
| 📌 The essentials Briviact (brivaracetam, UCB) is an oral antiseizure medication (ASM) approved in February 2016 for adjunctive treatment of focal (partial-onset) seizures in patients aged 1 month and older. It is available as tablets (10 mg, 25 mg, 50 mg, 75 mg, 100 mg), an oral solution (10 mg/mL), and an intravenous solution. Mechanism: SV2A (synaptic vesicle protein 2A) inhibitor. Brivaracetam shares its mechanism class with levetiracetam (Keppra) but binds SV2A with 15 to 30 times higher affinity and penetrates the brain faster. At therapeutic doses it is predicted to occupy more than 80% of SV2A in the human brain. The key clinical differentiation from levetiracetam: substantially lower rates of behavioral and psychiatric side effects (irritability, aggression, mood disturbance), the most clinically significant limitation of levetiracetam in practice. Briviact generated approximately $652 million in U.S. sales in 2025. Generic status: generics are already entering the U.S. market. UCB’s own patient-facing materials acknowledge this directly. At least one full FDA approval for generic brivaracetam was issued as early as June 2022 (Sunshine Lake Pharma); twelve companies have filed for generic approval; five tentative approvals exist. Brand list price: approximately $650 to $800 per month for 100 mg twice daily. Expected generic price with multi-source competition: $50 to $100 per month. Phase 3 pivotal trials: approximately 38 to 42% of patients achieved a 50% or greater reduction in seizure frequency at 100 mg per day. Statistically significant seizure reduction was demonstrated even in patients who had failed five or more prior antiseizure medications. Critical prescribing caution: brivaracetam and levetiracetam should not be co-administered at therapeutic doses. Both compete for the same SV2A binding site, reducing brivaracetam efficacy. Cross-taper required when transitioning. |
|---|
| 📚 About this series: the 2026 Loss of Exclusivity Watch This is Post 9 of HED’s 2026 Loss of Exclusivity series, tracking the ten major drugs losing U.S. exclusivity this year. The full series covers: Xolair (omalizumab) • Pomalyst (pomalidomide) • Opsumit (macitentan) • Januvia/Janumet (sitagliptin) • Simponi (golimumab) • Mavenclad (cladribine) • Gattex (teduglutide) • Trintellix (vortioxetine) • Briviact (brivaracetam) • Xeljanz (tofacitinib). Each post follows the same format: what the drug is and how it works, what the clinical evidence shows, who uses it and why, and what the entrance of competition means for patients, prescribers, and the market. |
|---|
Epilepsy is one of the most common serious neurological conditions in the world. Approximately 3.4 million Americans live with active epilepsy, and roughly 150,000 new cases are diagnosed each year in the United States alone. For the majority of patients, antiseizure medications manage the condition well enough to allow normal daily functioning. For about one-third, however, seizures remain inadequately controlled despite multiple medication trials, a population with enormous unmet need and, for many, a daily reality shaped by unpredictable neurological events that affect their ability to drive, work, care for their families, and move through the world safely.
Briviact (brivaracetam), developed by the Belgian biopharmaceutical company UCB, was FDA-approved in February 2016 for the adjunctive treatment of focal (partial-onset) seizures in patients aged 1 month and older. It belongs to the same drug class as levetiracetam (Keppra), one of the most widely prescribed antiseizure medications globally, but is not the same drug. Brivaracetam displays higher selectivity and affinity for synaptic vesicle protein 2A (SV2A) in the brain than levetiracetam. That distinction in receptor pharmacology translates into meaningful clinical differences, particularly in the behavioral and psychiatric side effect profile that has long been levetiracetam’s most significant clinical limitation.
Briviact generated approximately $652 million in U.S. sales in 2025. Generics are already entering the U.S. market. UCB’s own patient-facing website acknowledges this directly, stating that patients may notice generic versions of Briviact becoming available because the medicine’s patent is expiring.
