TED. What makes Lumvoa distinct: it is the first FDA-approved treatment for TED with labeling that includes clinical data in both active and chronic TED, making it the first therapy with a regulatory basis for use across the full disease spectrum. Mechanism: veligrotug is a full antagonist of the insulin-like growth factor-1 receptor (IGF-1R), a humanized monoclonal antibody that completely blocks IGF-1R signaling. This distinguishes it from teprotumumab, which is a partial/mixed agonist-antagonist. Regulatory designations: Breakthrough Therapy Designation; Priority Review. Clinical basis: Phase 3 THRIVE (NCT05176639) in active TED and Phase 3 THRIVE-2 (NCT06021054) in chronic TED. Both trials met their primary endpoint and all secondary endpoints at week 15 with high statistical significance. THRIVE (active TED, n=113): Proptosis Responder Rate (PRR) 70% versus 5% placebo (p less than 0.0001); mean proptosis reduction 2.9 mm versus 0.5 mm; diplopia complete resolution 54% versus 12% (p less than 0.0001). THRIVE-2 (chronic TED, n=188): PRR 56% versus 8% (p less than 0.0001); mean proptosis reduction 2.34 mm versus 0.46 mm; diplopia improvement 56% versus 25% (p=0.0006); diplopia complete resolution 32% versus 14% (p=0.0152). Rapid onset: statistically significant proptosis reduction observed as early as week 3 (after one infusion) in both trials. Treatment course: 5 intravenous infusions administered every 3 weeks (infusions at weeks 0, 3, 6, 9, 12; primary analysis at week 15). Shorter infusion course than teprotumumab (8 infusions). Key safety: infusion reactions approximately 9%; hyperglycemia 12% including patients without pre-existing diabetes; hearing impairment (class risk); muscle spasms most common adverse reaction. Available now: commercial launch immediately following approval. |
|---|
Thyroid eye disease is one of those conditions that sounds manageable until you understand what it actually does to the people who have it. The immune system targets the tissues behind and around the eye — the orbital fat, the extraocular muscles, the connective tissue. The result can include forward protrusion of the eyeball (proptosis) that makes it impossible to close the eye fully, double vision that prevents driving or reading or functioning normally, and pain behind the eyes that is present with every eye movement. At its most severe, the expansion of orbital tissue compresses the optic nerve, threatening permanent vision loss.
Before 2020, the only systemic treatment for TED was intravenous corticosteroids, which reduce inflammation but do not address the underlying disease mechanism. In 2020, teprotumumab (Tepezza) became the first drug approved specifically for TED, targeting the insulin-like growth factor-1 receptor (IGF-1R) and demonstrating that the proptosis and diplopia of TED could be substantially reversed pharmacologically.
Lumvoa (veligrotug-vvze, Viridian Therapeutics), approved June 26, 2026, is the second drug approved for TED — and the first with regulatory labeling that includes data across the full disease spectrum, both active and chronic phases. The THRIVE and THRIVE-2 Phase 3 trials demonstrated not only that veligrotug works in both phases, but that it works rapidly, producing statistically significant proptosis reduction after just one infusion in week 3, with diplopia improvements that are among the most robust data ever generated for any TED therapy.
What Thyroid Eye Disease Is and Why the Active/Chronic Distinction Matters
Thyroid eye disease is a rare autoimmune orbitopathy most commonly associated with Graves disease, a condition in which autoantibodies against the thyroid-stimulating hormone receptor (TSHR) drive overproduction of thyroid hormone. In TED, those same autoantibodies, along with antibodies to IGF-1R, activate fibroblasts in the orbital fat and extraocular muscles, triggering inflammation, glycosaminoglycan accumulation, and remodeling of the orbital soft tissues. The result is a progressive expansion of orbital volume that pushes the eyeball forward (proptosis) and impairs the function of the muscles that move it (causing diplopia and limiting motility).
TED affects approximately 16 to 19 adults per 100,000, primarily those with Graves disease, though it can occur in euthyroid or hypothyroid patients with autoimmune thyroid conditions. Women are more commonly affected than men.
