| 📌 The essentials Trintellix (vortioxetine, Lundbeck/Takeda) is an oral antidepressant with a multimodal mechanism of action, approved in September 2013 for adults with major depressive disorder (MDD). It is not an SSRI. It simultaneously inhibits the serotonin transporter (SERT) and acts as an agonist, partial agonist, or antagonist at five distinct serotonin receptor subtypes: 5-HT1A (full agonist), 5-HT1B (partial agonist), 5-HT3 (antagonist), 5-HT7 (antagonist), and 5-HT1D (antagonist). The clinical differentiation: vortioxetine produces antidepressant and anxiolytic effects comparable to SSRIs and better-tolerated than SNRIs, while demonstrating a direct pharmacological benefit on cognitive function (processing speed, working memory) that duloxetine and SSRIs have not shown in controlled trials. The cognitive benefit is real and pharmacologically independent of mood improvement, but effect sizes are modest (standardized effect size 0.24 to 0.35 after MADRS adjustment). Current list price: approximately $514 per 30-day supply. Generic timeline: the core compound patent (U.S. Patent No. 7,144,884) expired June 17, 2026. A six-month pediatric exclusivity period extends effective market protection to approximately February 2027. As of June 2026, the FDA has not issued final generic approval for vortioxetine; three tentative approvals exist (Alembic, Lupin, and others), which convert to final approvals when exclusivity ends. Generic launches are expected in early to mid-2027 at prices 70 to 85% below current list price. |
|---|
| 📚 About this series: the 2026 Loss of Exclusivity Watch This is Post 8 of HED’s 2026 Loss of Exclusivity series, tracking the ten major drugs losing U.S. exclusivity this year. The full series covers: Xolair (omalizumab) • Pomalyst (pomalidomide) • Opsumit (macitentan) • Januvia/Janumet (sitagliptin) • Simponi (golimumab) • Mavenclad (cladribine) • Gattex (teduglutide) • Trintellix (vortioxetine) • Briviact (brivaracetam) • Xeljanz (tofacitinib). Each post follows the same format: what the drug is and how it works, what the clinical evidence shows, who uses it and why, and what the entrance of competition means for patients, prescribers, and the market. |
|---|
Major depressive disorder is the leading cause of disability worldwide. An estimated 280 million people live with depression globally, and in the United States alone, approximately 21 million adults experienced at least one major depressive episode in the past year. Despite decades of drug development, treatment outcomes remain deeply unsatisfying for a large proportion of patients. About one-third of people with MDD do not achieve adequate response after trying multiple antidepressants, a population so large and so poorly served that it has its own clinical designation: treatment-resistant depression.
Even among patients who do respond to antidepressants, a significant and underappreciated problem persists: cognitive impairment. Depression is not only a disease of mood. Patients consistently report difficulties with concentration, memory, processing speed, and executive function, symptoms that often persist even after mood has improved on conventional antidepressant therapy. This cognitive dysfunction in depression is one of the most significant contributors to functional impairment, disability, and reduced quality of life in patients who are otherwise considered treatment responders.
Vortioxetine is a novel antidepressant with multimodal activity that provides improvements in cognitive function alongside antidepressant and anxiolytic effects. In head-to-head comparisons it has been found to be one of the most tolerable options for MDD and demonstrates a direct cognitive benefit that comparators including duloxetine have not replicated in controlled trials.
Trintellix (vortioxetine), developed by Lundbeck and commercialized in the U.S. by Takeda, was FDA-approved in September 2013. The current list price is approximately $514 for a 30-day supply. A 2021 study of Medicare beneficiaries on antidepressants found 16.6% had cost-related medication nonadherence, and separate analyses have linked antidepressant nonadherence to more hospitalizations, more emergency room visits, and higher total medical costs, meaning high out-of-pocket costs can worsen the very condition these medications are meant to treat.
The core patent expired June 17, 2026. With pediatric exclusivity extending effective protection to approximately February 2027, generic vortioxetine is expected to reach U.S. pharmacies in early to mid-2027 at 70 to 85% below current list price.