The LOE story for brivaracetam is less dramatic than some others in this series: no litigation standoff, no manufacturing CRL, no biosimilar complexity. Generics are arriving. For patients currently on Briviact at brand-name prices, the cost relief is real and the transition should be clinically straightforward. But to understand what is being preserved when a patient transitions to generic brivaracetam, and why the drug’s specific receptor pharmacology was worth developing in the first place, requires going inside the science of SV2A, one of the more unusual drug targets in all of neurology.
What Epilepsy Is and Why Focal Seizures Are the Focus
Epilepsy is defined by the International League Against Epilepsy as a disease characterized by at least two unprovoked seizures occurring more than 24 hours apart, or one unprovoked seizure with a high probability of further seizures based on brain imaging or other factors. Seizures are the visible manifestation of abnormal, synchronous electrical activity across networks of neurons, either a localized discharge that remains focal or one that spreads to involve the entire brain.
The classification of seizure types has clinical importance because different seizure types respond to different drug mechanisms, and because the experience of a seizure is highly variable depending on where in the brain the discharge originates:
| Seizure type | Origin | Common experience | Key treatment consideration |
|---|---|---|---|
| Focal onset (aware) | Localized cortical region, consciousness preserved | Strange feelings, déjà vu, unusual smells or tastes, repetitive movements, emotional changes | Brivaracetam, levetiracetam, lacosamide, lamotrigine, carbamazepine |
| Focal onset (impaired awareness) | Localized region, consciousness affected | Automatisms (lip smacking, hand movements), confusion, amnesia for the event | Same class options; seizure impact on daily function significant |
| Focal to bilateral tonic-clonic | Focal onset spreading to both hemispheres | Convulsions, loss of consciousness, post-ictal fatigue | Multiple agents; drug-resistant disease common |
| Generalized onset | Both hemispheres simultaneously from onset | Absence, myoclonic jerks, tonic-clonic episodes | Different drug profile; some focal ASMs ineffective |
Brivaracetam is indicated for focal (partial-onset) seizures specifically. It is not approved for generalized epilepsy syndromes such as juvenile myoclonic epilepsy or absence epilepsy in the same way as some broader-spectrum agents. This specificity matters when evaluating its place in the treatment landscape.
The one-third of epilepsy patients with drug-resistant disease, defined as failure of two adequate trials of appropriately chosen and tolerated antiseizure medications, face a different clinical and quality-of-life reality from those who achieve seizure freedom early. For this population, the ongoing search for better-tolerated, more effective adjunctive agents is the difference between driving and not driving, working and not working, independent living and supervised care.
The SV2A Target: What It Is and Why It Matters
The mechanism shared by both levetiracetam and brivaracetam is one of the more scientifically unusual in clinical neuroscience. Both drugs bind to synaptic vesicle protein 2A (SV2A), a protein embedded in the membrane of synaptic vesicles inside neurons. Understanding what SV2A does, and why binding to it controls seizures, requires a brief look at how synaptic transmission works.