The active and chronic phases: why they are clinically distinct
| Disease phase | Definition | Characteristics | Clinical significance |
|---|---|---|---|
| Active TED | Clinical Activity Score (CAS) at or above 3/7; onset within approximately 15 months | Active inflammation; edema; periorbital redness; pain; rapidly changing proptosis | Amenable to anti-inflammatory intervention; spontaneous partial remission possible |
| Chronic TED | CAS below 3; disease onset more than 15 months ago | Fibrosis and remodeling dominate over active inflammation; proptosis is stable; diplopia is fixed | Less responsive to corticosteroids; fibrotic changes once thought irreversible; surgical intervention (orbital decompression, strabismus surgery, eyelid surgery) traditionally the primary option |
This distinction has historically defined treatment options. Teprotumumab’s pivotal trial was conducted in active TED, and its label is primarily supported by data in this phase. Patients with chronic TED, who have passed through the active inflammatory phase into a state dominated by fibrotic orbital remodeling, have had essentially no systemic pharmacologic options except orbital decompression surgery.
The THRIVE-2 trial, conducted specifically in chronic TED, is the first global Phase 3 randomized controlled trial to demonstrate statistically significant improvement in both proptosis and diplopia in this population. That is the clinical significance of Lumvoa’s “both active and chronic” labeling.
The Science: Why IGF-1R Is the Target and What “Full Antagonist” Means
The IGF-1R/TSHR cross-talk mechanism
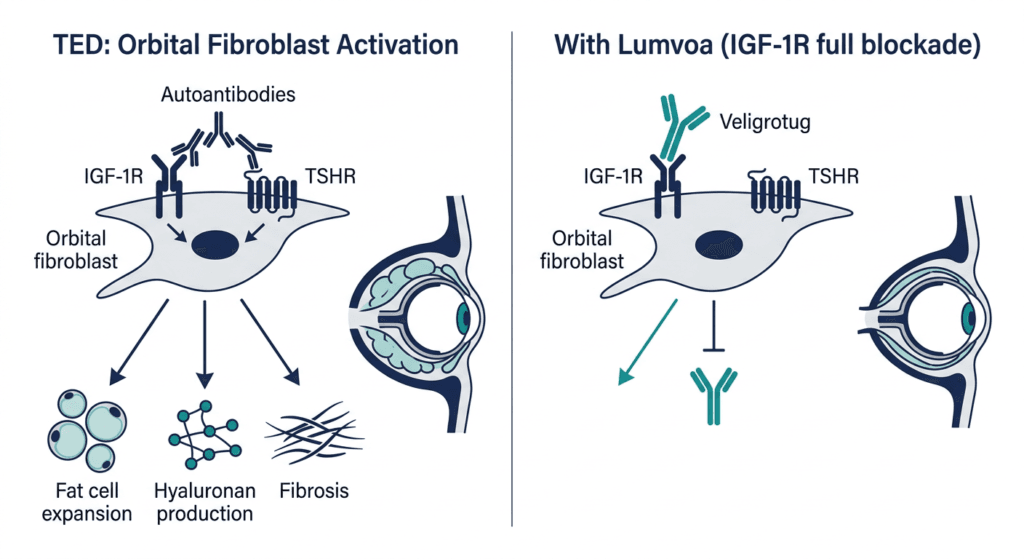
The pathogenesis of TED involves a synergistic interaction between two surface receptors on orbital fibroblasts: the thyroid-stimulating hormone receptor (TSHR) and the insulin-like growth factor-1 receptor (IGF-1R). These two receptors form a physical complex on the fibroblast surface and engage in molecular cross-talk: activation of one sensitizes or amplifies signaling through the other.
In TED, autoantibodies against TSHR and IGF-1R activate this fibroblast complex, driving: expansion of orbital preadipocytes into mature fat cells (hyaluronan-producing adipogenesis); differentiation of fibroblasts into myofibroblasts that produce the fibrous connective tissue that hardens the orbital fat; and production of hyaluronic acid and glycosaminoglycans that attract water, expanding orbital volume further. The combination of fat expansion, glycosaminoglycan accumulation, and fibrotic remodeling produces the characteristic proptosis, restricted ocular motility, and diplopia of TED.