What Major Depressive Disorder Is and Why It Remains So Hard to Treat
Major depressive disorder is diagnosed when a person experiences at least five of nine specific symptoms for two weeks or longer, with at least one of those symptoms being either depressed mood or loss of interest or pleasure. The other diagnostic criteria include changes in weight or appetite, sleep disturbances, psychomotor changes observable by others, fatigue, feelings of worthlessness or excessive guilt, difficulty thinking or concentrating, and recurrent thoughts of death or suicidal ideation.
What this clinical description obscures is the heterogeneity of the disease in practice. Two patients who both meet criteria for MDD may have almost entirely different symptom profiles: one with profound psychomotor slowing, hypersomnia, and appetite increase; another with insomnia, agitation, and severe cognitive dysfunction. The neurobiological mechanisms driving these different phenotypes are not identical, which helps explain why no single antidepressant works for all patients and why treatment often requires multiple trials.
The antidepressant treatment landscape has been dominated since the late 1980s by SSRIs, fluoxetine, sertraline, escitalopram, paroxetine, and subsequently by SNRIs such as venlafaxine and duloxetine. These drugs block the reuptake transporters for serotonin, and in the case of SNRIs, norepinephrine, increasing the available concentration of these neurotransmitters in the synaptic cleft. They are effective for many patients, reasonably well tolerated, and generically available at very low cost.
The unmet need they leave behind is twofold: the treatment-resistant patients who do not respond, and the responders who achieve better mood but not better thinking. Vortioxetine was specifically designed to address the second of these gaps, and the clinical evidence suggests it does so in a meaningful way.
The Science: What Makes Vortioxetine’s Mechanism Different
Most antidepressants approved over the past three decades have a single primary mechanism: blocking one or two neurotransmitter transporters. Vortioxetine does something fundamentally different. It simultaneously acts on multiple serotonin receptor subtypes while also blocking the serotonin transporter, creating what pharmacologists call a multimodal mechanism of action.
Vortioxetine is a 5-HT3, 5-HT7, and 5-HT1D receptor antagonist, a 5-HT1B receptor partial agonist, a 5-HT1A receptor full agonist, and an inhibitor of the serotonin transporter (SERT), leading to modulation of neurotransmission in several systems simultaneously. This multimodal activity is considered responsible for the antidepressant and anxiolytic effects and the improvement of cognitive function observed with vortioxetine.
SERT inhibition — blocking the serotonin reuptake transporter, just as SSRIs do — is the foundation. It increases serotonin availability in the synapse.
5-HT1A receptor full agonism activates receptors on serotonergic neurons in the raphe nuclei, increasing serotonin firing and release. SSRIs do not directly activate 5-HT1A; they increase serotonin, which then stimulates 5-HT1A indirectly. Vortioxetine’s direct agonism augments this effect.
5-HT3 receptor antagonism is arguably the most pharmacologically interesting element. 5-HT3 receptors are ion channels located on inhibitory interneurons throughout the brain. When activated, they inhibit the release of multiple neurotransmitters including serotonin, dopamine, norepinephrine, and acetylcholine. Blocking 5-HT3 removes this inhibitory brake on multiple neurotransmitter systems simultaneously, which may explain the pro-cognitive effects of vortioxetine.
5-HT7 receptor antagonism regulates circadian rhythms, sleep architecture, and learning and memory processes. Blocking these receptors enhances serotonin release and affects glutamatergic neurotransmission in the hippocampus, a region critical for memory consolidation.
