| 📌 The essentials Mavenclad (cladribine tablets, EMD Serono) is the first and only FDA-approved MS treatment that provides two years of proven disease control with a maximum of 20 days of oral tablet-taking across the entire two-year treatment cycle. Approved in March 2019 for relapsing-remitting MS (RRMS) and active secondary progressive MS (SPMS) in patients with inadequate response to or intolerance of an alternate MS therapy. Mechanism: selective immune reconstitution therapy (SIRT). Cladribine is a synthetic purine nucleoside analogue that preferentially depletes B cells and T cells, particularly memory B cells, while largely sparing innate immune cells. This produces durable disease control without continuous immunosuppression. Revenue: Mavenclad generated sales of approximately €1.2 billion in 2025, with North American revenue of €635 million. The patent story: an appeals court upheld a decision by the U.S. Patent Office invalidating two of the dosing regimen patents protecting Mavenclad. Generic launches arrived in December 2025, roughly 10 to 11 months earlier than Merck KGaA anticipated. Merck guided for no U.S. Mavenclad sales from March 2026 onward amid generic competition. Generic pricing: approximately $15,000 to $22,000 per annual treatment course versus brand-name list price of approximately $99,500. CLARITY trial primary endpoint: 57.6% reduction in annualized relapse rate with cladribine 3.5 mg/kg versus placebo (0.14 vs. 0.33; p less than 0.001) at 96 weeks. CLARITY Extension: clinical benefits from the two-year treatment course may be maintained for at least four years in the majority of patients. Boxed warning: embryo-fetal toxicity. Contraception required during treatment and for 6 months after the last dose in both male and female patients. |
|---|
| 📚 About this series: the 2026 Loss of Exclusivity Watch This is Post 6 of HED’s 2026 Loss of Exclusivity series, tracking the ten major drugs losing U.S. exclusivity this year. The full series covers: Xolair (omalizumab) • Pomalyst (pomalidomide) • Opsumit (macitentan) • Januvia/Janumet (sitagliptin) • Simponi (golimumab) • Mavenclad (cladribine) • Gattex (teduglutide) • Trintellix (vortioxetine) • Briviact (brivaracetam) • Xeljanz (tofacitinib). Each post follows the same format: what the drug is and how it works, what the clinical evidence shows, who uses it and why, and what the entrance of competition means for patients, prescribers, and the market. |
|---|
Multiple sclerosis is the most common acquired neurological disease of young adults, affecting roughly one million people in the United States and 2.9 million worldwide. It is a disease that primarily strikes in the prime of life, with most patients receiving their diagnosis between the ages of 20 and 40, and the prospect of decades of progressive disability shapes every treatment decision from the moment of diagnosis.
Most MS therapies require continuous, ongoing treatment. You take the pill daily, or inject yourself weekly, or receive an infusion every month or every six months, indefinitely. The therapy suppresses disease activity while you are taking it; stop taking it, and the disease typically returns.
Mavenclad (cladribine tablets) is the first and only FDA-approved treatment for relapsing-remitting MS and active secondary progressive MS that provides two years of proven efficacy with a maximum of 20 days of oral treatment over a two-year period. Patients take cladribine tablets for a handful of days during two treatment weeks in Year 1, and the same in Year 2, a total of no more than 20 days of actual tablet-taking across the entire two-year treatment cycle. Then, for many patients, no further treatment is needed for at least the following two years.
That is genuinely unlike anything else in the MS formulary. And it is possible because of the biology of what cladribine does inside lymphocytes, a mechanism that produces durable disease control not through continuous immunosuppression, but through something closer to an immune system reset.
Mavenclad generated sales of approximately €1.2 billion in 2025, with North American revenue of €635 million. Then came a dramatic turn. An appeals court upheld a decision by the U.S. Patent Office invalidating two of the dosing regimen patents that had been protecting Mavenclad from generic competition. Generic launches arrived in December 2025, roughly 10 to 11 months earlier than Merck KGaA had anticipated, and Merck’s guidance for 2026 assumed no U.S. Mavenclad sales from March onward amid generic competition.
This post covers the science behind cladribine’s mechanism, what the pivotal CLARITY trials showed, where it fits in the MS treatment landscape, and what the patent invalidation and early generic entry mean for patients and prescribers.
What Multiple Sclerosis Is and Why Relapsing Forms Are the Target
MS is a chronic autoimmune disease in which the immune system attacks myelin, the protective sheath surrounding nerve fibers in the brain and spinal cord, and over time the nerve fibers themselves. The resulting nerve damage disrupts signals between the brain and body, producing a wide spectrum of symptoms: fatigue, walking difficulty, cognitive problems, vision loss, sensory disturbances, spasticity, bladder dysfunction, and pain.
Relapsing-remitting MS (RRMS) is the most common form at diagnosis, affecting approximately 85% of newly diagnosed patients. It is characterized by discrete episodes of neurological worsening (relapses or attacks) followed by periods of partial or complete recovery. Inflammation is the dominant driver of damage in the relapsing phase.