IGF-1R inhibition interrupts this fibroblast activation cascade at the receptor level. By blocking IGF-1R, the downstream signaling pathways (PI3K/Akt, MAPK/ERK) that drive fibroblast proliferation, differentiation, and hyaluronan synthesis are suppressed. The anti-inflammatory effect follows: the cycle of immune cell recruitment driven by fibroblast activation slows, and the structural remodeling that produces proptosis is interrupted.
Full antagonist versus partial agonist-antagonist: the distinction from teprotumumab
Veligrotug is described as a full antagonist of IGF-1R. This is a specific pharmacological claim that distinguishes it from teprotumumab.
Teprotumumab acts as a partial agonist at IGF-1R in certain contexts: while it blocks much of IGF-1R’s downstream signaling, it also produces some residual IGF-1R activation through the receptor before its internalization and degradation. Veligrotug, by contrast, binds the receptor and completely blocks signaling without producing any agonist activation. The clinical relevance of this pharmacological distinction is an active area of investigation, but the theoretical benefit of full antagonism is the absence of any compensatory receptor activation that might limit or counterbalance the therapeutic blockade.
The “full antagonist” distinction is included in Lumvoa’s approved labeling, which is clinically notable. It is not a marketing description; it is a regulatory characterization of the drug’s pharmacological mechanism supported by preclinical and clinical evidence provided to the FDA.
The THRIVE and THRIVE-2 Trials: Complete Data
THRIVE: Phase 3 in active TED
THRIVE (NCT05176639) was a randomized, double-masked, placebo-controlled Phase 3 trial enrolling adults with moderate-to-severe active TED, defined by CAS at or above 3/7, proptosis at or above 3 mm, and disease onset within 15 months of screening.
Patients were randomized to veligrotug 10 mg/kg IV or placebo, administered every 3 weeks for 5 total infusions (at weeks 0, 3, 6, 9, and 12), with the primary analysis at week 15. The trial enrolled 113 patients (75 veligrotug; 38 placebo).
| Endpoint at week 15 | Veligrotug | Placebo | p-value |
|---|---|---|---|
| Proptosis Responder Rate (PRR by Hertel) | 70% | 5% | p less than 0.0001 |
| PRR by MRI/CT | 69% | 9% | p less than 0.0001 |
| Mean proptosis reduction | 2.9 mm | 0.5 mm | p less than 0.0001 |
| Mean CAS reduction | 3.4 points | 1.7 points | p less than 0.0001 |
| Diplopia complete resolution (in patients with diplopia at baseline) | 54% (27/50) | 12% (3/26) | p less than 0.0001 |
| PRR statistically significant from week 3 (after 1 infusion) | Yes | — | p less than 0.0001 |
Source: Endocrine Practice THRIVE topline results abstract. 2025. PMC12545473. THRIVE NCT05176639.
The 70% proptosis responder rate at week 15 — compared to 5% for placebo — is a dramatic treatment effect. The 54% complete diplopia resolution rate in patients who had diplopia at baseline is particularly notable: more than half of patients with double vision resolved it completely within 15 weeks of treatment.
The rapid onset finding deserves specific attention. Statistical significance in proptosis reduction was achieved at week 3, after only a single infusion. This speed of response is faster than what was observed in the teprotumumab clinical trials and has direct clinical significance: patients and clinicians can assess whether treatment is working within the first month rather than waiting for the full course to complete.
THRIVE-2: Phase 3 in chronic TED
THRIVE-2 (NCT06021054) used the same treatment design but enrolled adults with moderate-to-severe chronic TED, defined as disease onset more than 15 months before screening and proptosis at or above 3 mm with any CAS value. The mean time since TED onset in enrolled patients was 69.8 months — nearly 6 years — making this a population in whom fibrotic remodeling had been accumulating for a substantial period. The trial enrolled 188 patients (125 veligrotug; 63 placebo) with a 2:1 randomization.
| Endpoint at week 15 | Veligrotug | Placebo | p-value |
|---|---|---|---|
| Proptosis Responder Rate (PRR by Hertel) | 56% | 8% | p less than 0.0001 |
| PRR by MRI/CT | 48% | 3% | p less than 0.0001 |
| Mean proptosis reduction | 2.34 mm | 0.46 mm | p less than 0.0001 |
| Overall Responder Rate | 56% | 7% | p less than 0.0001 |
| Diplopia improvement (Gorman scale; in patients with diplopia at baseline) | 56% | 25% | p=0.0006 |
| Diplopia complete resolution (Gorman scale) | 32% | 14% | p=0.0152 |
| CAS of 0 or 1 achieved (patients with CAS at or above 3 at baseline) | 54% | 24% | p=0.0060 |
| PRR statistically significant from week 3 (after 1 infusion) | Yes | — | — |
Source: Endocrine Practice THRIVE-2 publication. 2025. doi:10.1016/j.eprac.2025. NCT06021054.