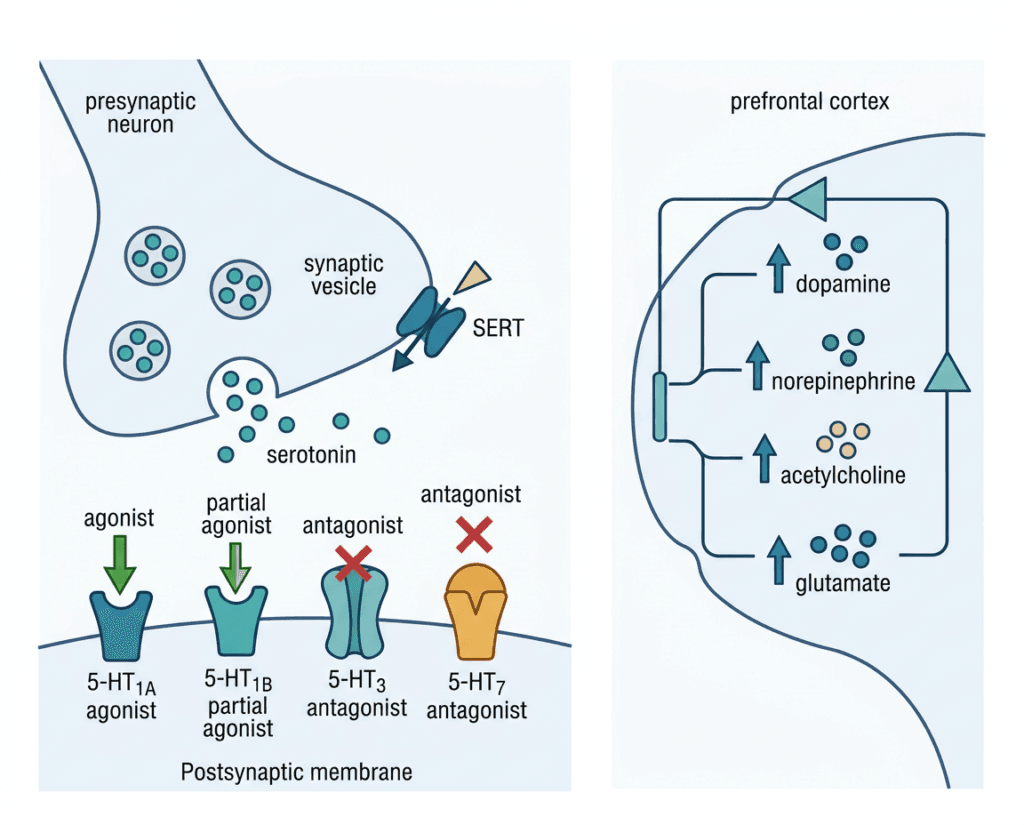
The downstream consequence of this receptor profile is that vortioxetine increases not only serotonin but also dopamine, norepinephrine, acetylcholine, histamine, and glutamate in specific brain regions. Enhanced release of glutamate from increased pyramidal neuron activity could enhance long-term potentiation, neuronal plasticity, and memory formation. This is not theoretical: the cognitive benefit is measured and quantified in clinical trials with objective neuropsychological instruments.
| Receptor target | Vortioxetine action | Downstream effect |
|---|---|---|
| SERT (serotonin transporter) | Inhibitor | Increases synaptic serotonin: the SSRI foundation |
| 5-HT1A receptor | Full agonist | Increases serotonin firing from raphe nuclei; anxiolytic effects |
| 5-HT1B receptor | Partial agonist | Further increases serotonin, glutamate, acetylcholine, histamine release |
| 5-HT3 receptor | Antagonist | Removes inhibitory brake on multiple neurotransmitters; key pro-cognitive contribution |
| 5-HT7 receptor | Antagonist | Affects circadian regulation, hippocampal glutamate, memory processes |
| 5-HT1D receptor | Antagonist | Modulates serotonin autoreceptors; contributes to net serotonin increase |
The Clinical Evidence: Mood, Cognition, and What the Head-to-Head Data Shows
Antidepressant efficacy
Across the pivotal clinical trials, vortioxetine consistently outperformed placebo on the Montgomery-Asberg Depression Rating Scale (MADRS), the primary outcome measure for MDD trials. A systematic review and meta-analysis of 20 studies involving 8,547 participants found that vortioxetine outperformed placebo in response (RR 1.35; 95% CI 1.23 to 1.48; p less than 0.001), remission (RR 1.33; 95% CI 1.17 to 1.52; p less than 0.001), and cognitive function (SMD 0.34; 95% CI 0.16 to 0.52; p less than 0.001).