Active secondary progressive MS (SPMS) develops in a proportion of RRMS patients over time, transitioning from a relapsing pattern to steady, ongoing accumulation of disability with or without superimposed relapses. The FDA approved cladribine specifically for SPMS patients who still have active inflammatory disease, a distinction that matters because not all SPMS patients benefit from anti-inflammatory therapies.
Primary progressive MS (PPMS) involves steady neurological decline from onset, without relapses, and is a distinct biological entity. Cladribine is not indicated for PPMS.
Cladribine’s mechanism, selectively depleting the lymphocytes that drive MS inflammation, is most relevant in the relapsing disease context, where adaptive immune cells (B cells and T cells) are the primary drivers of the inflammatory cascade responsible for relapses and new MRI lesion formation.
The Science: What Cladribine Does and Why 20 Days Generates Years of Effect
Cladribine is a synthetic purine nucleoside analogue, a molecular mimic of deoxyadenosine, one of the building blocks of DNA. Understanding why it works in MS requires understanding why lymphocytes are unusually vulnerable to it.
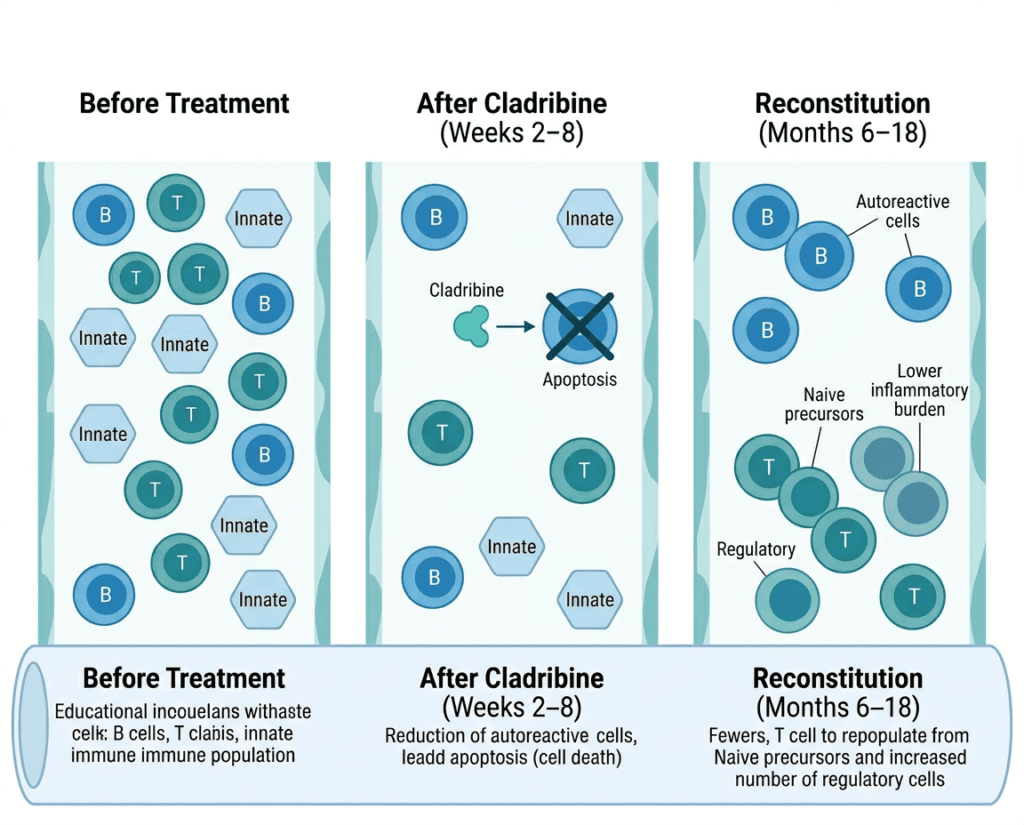
The main mechanism of action is the induction of a cytotoxic effect on lymphocytes, leading to long-term depletion of peripheral T and B cells. To produce its effects, cladribine must be phosphorylated inside the cell by deoxycytidine kinase (DCK) to its active triphosphate form. Here is the key to cladribine’s selectivity: DCK is expressed at high levels in lymphocytes, far higher than in most other cell types. When cladribine enters a lymphocyte, DCK phosphorylates it into the active form, which then accumulates intracellularly, impairs DNA synthesis and repair, and triggers apoptosis (programmed cell death). Cells that express low levels of DCK, including most cells of the innate immune system such as neutrophils and monocytes, cannot efficiently activate cladribine and are therefore largely spared.
This biochemical selectivity produces a clinically important profile: cladribine preferentially depletes lymphocytes without a major impact on innate immune cells. Within the lymphocyte compartment, it depletes B cells more profoundly and durably than T cells.
