| 📌 The essentials On June 9, 2026, the FDA approved a new maintenance dosing regimen for Ebglyss (lebrikizumab-lbkz, Eli Lilly): one injection of 250 mg every 8 weeks (Q8W) for adults and adolescents aged 12 years and older weighing at least 40 kg (approximately 88 lbs) with moderate-to-severe atopic dermatitis (AD) not adequately controlled with topical prescription therapies. This is a new dosing regimen approval, not a new drug or new indication. Ebglyss was originally approved in September 2024 for the same population with a once-every-4-weeks (Q4W) maintenance regimen. The complete dosing schedule with the Q8W option: induction with 500 mg (two 250 mg injections) at weeks 0 and 2, then 250 mg every 2 weeks through week 16 or until adequate clinical response is achieved, followed by maintenance dosing of either 250 mg Q4W or 250 mg Q8W. What makes the Q8W approval clinically notable: Ebglyss is now the only FDA-approved biologic for atopic dermatitis that offers as few as 6 maintenance injections per year without a mandatory requirement for concomitant topical therapy from treatment initiation. No other approved AD biologic currently combines both of these features. The evidence basis: longitudinal exposure-response modeling and the Q8W ADjoin extension (NCT04392154), a 32-week open-label study evaluating Q8W and Q4W dosing in patients who had completed the 100-week ADjoin long-term study. No new safety signals were identified. No patients discontinued due to adverse events through 32 weeks. Important interpretive caveat: extension participants had already received approximately 100 weeks of lebrikizumab therapy before entering the Q8W study. The real-world applicability to newly initiating patients who transition to Q8W earlier has not been directly studied. |
|---|
Atopic dermatitis is not a rash. It is a chronic, relapsing immune-mediated inflammatory disease of the skin that affects an estimated 16 million adults in the United States, more than 10% of the adult population, and a substantially higher proportion of children. At its severe end, atopic dermatitis produces relentless itch, disrupted sleep, cracked and weeping skin, and a psychological burden documented to rival conditions such as psoriasis and chronic pain. For adults and adolescents with moderate-to-severe disease inadequately controlled by topical therapies, systemic treatments including biologics are increasingly the standard of care.
Ebglyss (lebrikizumab), an IL-13 inhibitor, was approved in September 2024 with a once-monthly (Q4W) maintenance dosing schedule. On June 9, 2026, the FDA approved an expanded maintenance option: one injection every 8 weeks (Q8W), allowing eligible patients to reduce their annual injection burden from 13 to as few as 6 after completing induction. That numerical change from 13 to 6 injections per year is not a trivial reduction in the context of a disease that will require ongoing management for most patients indefinitely.
This post covers what atopic dermatitis is, how IL-13 drives its pathology and why blocking it works, what the ADjoin extension data supports, what the competitive significance of the Q8W approval is, and what patients and prescribers need to know about the dosing schedule in practice.
What Atopic Dermatitis Is and Why Moderate-to-Severe Disease Requires Systemic Therapy