Head-to-head comparisons with SSRIs and SNRIs require honest framing. Compared with SNRIs, vortioxetine had better tolerability (RR 0.90; 95% CI 0.86 to 0.94; p less than 0.001) but no significant difference in response or remission rates. Compared with SSRIs, vortioxetine showed no difference in response or remission. Vortioxetine is not more effective at treating depression symptoms than SSRIs or SNRIs. It is comparably effective and better tolerated than SNRIs. The clinical differentiation lies in what it does to cognition, not in superior mood outcomes.
The cognitive benefit: what the evidence actually shows
The cognitive evidence for vortioxetine is the most scientifically distinctive part of the drug’s story. The primary instrument used across trials to measure cognitive function was the Digit Symbol Substitution Test (DSST), a validated, objective neuropsychological test of processing speed, attention, and working memory.
A meta-analysis across three randomized, double-blind, placebo-controlled 8-week trials of vortioxetine in MDD found that before adjustment for MADRS score, vortioxetine separated from placebo on DSST in all individual trials and statistically improved DSST performance versus placebo in meta-analysis (standardized effect size [SES] 0.35; p less than 0.0001). After adjustment for MADRS score, controlling for the possibility that cognitive improvement was simply a consequence of mood improvement, vortioxetine maintained DSST improvement with separation from placebo maintained in meta-analysis (SES 0.24; p less than 0.0001). By contrast, duloxetine failed to separate from placebo on DSST in either individual trials or meta-analyses. Vortioxetine statistically favored duloxetine on DSST after MADRS adjustment.
The MADRS adjustment is the critical methodological point. A drug that improves mood will often improve cognition as a secondary consequence: patients think more clearly when they feel less depressed. By controlling statistically for the degree of mood improvement and still finding a cognitive benefit, the analysis establishes that vortioxetine’s cognitive effect has a direct pharmacological component beyond its antidepressant effect. Duloxetine, a widely used SNRI, did not demonstrate this.
A separate meta-analysis of six placebo-controlled trials confirmed that vortioxetine significantly improved cognitive function compared with placebo as measured by both DSST and PDQ (Perceived Deficit Questionnaire, a patient-reported cognitive outcomes measure) scores, with improvements not related to vortioxetine dosage.
| Outcome measure | Effect versus placebo | Effect versus duloxetine | Independence from mood improvement |
|---|---|---|---|
| MADRS (depression severity) | Significant (p less than 0.001) | Comparable | Not applicable |
| DSST (objective cognitive processing) | Significant (SES 0.35; p less than 0.0001) | Statistically superior (SES 0.16 favoring vortioxetine; p=0.04) | Maintained after MADRS adjustment (SES 0.24) |
| PDQ (patient-reported cognition) | Significant improvement | Better than SNRIs | Direct pharmacological component established |
| Response rate | RR 1.35 versus placebo | Comparable to SSRIs/SNRIs | — |
| Remission rate | RR 1.33 versus placebo | Comparable to SSRIs/SNRIs | — |
The honest framing: the cognitive benefit is real, statistically robust, and pharmacologically independent. But effect sizes are modest (SES 0.24 to 0.35 after adjustment). This is not a dramatic cognitive rescue. It is a meaningful but incremental advantage in processing speed and working memory that may translate to real functional improvement for patients who find cognitive symptoms particularly impairing.
Where Vortioxetine Fits in the 2026 Antidepressant Landscape
The MDD treatment landscape in 2026 is broader than it has ever been, and vortioxetine’s niche is more specific than its general antidepressant label implies.
The first-line standard of care remains SSRIs, sertraline, escitalopram, fluoxetine, all generically available for under $20 per month. They work for a large proportion of patients and their cost-effectiveness at scale is excellent. SNRIs including venlafaxine and duloxetine are also generically available and appropriate for patients who need norepinephrine augmentation or have comorbid pain conditions.