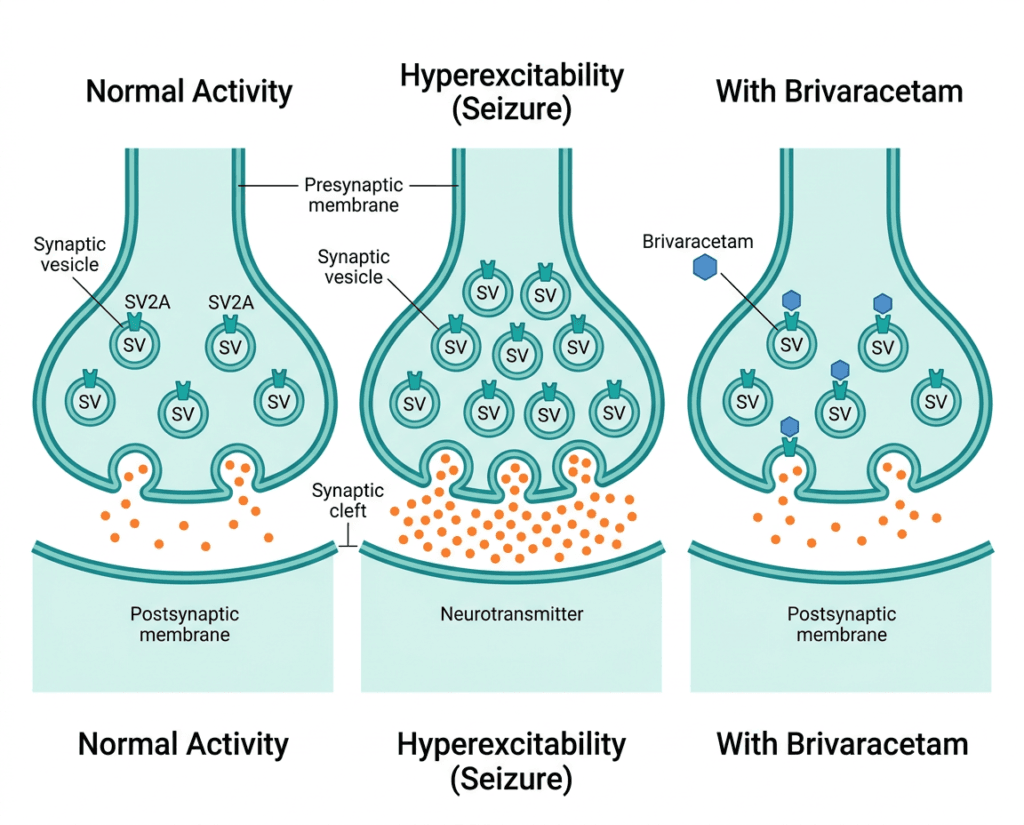
Neurons communicate at synapses by releasing neurotransmitters into the synaptic cleft. These neurotransmitters are stored in small membrane-bound packages called synaptic vesicles. When an action potential arrives at the presynaptic terminal, voltage-gated calcium channels open, calcium flows in, and the vesicles fuse with the presynaptic membrane to release their contents into the cleft in a process called exocytosis.
SV2A is a transmembrane glycoprotein expressed in virtually all neurons throughout the central nervous system. It contributes to calcium-sensitive exocytosis of transmitters through interaction with synaptotagmin, vesicular transport, stabilization of vesicular neurotransmitter loading, and regulation of calcium sensitivity. In practical terms: SV2A is part of the molecular machinery regulating how readily vesicles release neurotransmitter in response to neuronal activity.
In epilepsy, the problem is neuronal hyperexcitability: networks of neurons that fire too synchronously and too readily, creating the electrical storm of a seizure. By modulating SV2A, levetiracetam and brivaracetam dampen the readiness of vesicles to release neurotransmitter during high-frequency neuronal firing, selectively reducing the excessive synaptic transmission that characterizes seizure activity without broadly suppressing normal neuronal communication.
Both drugs bind selectively to SV2A with at least 100-fold higher affinity compared to SV2B and SV2C, the two related isoforms. This selectivity for the A isoform is thought to be central to the antiseizure effect, since SV2A is expressed in excitatory glutamatergic and inhibitory GABAergic neurons throughout the brain while SV2B and SV2C have more restricted distributions.
What Makes Brivaracetam Different From Levetiracetam
This is the central clinical pharmacology question, because levetiracetam has been generically available since 2008 and costs only a few dollars per month. If brivaracetam were simply levetiracetam with a slightly different structure, its development and $652 million in annual sales would be difficult to justify. The evidence says it is meaningfully different in three ways.
First: substantially higher SV2A affinity. Brivaracetam is a selective, high-affinity SV2A ligand with 15 to 30 times higher affinity than levetiracetam. Based on its affinity and pharmacokinetic parameters, at therapeutic concentrations brivaracetam is predicted to occupy more than 80% of SV2A in the human brain. Higher receptor occupancy at therapeutic doses means more complete target engagement, which may translate into efficacy at lower doses and in patients who have shown partial or incomplete response to levetiracetam.