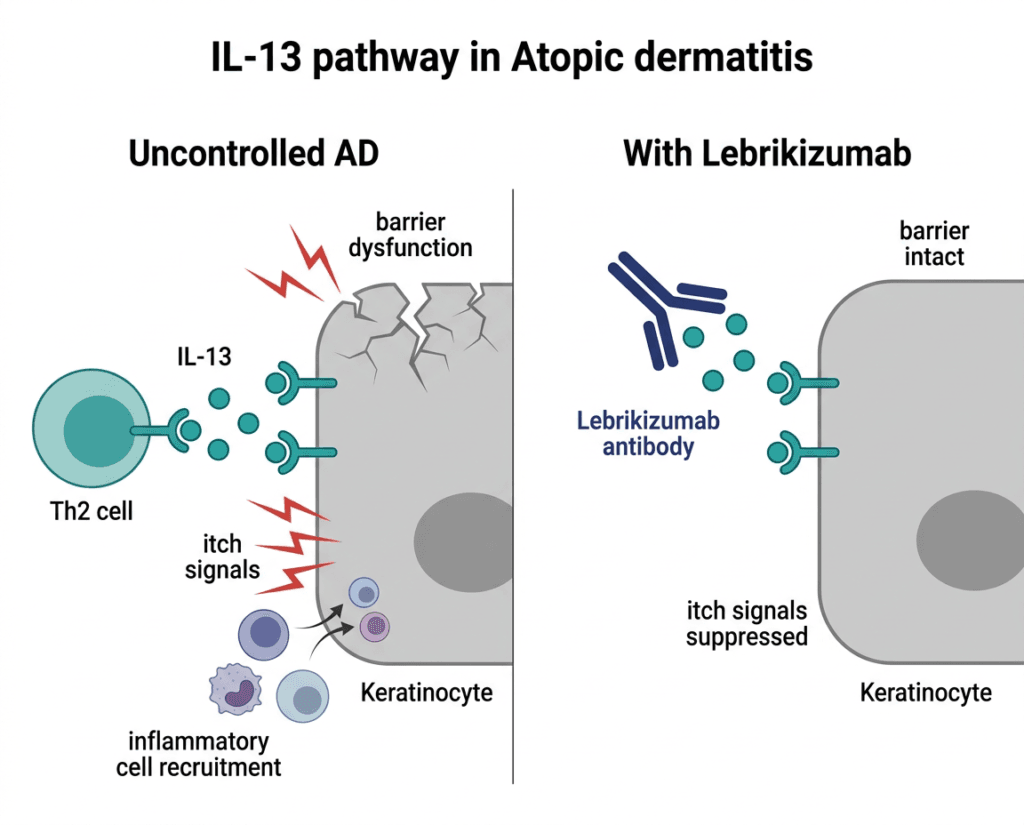
Atopic dermatitis is a chronic inflammatory skin disease driven by dysfunction in both the skin barrier and the immune system. The two abnormalities are interconnected: a defective epidermal barrier, often related to mutations in the gene encoding filaggrin, allows allergens, irritants, and microorganisms to penetrate the skin, triggering and sustaining a type 2 (Th2-skewed) immune response. The resulting cytokine cascade, dominated by IL-4, IL-13, and IL-31, drives ongoing skin inflammation, barrier disruption, and the hallmark symptom of atopic dermatitis: intense, persistent itch.
The Th2-skewed immune response in atopic dermatitis is what has made this disease amenable to targeted biologic therapy. The first approved biologic for AD, dupilumab (Dupixent), targets both IL-4 and IL-13 by blocking the shared IL-4 receptor alpha chain. Lebrikizumab takes a more targeted approach: it binds specifically and exclusively to IL-13.
Why moderate-to-severe atopic dermatitis requires more than topical therapy
Topical corticosteroids and calcineurin inhibitors (tacrolimus, pimecrolimus) are effective for mild to moderate disease but have significant limitations in moderate-to-severe disease. Long-term topical corticosteroid use carries risks of skin atrophy, striae, and hypothalamic-pituitary-adrenal axis suppression with extensive application. The emotional and logistical burden of applying topical agents to extensive, inflamed skin multiple times daily is substantial, particularly for patients with involvement of difficult-to-treat areas such as the face, neck, and skin folds.
For patients whose disease is not adequately controlled by topical prescription therapies, systemic options including biologics targeting IL-4/IL-13 signaling (dupilumab, tralokinumab, lebrikizumab) and the JAK inhibitor class (upadacitinib, abrocitinib, baricitinib) represent the current standard. No mandatory concomitant topical therapy requirement at treatment initiation is a practical advantage for patients with extensive or difficult-to-treat distribution.
The Science: How IL-13 Drives Atopic Dermatitis and Why Blocking It Works
Interleukin-13 (IL-13) is a cytokine produced primarily by activated Th2 T cells, innate lymphoid cells type 2 (ILC2), and mast cells in atopic skin. It is the dominant driver of multiple pathological processes in atopic dermatitis:
Skin barrier disruption: IL-13 suppresses the expression of filaggrin, loricrin, and other structural proteins essential for the epidermal barrier. By reducing barrier protein synthesis, IL-13 perpetuates the permeability defect that allows allergen penetration and drives the cycle of sensitization and immune activation.
Itch: IL-13 directly stimulates sensory nerve fibers and primes skin-resident cells to release histamine and other pruritogens, contributing directly to the intense itch that is the defining symptom of atopic dermatitis.
Inflammation: IL-13 activates keratinocytes, fibroblasts, and other skin cells to produce chemokines and adhesion molecules that recruit additional immune cells to the skin, amplifying the local inflammatory response.
IgE production: IL-13 cooperates with IL-4 to drive B cell class switching to IgE production, the antibody class responsible for atopic sensitization.