Vortioxetine’s specific clinical home is patients for whom cognitive symptoms are a prominent part of their depression, either the primary complaint or a residual symptom that persists after adequate mood response on prior treatment. The evidence supports a direct pharmacological role in improving objective processing speed and subjective cognitive function that other antidepressants including duloxetine have not demonstrated. This is where a prescriber would reach for vortioxetine rather than a less expensive SSRI alternative.
The 2026 antidepressant landscape also includes newer entrants in adjacent spaces. Esketamine (Spravato), approved for treatment-resistant depression, targets the glutamate system through NMDA receptor antagonism. Auvelity (dextromethorphan/bupropion), approved for MDD and now also for Alzheimer’s agitation, also targets NMDA receptors. Gepirone (Exxua), an azapirone approved in 2023, is a selective 5-HT1A agonist. None overlap directly with vortioxetine’s specific receptor profile, and none are positioned for the cognition-focused use case in the same way.
The comparison that matters most for payers and formulary decision-makers is vortioxetine against the cheap SSRIs. Once generic vortioxetine is available, priced at 70 to 85% below the current list price, the formulary calculus changes and patients who have been prescribed Trintellix at $500 per month can access the same molecule for $30 to $50.
The Patent Timeline: When Generics Will Actually Arrive
The core compound patent, U.S. Patent No. 7,144,884, expired June 17, 2026. A six-month pediatric exclusivity period follows, extending to approximately December 17, 2026. However, accounting for the specific pediatric study completion timing and the precise triggering conditions for exclusivity, the effective protection extends to approximately February 2027, which is the date used by most legal and pharmaceutical analysts as the practical entry window.
While Trintellix’s Orange Book patent listings extend as far as March 2032, federal courts have ruled that the latest-expiring patents do not cover the use generic manufacturers are seeking approval for, which is treating MDD rather than the specialized cognitive impairment or adverse-event management methods those later patents claimed. The patents stretching to 2031 and 2032 do not block generic vortioxetine tablets approved for MDD. The only enforceable barrier to generic entry is the core compound patent and the pediatric exclusivity.
As of June 2026, the FDA has not issued final approval for a generic version of Trintellix, though three tentative approvals exist. Tentative approval means the FDA has determined the applications are approvable but cannot grant final approval while exclusivity protections remain active. When pediatric exclusivity expires in approximately February 2027, those tentative approvals convert to final approvals and manufacturers can launch.
Manufacturers with tentative approvals include Alembic, Lupin, Macleods, Sandoz, Sigmapharm, and Zydus, each of which filed ANDAs and participated in the patent proceedings. First-to-file status in Hatch-Waxman litigation may entitle one or more challengers to 180 days of market exclusivity, meaning for six months after the first generic launch only the first filer can sell generic vortioxetine. After that window, the full field enters and prices typically fall sharply.
Patients and prescribers should expect generic vortioxetine availability in U.S. pharmacies beginning in early to mid-2027, with prices expected to fall 70 to 85% below Trintellix’s current list price within 12 to 18 months of multi-generic competition.
The Safety Profile
Vortioxetine’s tolerability profile is one of its clinical selling points. It avoids several side effects common to other antidepressant classes, while introducing its own characteristic profile.