Second: faster and more complete brain penetration. Brivaracetam has high lipid solubility and rapid brain penetration, with engagement of SV2A within minutes of administration. Levetiracetam’s brain penetration is slower. This pharmacokinetic difference is particularly relevant for intravenous use in acute seizure management, where speed of action matters, and may help explain why brivaracetam can work in some patients where levetiracetam does not achieve adequate SV2A occupancy.
Third: a more favorable behavioral side effect profile. This is the most clinically significant differentiation from a prescriber and patient perspective. Levetiracetam has a well-established adverse effect profile involving irritability, aggression, mood disturbance, and behavioral changes, sometimes severe enough to require drug discontinuation. The mechanism behind this behavioral toxicity is not fully elucidated but is thought to involve off-target effects beyond SV2A.
Brivaracetam’s exceptional selectivity for SV2A and its higher affinity suggest it exhibits superior clinical tolerability compared to levetiracetam. The increased possibility of behavioral abnormalities associated with levetiracetam has driven clinical interest in brivaracetam as an alternative with a cleaner receptor profile.
In clinical practice, the most common reason a neurologist prescribes brivaracetam over levetiracetam is either a patient with prior levetiracetam intolerance due to behavioral effects, or a patient with inadequate seizure control on levetiracetam who the clinician believes may achieve better SV2A occupancy with the higher-affinity compound.
There is one important prescribing caution arising from this relationship: the two drugs should not be used concurrently. Brivaracetam’s efficacy is reduced when levetiracetam is co-administered, because levetiracetam competes with brivaracetam for the same SV2A binding site. The clinical trials that evaluated brivaracetam efficacy excluded patients on concomitant levetiracetam from the efficacy analysis for exactly this reason.
The Clinical Evidence: Three Pivotal Phase 3 Trials
Brivaracetam’s FDA approval was supported primarily by three randomized, double-blind, placebo-controlled Phase 3 trials: N01252 (NCT00490035), N01253 (NCT00464269), and N01358 (NCT01261325), all evaluating adjunctive brivaracetam at doses of 50 to 200 mg per day in adults with uncontrolled focal seizures despite one to two existing antiseizure medications.
The primary endpoint across the pivotal trials was the percentage reduction over placebo in baseline-adjusted focal seizure frequency per 28 days during the 12-week treatment period.
| Trial | N | Doses tested | Seizure frequency reduction versus placebo (100 mg/day) | 50% responder rate (100 mg/day) | Notes |
|---|---|---|---|---|---|
| N01252 | approximately 400 | 20, 50, 100 mg/day | Significant at 100 mg | approximately 40% | Conducted in Europe and India |
| N01253 | approximately 400 | 5, 20, 50 mg/day | Significant at 50 mg (reduction 12.8%, p equals 0.025) | Dose-dependent improvement | Lower doses; 50 mg minimum effective |
| N01358 | approximately 768 | 50, 100, 200 mg/day | Significant at 100 and 200 mg/day | approximately 38 to 42% at 100 to 200 mg/day | Largest pivotal trial; established dose range |
The 50% responder rate, the proportion of patients achieving at least a 50% reduction in seizure frequency, is the benchmark most commonly used in clinical practice to assess whether an antiseizure medication is working meaningfully for an individual patient. Rates of approximately 38 to 42% at the 100 mg dose are consistent with what would be expected from an active adjunctive agent in a refractory focal epilepsy population.
The drug-resistant patient data is particularly informative. In patients with five or more previous antiseizure medications, a highly refractory population, the percentage reduction over placebo in 28-day adjusted focal seizure frequency was 18.1% for 100 mg per day (p equals 0.006) and 19.8% for 200 mg per day (p equals 0.004). Demonstrating statistically significant seizure reduction in patients who have already failed five or more previous medications is clinically meaningful, even if the absolute reduction is modest. For this population, any additional seizure control represents a real change in safety and quality of life.
A later Phase 3 study in adult Asian patients (EP0083) confirmed these findings across a different population: the percentage reduction over placebo was 24.5% (p equals 0.0005) for 50 mg per day and 33.4% (p less than 0.0001) for 200 mg per day. The 50% responder rate was 19.0% for placebo, 41.1% for 50 mg, and 49.3% for 200 mg per day.