THRIVE-2 is the first randomized controlled trial in chronic TED to demonstrate statistically significant improvement in both proptosis and diplopia. The finding that 56% of chronic TED patients achieved a proptosis response, in a disease phase previously considered refractory to systemic pharmacotherapy, challenges the historical assumption that fibrotic TED could only be addressed surgically.
The 32% complete diplopia resolution rate in chronic TED patients with diplopia is also clinically significant: for a patient who has had double vision for years, the possibility of complete resolution from a 12-week course of infusions represents a meaningful departure from the trajectory that orbital decompression, strabismus surgery, and eyelid surgery were previously the only path toward.
How Lumvoa Compares to Tepezza: A Clinical Summary
Teprotumumab (Tepezza) was the first drug ever approved for TED and established proof of concept for IGF-1R inhibition in this disease. Lumvoa enters the same mechanistic space with several clinically meaningful differences.
| Feature | Lumvoa (veligrotug) | Tepezza (teprotumumab) |
|---|---|---|
| Mechanism | Full IGF-1R antagonist | Partial agonist-antagonist at IGF-1R |
| Active TED data | Yes (THRIVE Phase 3) | Yes (pivotal Phase 2 and Phase 3) |
| Chronic TED data | Yes (THRIVE-2 Phase 3; first RCT in chronic TED with positive diplopia data) | Limited; label primarily supported by active TED data |
| Number of infusions | 5 infusions over 12 weeks | 8 infusions over 21 weeks |
| Dose | 10 mg/kg IV every 3 weeks | 10 mg/kg first infusion, then 20 mg/kg every 3 weeks |
| Onset of proptosis response | Week 3 (after 1 infusion) | Week 6 (after 2 infusions) |
| Hyperglycemia rate | Approximately 12% | Approximately 10% |
| Hearing impairment | Reported (class risk; approximately 16% in THRIVE active TED) | Reported (class risk; approximately 10 to 29% in trials) |
| Chronic TED diplopia resolution | 32% complete resolution (THRIVE-2) | Not established in a dedicated chronic TED Phase 3 RCT |
Sources: Viridian THRIVE/THRIVE-2 data; Tepezza FDA approval and prescribing information.
The most clinically significant difference for prescribers is the combination of fewer infusions and the chronic TED data. From a patient experience standpoint, 5 infusions over 12 weeks is a substantially lighter treatment burden than 8 infusions over 21 weeks. Infusion center visits for a condition that already carries significant quality-of-life burden matter.
Dr. Michael Yen, MD, Professor of Oculoplastic Surgery and Ophthalmology at Baylor College of Medicine and an investigator in the THRIVE program, noted that the clinical data demonstrated meaningful improvements across the full spectrum of TED, including rapid reductions in proptosis and significant improvements in diplopia, in both the active and chronic disease settings.
An important note on indirect comparison: THRIVE and THRIVE-2 were not head-to-head trials against teprotumumab. The efficacy numbers from Lumvoa’s trials should not be used for direct numeric comparison against teprotumumab’s trials. Patient populations, trial designs, and baseline characteristics differed across programs. What can be said is that both drugs demonstrated substantial, statistically significant, clinically meaningful benefits in their respective trials, and that Lumvoa now adds a Phase 3 evidence base in chronic TED where Tepezza’s regulatory support was limited.
Safety: What Prescribers and Patients Need to Know
Lumvoa’s safety profile is consistent with the IGF-1R inhibitor class established by teprotumumab, with some differences in rate and pattern across specific adverse events.