Lebrikizumab is a high-affinity human monoclonal antibody that binds specifically to IL-13 itself, rather than to the IL-4/IL-13 shared receptor that dupilumab targets. By capturing circulating IL-13 before it can engage its receptor, lebrikizumab blocks downstream signaling through both the IL-13Rα1/IL-4Rα heterodimer (the signaling receptor for IL-13 in skin cells) and the IL-13Rα2 decoy receptor. The high binding affinity and specificity for IL-13 means the drug does not affect IL-4 signaling, which distinguishes it from dupilumab pharmacologically, though clinical outcomes in pivotal trials have been broadly comparable in terms of efficacy endpoints.
The structural basis for lebrikizumab’s IL-13 binding has been characterized crystallographically: the antibody binds at a distinct epitope on IL-13 that prevents both IL-13Rα1 and IL-13Rα2 engagement, explaining the completeness of its IL-13 blockade.
The Approved Dosing Schedule: Complete and Correct
With the June 9, 2026 approval, the complete Ebglyss dosing schedule for the approved population (adults and adolescents aged 12 years and older, weight at least 40 kg) is:
| Phase | Dose | Frequency |
|---|---|---|
| Induction (weeks 0 and 2) | 500 mg (two 250 mg injections administered at the same visit) | Two doses, two weeks apart |
| Maintenance (weeks 2 through 16 or until adequate response) | 250 mg single injection | Every 2 weeks (Q2W) |
| Maintenance (after adequate response achieved, ongoing) | 250 mg single injection | Every 4 weeks (Q4W) OR every 8 weeks (Q8W) — patient and clinician choice |
The decision between Q4W and Q8W maintenance should be individualized. Patients with robust and sustained response who prefer a less frequent injection schedule are candidates for Q8W. Patients with a history of more frequent flares or less complete response may be better maintained on Q4W. This is a clinical judgment discussion between the patient and their dermatologist.
Annual injection count summary:
- Induction (2 visits, 4 injections total across weeks 0 and 2, plus Q2W phase)
- Q4W maintenance: approximately 13 injections per year
- Q8W maintenance: as few as 6 injections per year
The ADjoin Extension Data: What Supported the Q8W Approval
The Q8W approval was based on two complementary data sources: longitudinal exposure-response modeling and the Q8W ADjoin extension study.
Exposure-response modeling
The pharmacokinetic and pharmacodynamic data from the original lebrikizumab development program, including ADvocate 1 and ADvocate 2 (the pivotal Phase 3 trials), demonstrated that lebrikizumab’s long half-life and sustained IL-13 suppression at Q8W dosing supported the hypothesis that every-8-week dosing could maintain therapeutic drug levels and clinical response in patients who had achieved adequate disease control. Longitudinal exposure-response modeling provides the mechanistic rationale for the regimen; the ADjoin extension provided the confirmatory clinical data.
ADjoin extension (NCT04392154)
The Q8W ADjoin extension was a 32-week open-label study evaluating Q8W and Q4W dosing in adult and adolescent patients who had completed the 100-week ADjoin long-term study. ADjoin itself enrolled completers from four prior Phase 3 trials: ADvocate 1 and 2 (52-week trials), ADore (52-week trial), and ADopt-VA (16-week trial). Patients in the extension received open-label Ebglyss 250 mg, Q8W or Q4W, regardless of their prior dosing interval (Q2W or Q4W) or response status at extension baseline.
Extension safety findings:
- No new safety signals identified through 32 weeks of Q8W dosing
- No patients discontinued due to adverse events through 32 weeks
- Safety profile consistent with the established lebrikizumab dataset
Efficacy:
- Disease control was maintained through 32 weeks in both Q8W and Q4W dosing groups
- Long-term data from the broader lebrikizumab program show durable disease control for up to 4 years of continuous treatment
Dr. Peter Lio, MD, primary investigator of the ADjoin study and Clinical Assistant Professor of Dermatology and Pediatrics at Northwestern University, noted that extending maintenance dosing to every eight weeks represents an important option for patients living with moderate-to-severe atopic dermatitis.