The Safety Profile
Brivaracetam’s safety profile is a key part of its clinical story, and the comparison to levetiracetam is front and center.
| Safety item | Details | Clinical guidance |
|---|---|---|
| Somnolence and fatigue | Most common adverse events; dose-dependent; occurred in approximately 15 to 25% of patients at therapeutic doses versus approximately 8 to 10% with placebo. | Counsel patients to avoid driving or operating heavy machinery until individual CNS effects are established. Often improves with continued treatment. |
| Dizziness | Common, dose-dependent; reported in approximately 10 to 12% at 100 to 200 mg/day. | Same caution regarding driving and machinery. Usually mild. |
| Behavioral and psychiatric effects | Substantially less common than with levetiracetam. Irritability, aggression, and mood disturbance reported at rates more comparable to other adjunctive antiseizure medications. | Monitor for mood changes, especially in patients with prior psychiatric history. Lower behavioral burden than levetiracetam is a key clinical differentiator. |
| Suicidal behavior and ideation | Class-level FDA warning for antiseizure medications: increased risk of suicidal thoughts and behavior. | Monitor all patients on antiseizure medications for emergence of new or worsening depressive symptoms, suicidal thoughts, or unusual behavioral changes. |
| Drug interactions: CYP2C19 inhibitors | Brivaracetam is metabolized by CYP2C19. Strong inhibitors (fluconazole, fluvoxamine) may increase brivaracetam plasma concentrations. | Reduce brivaracetam dose by half when co-administered with strong CYP2C19 inhibitors. |
| Drug interactions: rifampin | Strong CYP3A4 and CYP2C19 inducers (rifampin) can reduce brivaracetam levels by up to 45%. | Consider increasing brivaracetam dose when co-administered with rifampin or other strong inducers; monitor seizure control. |
| Drug interactions: levetiracetam | Concurrent use not recommended. Both compete for SV2A binding, reducing brivaracetam efficacy. | Cross-taper required when transitioning from levetiracetam: taper levetiracetam down while titrating brivaracetam up. Do not co-prescribe at therapeutic doses. |
| Renal impairment | Dose adjustment not required for mild to moderate impairment based on renal function alone. | Use with caution in severe renal impairment; monitor closely. |
| Pregnancy | Animal studies showed adverse developmental effects at high exposures. Human teratogenicity risk not fully established. | Discuss contraception and pregnancy planning with all patients of reproductive potential. Encourage pregnancy registry enrollment. |
| Abrupt discontinuation | As with all antiseizure medications, abrupt discontinuation risks seizure recurrence and status epilepticus. | Taper gradually when discontinuing. Never stop brivaracetam abruptly without medical supervision. |
The behavioral tolerability advantage over levetiracetam deserves emphasis. Levetiracetam-induced irritability and aggression, sometimes called “Keppra rage” in patient communities, is not a trivial side effect. It affects family functioning, occupational performance, and quality of life, and is the most commonly cited reason for levetiracetam discontinuation in clinical practice. Brivaracetam’s cleaner SV2A selectivity appears to substantially reduce this risk, making it a genuinely preferred option for patients with prior behavioral side effects on levetiracetam.
The Patent and Generic Landscape: What Has Already Happened
Unlike several other drugs in this series, Briviact’s generic transition is not a future event. It is already underway.
UCB won a patent litigation decision in 2023, with a federal judge upholding the validity of U.S. Patent No. 6,911,461 covering the brivaracetam compound and blocking generic copies until 2026. That protection has now expired. The FDA has approved a generic version of Briviact, and UCB’s own materials acknowledge that patients may see generic versions appearing at their pharmacy.
Twelve different companies have filed for generic approval of Briviact. The manufacturers that have received or are pursuing FDA approval include Aurobindo, Lupin, MSN Laboratories, Zydus Pharmaceuticals, and Sunshine Lake Pharma, among others. Five tentative approvals exist for generic brivaracetam indicating near-term availability, and Sunshine Lake Pharma received a full FDA approval on June 9, 2022, among the first generic approvals for this compound.