Most common adverse reactions (occurring in 5% or more of patients):
Muscle spasms were the most common adverse event overall, reported in approximately 36% of veligrotug-treated patients versus 6% of placebo patients in THRIVE-2. While striking in relative frequency, the muscle spasms were predominantly mild in severity and rarely led to treatment discontinuation. Other common adverse reactions include headache, fatigue, diarrhea, nausea, nasopharyngitis, elevated creatine phosphokinase, dry skin, and hypertension.
Key warnings and precautions:
Infusion reactions: Infusion-related reactions occurred in approximately 9% of Lumvoa-treated patients in the THRIVE program. Most were mild to moderate. Premedication before infusions and clinical monitoring during administration are standard management. Patients should be observed during and after each infusion.
Hyperglycemia: Hyperglycemia was reported in approximately 12% of veligrotug-treated patients, including patients without pre-existing diabetes. IGF-1R inhibition affects insulin signaling, and glucose elevation is a class effect shared with teprotumumab. Blood glucose should be monitored before and during treatment, particularly in patients with diabetes or prediabetes. Dose modification or antidiabetic medication adjustment may be required.
Hearing impairment: Hearing impairment, including potentially permanent hearing loss, is identified as a risk in Lumvoa’s prescribing information. This is a class effect of IGF-1R inhibitors in TED. In the THRIVE trials, hearing-related adverse events were reported in approximately 13% to 16% of veligrotug-treated patients in the active and chronic TED trials, with a placebo-adjusted rate of approximately 9.6% in THRIVE-2. Patients should be counseled about this risk before treatment initiation. Audiologic evaluation before and during treatment is clinically appropriate, and patients should report any new hearing changes promptly.
Inflammatory bowel disease: The prescribing information includes a risk of inflammatory bowel disease exacerbation. Patients with a history of inflammatory bowel disease should be evaluated carefully before initiating Lumvoa.
Embryo-fetal toxicity: Based on its mechanism of action affecting IGF-1R signaling, Lumvoa may cause fetal harm. Females of reproductive potential should use effective contraception during treatment and for a specified period after the final infusion. Pregnancy testing before initiating treatment is appropriate.
Serious adverse events: Serious treatment-emergent adverse events in THRIVE were reported in 4 veligrotug-treated patients, all assessed as unrelated to treatment. Serious adverse events in THRIVE-2 occurred in 2% of veligrotug patients versus 3% of placebo patients. Treatment completion rates were high: 94% of veligrotug-treated patients in THRIVE-2 completed their full treatment course, a retention rate that speaks to the overall tolerability of the regimen.
What This Means for Patients and Clinicians
For patients with active TED
Lumvoa provides a second approved systemic pharmacologic option for active TED, alongside teprotumumab. The clinical discussion with an ophthalmologist or oculoplastic surgeon experienced in TED should now include both options, weighing the specific clinical profile, the shorter infusion course, the full antagonist mechanism, and individual patient factors including diabetes status, hearing risk, and infusion access.
For patients who have previously received teprotumumab and experienced disease recurrence or inadequate response, Lumvoa’s distinct pharmacological profile as a full antagonist represents a mechanistically differentiated alternative. Whether prior IGF-1R therapy exposure affects veligrotug response is a question that ongoing clinical experience will address. The THRIVE trials excluded patients who had received prior anti-IGF-1R therapy, so the evidence in this subgroup is not yet established.
For patients with chronic TED
This is the population for whom Lumvoa’s approval is most transformative. Until now, patients in the chronic phase of TED with established proptosis and fixed diplopia faced a choice between living with these manifestations or pursuing surgical correction: orbital decompression for proptosis, strabismus surgery for diplopia, and eyelid surgery for cosmetic and functional restoration. These surgeries are effective but carry their own risks and often require sequential procedures.
The THRIVE-2 data demonstrates that pharmacologic reversal of chronic TED manifestations is achievable in a meaningful proportion of patients. A 56% proptosis response rate and 32% complete diplopia resolution in a population with a mean TED onset of nearly 6 years challenges the assumption that fibrotic orbital changes are irreversible. For patients and clinicians managing chronic TED, a conversation about whether a 12-week course of Lumvoa infusions might reduce or eliminate the need for surgical intervention is now evidence-supported.
Christine Gustafson, Founder and Executive Director of the TED Community Organization, noted that a new treatment option could benefit many patients living with the physical and emotional burden of thyroid eye disease. The psychosocial burden of TED is well-documented: disfiguring proptosis, double vision that impairs independence, and pain with eye movement contribute to depression, social withdrawal, and reduced quality of life that persist well beyond the active inflammatory phase.