| Safety item | Details | Clinical guidance |
|---|---|---|
| Nausea | Most common adverse event; reported in approximately 21 to 32% of patients across trials, dose-dependent, most prominent in the first 1 to 2 weeks. | Taking with food reduces severity. Starting at 5 mg and titrating to target dose may improve tolerability. Usually resolves within 2 weeks of continued treatment. |
| Sexual dysfunction | Less common than with SSRIs, a clinically meaningful advantage for many patients. However, decreased libido, delayed orgasm, and erectile dysfunction have been reported. | Discuss openly before initiating. The comparative advantage over SSRIs in this domain is meaningful for patients who have discontinued prior antidepressants due to sexual side effects. |
| Suicidality (boxed warning) | Class-level FDA boxed warning for all antidepressants: increased risk of suicidal thinking and behavior in children, adolescents, and young adults in short-term studies. Not indicated in pediatric patients. | Monitor closely during the first weeks of treatment, particularly in patients aged 18 to 24. Clinical benefit in adults 25 and older outweighs risk. |
| Serotonin syndrome | Risk when combined with other serotonergic drugs: other antidepressants, tramadol, certain migraine medications, linezolid. | Do not use with MAOIs or within 21 days of stopping an MAOI. Allow 14 days after stopping vortioxetine before starting an MAOI. Educate patients about serotonin syndrome symptoms. |
| Discontinuation syndrome | Abrupt discontinuation can cause dizziness, sensory disturbances, irritability, anxiety, and confusion. | Taper gradually when discontinuing; titrate down over 2 to 4 weeks. Never stop abruptly. |
| Hyponatremia | Low sodium, primarily in older adults on diuretics: a class effect of SSRIs and SNRIs also seen with vortioxetine. | Monitor sodium levels in at-risk patients, especially elderly patients on diuretics. |
| Abnormal bleeding | Increased risk of GI bleeding, particularly when combined with NSAIDs, aspirin, or anticoagulants, from serotonin’s role in platelet function. | Caution with concurrent anticoagulant or antiplatelet use. |
| Weight | Weight-neutral in clinical trials. A meaningful advantage compared to TCAs, mirtazapine, and some atypical antipsychotics used as augmentation agents. | Reassure patients who have experienced weight gain on prior antidepressant therapy. |
| Sleep | Vortioxetine does not significantly impair sleep architecture and may be beneficial for certain sleep disturbances associated with depression, a consequence of its 5-HT7 antagonism and circadian effects. | Can generally be taken at any time of day; morning dosing may be preferred to minimize any activating effects. |
The comparative tolerability data from meta-analyses is clinically important: vortioxetine showed better tolerability than SNRIs, with fewer discontinuations due to adverse events, while showing comparable tolerability to SSRIs. For patients who have discontinued duloxetine or venlafaxine due to side effects, including nausea, sweating, blood pressure elevation, or discontinuation symptoms, vortioxetine offers a mechanistically different profile worth considering.
What the Generic Arrival Means for Patients
The significance of generic vortioxetine for the MDD patient population is both economic and clinical. At $466 to $576 per month, Trintellix is out of reach as a sustainable long-term therapy for uninsured patients and represents a substantial burden for those with high-deductible insurance plans. Cost-related medication nonadherence in antidepressants has been directly linked to worse clinical outcomes including more hospitalizations and higher total healthcare costs.
Depression is not a disease where medication gaps are clinically neutral. Stopping an antidepressant prematurely is associated with relapse risk, and the period immediately following discontinuation carries elevated suicide risk in some patients. A drug that is too expensive to continue consistently is not just an economic problem. It is a clinical hazard.
When generic vortioxetine becomes available in early to mid-2027, the cost profile shifts dramatically. Patients currently maintained on Trintellix who have been managing significant cost-sharing will have access to the same molecule at a price comparable to other generic antidepressants. Prescribers who have been reluctant to start Trintellix due to prior authorization requirements and formulary friction will face a different landscape. And patients who have heard about the cognitive benefits but could not access the drug financially will have a realistic path to trying it.
For patients currently on Trintellix who are responding: nothing changes clinically in 2026. The drug is available, and payer formularies have not yet shifted to generic alternatives because none exist. In early to mid-2027, when your formulary sends a notification about transitioning to generic vortioxetine, the medication will be therapeutically identical to what you are taking today. The active ingredient, the dose, the mechanism, and the clinical effects are the same. A brief conversation with your prescriber at your next visit is appropriate, not a reason to delay transition.
If you are experiencing a mental health crisis, contact the 988 Suicide and Crisis Lifeline by calling or texting 988.