With multiple generic manufacturers in the market, the price trajectory follows the standard antiseizure generic pattern: 70 to 85% reductions from brand-name pricing over 12 to 24 months as competition deepens. Briviact’s current list price runs approximately $650 to $800 per month for 100 mg twice daily. Generic brivaracetam is expected to settle at $50 to $100 per month with multi-source competition established.
UCB’s response to the LOE includes a branded patient loyalty program. UCB’s own Briviact savings card page states that even as generic options become available, patients may choose to stay on branded Briviact, and that without specific written instructions pharmacies may automatically dispense a generic version. This is a standard brand retention strategy: copay assistance programs that make the brand financially competitive with the generic at the point of care for commercially insured patients, while the payer bears the higher system-level cost. It slows but does not prevent market conversion.
Where Brivaracetam Fits in the 2026 Epilepsy Treatment Landscape
The antiseizure medication landscape is one of the most crowded in neurology, with more than 30 approved agents in the United States. The SV2A class represents one of the most established modern mechanisms: levetiracetam became a first-line agent for many epilepsy syndromes after its 1999 approval, and brivaracetam has carved out a complementary niche as the higher-affinity, better-tolerated successor.
The key positioning questions for a neurologist in 2026:
Is brivaracetam preferable to levetiracetam as first-line adjunctive therapy for focal epilepsy? The clinical evidence supports brivaracetam’s tolerability advantage, particularly the reduced behavioral side effect burden. However, levetiracetam has decades of real-world safety data, an even broader approved indication range, and costs pennies per day as a generic. Many neurologists use levetiracetam first and reserve brivaracetam for patients who develop behavioral side effects or need a switch.
Is generic brivaracetam bioequivalent to Briviact? Yes. The FDA bioequivalence standard ensures that approved generic brivaracetam delivers the same active ingredient at the same concentration with the same pharmacokinetic profile as the brand. The clinical effect, SV2A binding, seizure suppression, and tolerability profile, is preserved in the generic.
What about the interaction with levetiracetam? This is the most important practical management point for transitions. If a patient is switching from levetiracetam to brivaracetam or generic brivaracetam, the two should not be co-prescribed at full doses. A structured cross-taper, reducing levetiracetam while introducing brivaracetam, is the appropriate approach, managed by the treating neurologist.
The arrival of affordable generic brivaracetam has a particular public health significance for the drug-resistant epilepsy population. Patients cycling through multiple agents in search of seizure control have historically faced barriers to accessing newer, better-tolerated antiseizure medications due to cost and formulary restrictions. With generic brivaracetam entering the market at a fraction of Briviact’s brand price, prescribers have more flexibility to choose the agent best suited to a patient’s tolerability profile rather than the agent most easily covered by their insurance formulary.
What Patients Should Know
If you are currently taking Briviact and your seizures are well controlled: nothing in the generic transition changes the clinical effect of your medication. Generic brivaracetam contains the same active ingredient, at the same dose, with the same pharmacokinetics. If your pharmacy substitutes the generic and you experience any perceived change, whether in tablet appearance, packaging, or tolerability, contact your neurologist. Changes in perception of medication effect are sometimes real and sometimes related to factors unrelated to the drug itself; either way, they are worth reporting.
If you are switching from levetiracetam due to behavioral side effects: generic brivaracetam, now broadly available and significantly less expensive than brand Briviact, may be the option that has been cost-prohibitive for you in the past. Discuss this specifically with your neurologist, not just as an inquiry about a brand-name drug, but as a request to evaluate whether generic brivaracetam is now a realistic option given its changed cost profile.
If you are managing epilepsy in a child: brivaracetam is approved for patients aged 1 month and older. The availability of an oral solution formulation (10 mg/mL) is particularly relevant for young children or patients with swallowing difficulties. Confirm with your pediatric neurologist whether generic versions of both the tablet and oral solution formulations are available and appropriate for your child’s dosing needs.