The important interpretive caveat
The patients in the Q8W ADjoin extension had already completed approximately 100 weeks of lebrikizumab therapy before entering the extension. They were therefore a population with demonstrated long-term tolerability and sustained response, representing a selected, treatment-experienced group. The real-world applicability of Q8W dosing in newly initiating patients who have completed induction and transitioned earlier to Q8W maintenance has not been directly studied in a de novo population. Dermatologists should discuss this with patients: the 6-injections-per-year figure applies to patients who have achieved and maintained adequate response; the long-term profile of Q8W in newly initiated patients should be monitored as real-world experience accumulates.
Competitive Context: Where This Places Ebglyss in the AD Biologic Landscape
The atopic dermatitis biologic market in 2026 is the most competitive it has ever been. The approved biologics for moderate-to-severe AD include:
| Drug | Target | Approval | Dosing (maintenance) | Mandatory topical |
|---|---|---|---|---|
| Dupixent (dupilumab, Sanofi/Regeneron) | IL-4Rα (blocks IL-4 and IL-13) | 2017 (adults); expanded | Q2W | No |
| Adbry (tralokinumab, LEO Pharma) | IL-13 | 2021 | Q2W; Q4W option available | No |
| Ebglyss (lebrikizumab, Lilly) | IL-13 | 2024 | Q4W or Q8W | No |
The Q8W approval gives Ebglyss a dosing frequency advantage over dupilumab (Q2W mandatory maintenance) and tralokinumab (Q2W standard, Q4W available for responders). Ebglyss’s Q8W maintenance option of as few as 6 injections per year, without a mandatory concomitant topical therapy requirement, is a combination not currently available with any other approved AD biologic. That distinction is commercially meaningful for Lilly and clinically meaningful for the subset of patients who are well-controlled responders and for whom injection burden influences long-term adherence.
The practical comparison for prescribers: dupilumab has the most extensive long-term evidence base and the broadest approved indication range (including asthma, eosinophilic esophagitis, chronic rhinosinusitis with nasal polyps, and prurigo nodularis in addition to AD). For patients whose primary driver is AD management and for whom injection frequency is a concern, Ebglyss’s Q8W option is now a differentiating factor worth discussing.
Safety: What Prescribers and Patients Need to Know
The safety profile of lebrikizumab with the Q8W dosing regimen is consistent with the established dataset from the full lebrikizumab clinical program. The most common adverse reactions (occurring in at least 1% of patients) are:
Conjunctivitis: The most characteristic class effect across all IL-4/IL-13 pathway targeting biologics. Conjunctivitis in the lebrikizumab trials occurs at lower rates than typically reported with dupilumab, which is a clinically relevant distinction for patients who have experienced significant eye symptoms on dupilumab. Mild to moderate conjunctivitis should be assessed and treated with ophthalmic supportive care; if severe or persistent, ophthalmology consultation and discussion of dose adjustment are appropriate.
Injection site reactions: Common, typically mild (redness, pain, swelling at the injection site), and generally not requiring discontinuation. Rotate injection sites; abdomen, thigh, and upper arm are acceptable locations.
Herpes zoster: IL-13 pathway inhibition has a low but documented association with herpes zoster (shingles) reactivation. Patients who have not been vaccinated against herpes zoster should discuss vaccination with their dermatologist before initiating long-term biologic therapy for atopic dermatitis.
Contraindications:
- Hypersensitivity to lebrikizumab-lbkz or any ingredient in Ebglyss
Live vaccines: As with all biologic therapies, live attenuated vaccines should not be administered during lebrikizumab treatment. Update all vaccines, including zoster vaccine, before initiating therapy.
Pregnancy: The effect of lebrikizumab on a developing fetus is not fully established. Discuss contraception and pregnancy planning with patients of reproductive potential. A pregnancy exposure registry (1-800-545-6962) is available for patients who become pregnant while on Ebglyss.
What This Means for Patients
For patients currently on Ebglyss Q4W who are achieving good disease control, the Q8W option is now available to discuss with their dermatologist. If you have been well-controlled for an extended period on Q4W maintenance and would benefit from a less frequent injection schedule, this is a conversation worth initiating at your next dermatology appointment.
For patients newly initiating Ebglyss: the standard induction and Q2W maintenance schedule remains the starting point. The Q8W option comes after achieving adequate clinical response, which typically occurs by week 16. The dosing path is: start with induction, achieve response, then discuss with your dermatologist whether Q4W or Q8W maintenance fits your response profile and lifestyle.