For related HED coverage on newer antidepressant and psychiatric drug approvals in 2026, see our post on Auvelity receiving its second FDA approval for agitation in Alzheimer’s disease and our coverage of the FDA’s psychedelic drug program accelerations, including psilocybin for treatment-resistant depression.
Sources
Trintellix FDA approval: FDA approves vortioxetine to treat major depressive disorder. FDA.gov. September 2013.
Patent expiry and litigation timeline: U.S. court issues decision in Trintellix patent litigation. Lundbeck press release. news.cision.com. October 1, 2021. | Trintellix Patent Expiration Date and Generic Timeline. LegalClarity. April 2026.
Federal Circuit non-infringement ruling: H. Lundbeck A/S v. Lupin Ltd, No. 22-1194 (Fed. Cir. 2023). A&O Shearman. January 2026.
Generic availability (current): Generic Trintellix Availability. drugs.com. Updated June 11, 2026.
Trintellix pricing: Trintellix (vortioxetine) prices. MedicalNewsToday. 2026.
Cost-related nonadherence in antidepressants: Reus VI et al. Cost-related medication nonadherence among Medicare beneficiaries with depression. JAMA Psychiatry. 2021. PMID 33739377.
Vortioxetine mechanism (StatPearls): Vortioxetine. StatPearls. NCBI.
Multimodal mechanism — receptor specifics: Stahl SM. Modes and nodes explain the mechanism of action of vortioxetine: blocking 5HT3 receptors enhances release of serotonin, norepinephrine, and acetylcholine. CNS Spectrums. 2015.
Cognitive effects meta-analysis (primary, PMC 2016): Vieta E et al. The Effects of Vortioxetine on Cognitive Function in Patients with MDD: A Meta-Analysis of Three Randomized Controlled Trials. PMC5091829.
Cognitive effects meta-analysis (2022): Li J et al. Effect of Vortioxetine on Cognitive Impairment in Patients with Major Depressive Disorder: A Systematic Review and Meta-analysis. Int J Neuropsychopharmacol. 2022;25(12):969. PMC9743961.
Efficacy versus SSRIs/SNRIs meta-analysis: Systematic Review and Meta-Analysis of Vortioxetine for MDD in Adults. PMC9263295.
Cognitive dysfunction in depression review: Cognitive dysfunction in MDD. PMC6416141.
Treatment-resistant depression: Treatment-Resistant Depression. StatPearls. NCBI.
MDD StatPearls: Major Depressive Disorder. StatPearls. NCBI.
SSRIs: Selective Serotonin Reuptake Inhibitors. StatPearls. NCBI.
SNRIs: Serotonin-Norepinephrine Reuptake Inhibitors. StatPearls. NCBI.
Serotonin syndrome: Serotonin Syndrome. StatPearls. NCBI.
Trintellix prescribing information: Trintellix (vortioxetine) Prescribing Information. Takeda Pharmaceuticals.
NIMH MDD statistics: Major Depression. NIMH.
WHO depression fact sheet: Depression. WHO.
Esketamine FDA approval: FDA approves esketamine nasal spray (Spravato) for treatment-resistant depression. FDA.gov.
988 Suicide and Crisis Lifeline: 988lifeline.org.
HED internal references: Auvelity Alzheimer’s agitation approval post | FDA psychedelic drug program post
Patient resources: National Alliance on Mental Illness (NAMI) | Mental Health America | 988 Suicide and Crisis Lifeline | SAMHSA National Helpline: 1-800-662-4357
| Disclaimer: Health Evidence Digest provides general information about FDA approvals, loss of exclusivity events, and health research for educational purposes. This content is not a substitute for professional medical advice. Depression is a serious medical condition requiring individualized diagnosis and treatment by a qualified clinician. Decisions about antidepressant therapy, including transitions between brand-name and generic medications, should be made in consultation with a prescribing psychiatrist, primary care physician, or other qualified mental health provider. Never discontinue an antidepressant without medical guidance. If you or someone you know is experiencing a mental health crisis, contact the 988 Suicide and Crisis Lifeline by calling or texting 988. |
|---|
Leave a Reply