One final reminder that applies to every patient on any antiseizure medication: never stop or reduce the dose of brivaracetam without medical guidance. Abrupt discontinuation of antiseizure medications risks seizure recurrence, including status epilepticus, regardless of how long the patient has been seizure-free.
For related HED coverage on neurological drug LOE events and CNS approvals in 2026, see our post on Mavenclad (cladribine) losing its MS dosing regimen patents and what the science behind selective immune reconstitution actually shows, and our post on the FDA approval of Ocrevus (ocrelizumab) for pediatric relapsing-remitting MS.
Sources
Briviact FDA approval: FDA approves brivaracetam for partial-onset seizures. FDA.gov. February 2016.
Patent litigation and LOE timing: UCB Wins Patent Order Blocking Copies of Briviact Epilepsy Drug. Bloomberg Law. August 2023. | Top 10 Drugs Losing U.S. Patent Protection in 2026. FDCELL. March 2026.
Generic availability: Generic Briviact Availability. drugs.com. Updated May 7, 2026. | BRIVIACT patent and generic information. DrugPatentWatch.
UCB patient acknowledgment of LOE: Briviact Savings Card and Patient Support. briviact.com.
SV2A mechanism and brivaracetam pharmacology: Klein P, Schiemann J. A review of the pharmacology and clinical efficacy of brivaracetam. PMC5783144. 2018.
SV2A allosteric modulation structural basis: Mechanisms Underlying Allosteric Modulation of Antiseizure Medication Binding to SV2A. PNAS. 2025. doi:10.1073/pnas.2510239122.
Brivaracetam brain penetration and SV2A occupancy: Nicolas JM et al. Brivaracetam, a selective high-affinity SV2A ligand with preclinical evidence of high brain permeability and fast onset of action. Epilepsia. 2016;57(2):201–209. PMID 26663401.
SV2A differential interaction (brivaracetam vs. levetiracetam): Wood MD et al. Evidence for a differential interaction of brivaracetam and levetiracetam with SV2A. Epilepsia. 2017.
Phase 3 pivotal trial program: Klein P, Schiemann J. PMC5783144.
N01252 trial registration: NCT00490035. ClinicalTrials.gov.
N01253 trial registration: NCT00464269. ClinicalTrials.gov.
N01358 trial registration: NCT01261325. ClinicalTrials.gov.
Drug-resistant patient subgroup analysis: Villanueva V et al. Effect of Number of Previous Antiseizure Medications on Efficacy and Tolerability of Adjunctive Brivaracetam. Advances in Therapy. 2021.
Asian patient Phase 3 trial (EP0083): Inoue Y et al. Efficacy, safety, and tolerability of adjunctive brivaracetam in adult Asian patients. Epilepsia Open. 2024. PMC11145603.
Brivaracetam versus levetiracetam behavioral tolerability: Comparison of Effectiveness of Brivaracetam and Levetiracetam for Post-Traumatic Seizure Prophylaxis. PMC11588607.
FDA antiseizure medication suicidality warning: Information on Antiepileptic Drugs (AEDs) and Suicidality. FDA.gov.
Levetiracetam StatPearls: Levetiracetam. StatPearls. NCBI.
Epilepsy StatPearls: Epilepsy. StatPearls. NCBI.
CDC epilepsy data: Epilepsy Data and Statistics. CDC.
Briviact prescribing information: Briviact (brivaracetam) Prescribing Information, Schedule V. UCB, Inc.
Pregnancy registry: North American AED Pregnancy Registry. epilepsyregistry.org.
Patient resources: Epilepsy Foundation | American Epilepsy Society | UCB patient support: myuCARE
| Disclaimer: Health Evidence Digest provides general information about FDA approvals, loss of exclusivity events, and health research for educational purposes. This content is not a substitute for professional medical advice. Epilepsy management requires individualized assessment by a board-certified neurologist. Antiseizure medications should never be stopped or adjusted without medical supervision. Drug pricing information reflects figures at time of publication and is subject to change. |
|---|
Leave a Reply