For patients who have experienced significant conjunctivitis on dupilumab: lebrikizumab’s IL-13-only mechanism (not blocking IL-4) is associated with lower conjunctivitis rates than dupilumab in clinical trials, making it a clinically reasonable alternative for patients where ocular side effects have been a management challenge.
For prescribers: the Q8W approval gives an additional tool for the conversation about long-term maintenance. Patient adherence to any chronic biologic therapy is improved by dosing schedules that fit into normal life rhythms. Six injections per year, administered at home without routine monitoring requirements, is a significantly lighter burden than monthly or biweekly regimens for patients who can achieve and sustain adequate disease control.
For related HED coverage on biologics for inflammatory conditions and the expanding IL-13 inhibitor class, see our post on Fasenra (benralizumab) receiving its new indication for hypereosinophilic syndrome and our post on Xolair (omalizumab) and its biosimilar transition as part of the 2026 LOE series, which covers the broader IgE/type-2 inflammation treatment landscape in which both drug classes operate.
Sources
Lilly FDA approval press release: FDA approves Lilly’s EBGLYSS (lebrikizumab-lbkz) for one maintenance dose every eight weeks. Eli Lilly. investor.lilly.com. June 9, 2026.
Drugs.com approval news: FDA Approves Lilly’s Ebglyss for One Maintenance Dose Every Eight Weeks. drugs.com. June 9, 2026.
HCPLive clinical coverage: FDA Approves Lebrikizumab 8-Week Maintenance Dosing in Atopic Dermatitis. hcplive.com. June 2026.
BioPharm International clinical coverage: FDA Approves Lebrikizumab Every-8-Week Maintenance Dosing for Moderate-Severe Atopic Dermatitis. biopharminternational.com. June 2026.
Contemporary Pediatrics (with investigator caveat): FDA approves lebrikizumab every-8-week maintenance dosing for moderate-to-severe atopic dermatitis. contemporarypediatrics.com. June 2026.
Dermatology Times coverage: Lebrikizumab Earns FDA Approval for Less Frequent, Every-8-Week Maintenance Dosing in AD. dermatologytimes.com. June 2026.
ADjoin extension (NCT04392154): NCT04392154. ClinicalTrials.gov.
Silverberg J et al. (ADjoin Q8W data; Fall Clinical Dermatology Conference 2025): Silverberg J, et al. Lebrikizumab every 8 weeks as maintenance dose provides long-lasting response in patients with moderate-to-severe atopic dermatitis. Fall Clinical Dermatology Conference. 2025.
4-year durability data (Almirall): Lebrikizumab delivered long-term disease control for up to four years in patients with moderate-to-severe atopic dermatitis. Almirall press release. March 27, 2026.
Ebglyss original FDA approval (September 2024): FDA approves lebrikizumab-lbkz for atopic dermatitis. FDA.gov.
Dupixent FDA approval: FDA approves dupilumab for moderate to severe atopic dermatitis. FDA.gov.
Adbry FDA approval: FDA approves tralokinumab-ldrm for atopic dermatitis. FDA.gov.
IL-13 in atopic dermatitis: IL-13 in Atopic Dermatitis. PMC8908499.
Lebrikizumab IL-13 binding mechanism: Okragly A et al. Binding, neutralization and internalization of IL-13 antibody lebrikizumab. Dermatology and Therapy. 2023. doi:10.1007/s13555-023-00947-7.
Lebrikizumab structural basis: Ultsch M et al. Structural basis of signaling blockade by IL-13 antibody lebrikizumab. Journal of Molecular Biology. 2013;425(8):1330-1339. doi:10.1016/j.jmb.2013.01.024.
Atopic dermatitis epidemiology: Atopic Dermatitis. StatPearls. NCBI.
Atopic dermatitis quality of life burden: AD Quality of Life and Burden. PMC7305275.
NIAMS atopic dermatitis overview: Atopic Dermatitis. NIAMS.
Ebglyss prescribing information: EBGLYSS (lebrikizumab-lbkz) Prescribing Information. Eli Lilly. 2026.
Patient resources: National Eczema Association | American Academy of Dermatology: Find a Dermatologist | Lilly Ebglyss patient support
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice. Decisions about biologic therapy for atopic dermatitis, including the choice between Q4W and Q8W maintenance dosing for Ebglyss, should be made in close consultation with a board-certified dermatologist or allergist familiar with the patient’s disease history, prior treatment response, and overall health profile. |
|---|
Leave a Reply