Practical access and administration
Lumvoa launched commercially on June 26, 2026, the same day as FDA approval. Treatment requires intravenous infusion access, which means a certified infusion center or hospital outpatient setting. The 5-infusion schedule over 12 weeks, with infusions every 3 weeks, represents a meaningful reduction in infusion center visits compared to teprotumumab’s 8-infusion protocol. Viridian has established a patient support program to assist with access, insurance navigation, and infusion site coordination.
For related HED coverage on autoimmune and rare endocrine conditions, see our post on Tzield (teplizumab) approved as the first disease-modifying therapy for recently diagnosed Stage 3 type 1 diabetes and our post on Hympavzi (marstacimab) expanding to cover children aged 6 to 11 and inhibitor-positive hemophilia patients.
Sources
Viridian FDA approval press release: Viridian Therapeutics Announces U.S. FDA Approval and Launch of Lumvoa (veligrotug-vvze) for the Treatment of Thyroid Eye Disease. BusinessWire. June 26, 2026.
Eyewire clinical summary: FDA Approves Viridian’s Lumvoa for Thyroid Eye Disease. eyewire.news. June 2026.
Pharmacally detailed clinical coverage: FDA Approves Veligrotug as First Treatment for Active and Chronic Thyroid Eye Disease. pharmacally.com. June 2026.
Ophthalmology Times (full safety and mechanism detail): FDA approves veligrotug-vvze (Lumvoa) for thyroid eye disease across active and chronic stages. ophthalmologytimes.com. June 2026.
Optometry Times: FDA approves Lumvoa (veligrotug-vvze) for active and chronic thyroid eye disease. optometrytimes.com. June 2026.
HCPLive BLA acceptance coverage: FDA Accepts, Grants Priority Review to Veligrotug BLA for Thyroid Eye Disease. hcplive.com. March 2026.
THRIVE topline results (Endocrine Practice): Efficacy and Safety of Veligrotug, a Full Antagonist Monoclonal Antibody to IGF-1 Receptor, in Active Thyroid Eye Disease: THRIVE Phase 3 Topline Results. Endocrine Practice. 2025.
THRIVE PMC abstract: OR31-04 Efficacy and Safety of Veligrotug in Active TED: THRIVE Phase 3 Topline Results. PMC12545473.
THRIVE-2 primary results (Endocrine Practice): THRIVE-2 Phase 3 Trial of Veligrotug in Chronic Thyroid Eye Disease: Efficacy and Safety at 15 Weeks. Endocrine Practice. 2025.
THRIVE-2 topline press release (Viridian): Viridian Therapeutics Announces Positive Topline Results from Veligrotug Phase 3 THRIVE-2 Clinical Trial. ir.viridiantherapeutics.com. 2024.
THRIVE trial registration: NCT05176639. ClinicalTrials.gov.
THRIVE-2 trial registration: NCT06021054. ClinicalTrials.gov.
Viridian BLA acceptance and Priority Review: Viridian Therapeutics Announces BLA Acceptance and Priority Review for Veligrotug. ir.viridiantherapeutics.com. 2025.
Teprotumumab FDA approval: FDA approves teprotumumab-trbw for thyroid eye disease. FDA.gov. January 2020.
IGF-1R biology: IGF-1R in autoimmune disease. PMC6126283.
Thyroid eye disease overview: Thyroid Eye Disease. StatPearls. NCBI.
Graves disease overview: Graves Disease. NIDDK.
Lumvoa prescribing information: LUMVOA (veligrotug-vvze) Prescribing Information. Viridian Therapeutics. 2026.
Patient resources: TED Community Organization | American Thyroid Association: TED patient resources | Viridian Lumvoa patient support
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice. Thyroid eye disease management, including the decision to initiate pharmacologic therapy with Lumvoa or Tepezza, requires individualized evaluation by a board-certified ophthalmologist, oculoplastic surgeon, or endocrinologist with experience in TED. Patients with active or chronic TED should discuss all systemic treatment options with their managing specialist before initiating therapy. |
|---|
Leave a Reply