Memory B cells, the long-lived immune cells that carry immune memory and drive antigen-specific inflammation, repopulate very slowly after depletion. Unlike immature and mature B cell populations, memory B cells repopulate mostly via germinal center activity, leading to selective long-term loss of peripheral blood memory B cells that may persist for 18 months or longer. In a real-world longitudinal study, after two months CD19 B-lymphocytes were reduced by approximately 85%, CD4 T-lymphocytes by approximately 50%, and CD8 T-lymphocytes by approximately 40% of baseline levels. After 12 months, CD19 B-lymphocytes had largely reconstituted, while CD4 and CD8 T-lymphocytes remained depleted at approximately 40% and 30% of baseline levels respectively.
| Lymphocyte population | Depletion at Month 2 | Reconstitution at Month 12 | Key clinical relevance |
|---|---|---|---|
| CD19+ B cells (total) | approximately 85% reduction | Largely reconstituted | Deep early depletion of cells implicated in MS pathogenesis |
| Memory B cells specifically | Marked depletion (comparable to alemtuzumab) | Very slow; may remain depleted 18 months or longer | Prolonged memory B cell depletion may underlie durable efficacy |
| CD4+ T cells | approximately 50% reduction | Remain approximately 40% depleted at 12 months | Slower recovery; contribute to ongoing disease suppression |
| CD8+ T cells | approximately 40% reduction | Remain approximately 30% depleted at 12 months | Less selectively depleted than B cells |
| Innate immune cells (neutrophils, monocytes) | Largely spared | Not applicable | Preserves first-line infection defense |
This pattern, deep early depletion of pathogenic lymphocytes followed by gradual immune reconstitution, is the basis for cladribine’s classification as a selective immune reconstitution therapy (SIRT). As a SIRT, cladribine acts as a short-term immunosuppressant rather than a long-term maintenance immunosuppressive. The hypothesis is that depleting autoreactive lymphocytes and allowing the immune system to reconstitute from a cleaner baseline creates a durable window of reduced inflammatory disease activity, without requiring continuous immunosuppressive therapy.
The CLARITY Trials: What the Clinical Evidence Shows
The pivotal clinical program supporting Mavenclad’s approval was the CLARITY trial and its extension, together comprising the most comprehensive dataset for oral cladribine in MS.
CLARITY was a Phase 3, multicenter, randomized, double-blind, placebo-controlled trial enrolling 1,326 patients with RRMS. Patients were randomized to cladribine tablets at cumulative doses of 3.5 mg/kg or 5.25 mg/kg body weight, or placebo, administered as short-course annual treatment over 96 weeks.
| Outcome at 96 weeks | Placebo | Cladribine 3.5 mg/kg | Cladribine 5.25 mg/kg |
|---|---|---|---|
| Annualized relapse rate | 0.33 | 0.14 | 0.15 |
| ARR reduction versus placebo | — | 57.6% (p less than 0.001) | 54.5% (p less than 0.001) |
| Patients relapse-free | approximately 60% | approximately 80% | approximately 79% |
| T1 Gd+ lesion reduction | — | approximately 86% | approximately 87% |
| Active T2 lesion reduction | — | approximately 74% | approximately 77% |
| Sustained disability progression | Significantly reduced versus placebo for both doses | — | — |
Source: Giovannoni G et al. A Placebo-Controlled Trial of Oral Cladribine for Relapsing Multiple Sclerosis. NEJM. 2010;362:416–426. doi:10.1056/NEJMoa0902533. CLARITY trial, NCT00213135.
The MRI data was particularly striking. MRI-measured disease activity was greatly reduced by both doses, with significantly greater proportions of patients remaining lesion-free in cladribine groups versus placebo across all lesion types.
CLARITY Extension was designed to answer the durability question, the most important unknown for any induction therapy. Among patients who had received active cladribine in CLARITY and then received only placebo in the extension, a substantial proportion remained free of relapse and MRI disease activity for at least an additional two years. The CLARITY Extension data demonstrated that in a majority of patients, the clinical benefits of cladribine 3.5 mg/kg given in Years 1 and 2 may be maintained for at least four years, with decisions on further treatment based on monitoring during this period. This durability is the clinical core of the cladribine story: a drug that requires 20 days of tablets and then maintains efficacy for four or more years in a meaningful proportion of patients is a fundamentally different treatment proposition from anything else in MS therapy.
Where Cladribine Fits in the MS Treatment Landscape
The MS disease-modifying therapy landscape in 2026 is one of the most complex in all of neurology. Broadly, DMTs divide into two strategic categories: maintenance therapies and induction therapies.
Maintenance therapies require continuous ongoing treatment to suppress disease activity. Stopping them typically leads to return of disease activity. Examples include interferon betas, glatiramer acetate, natalizumab, ocrelizumab, and ofatumumab.
Induction therapies (or immune reconstitution therapies) aim to achieve durable remission through a time-limited course of treatment that fundamentally alters the immune landscape. Cladribine and alemtuzumab are the two primary examples currently approved for MS. Neither requires indefinite continuous dosing if disease control is achieved.
The regulatory positioning of Mavenclad in the U.S. reflects a second-line designation: it is generally recommended for patients who have had an inadequate response to, or are unable to tolerate, an alternate MS drug. In practice, it tends to be used in patients with higher disease activity, either those who have failed a first-line agent or those presenting with highly active disease who require high-efficacy therapy from the start.
| Therapy type | Examples | Dosing | Disease activity level | Key consideration |
|---|---|---|---|---|
| Moderate-efficacy maintenance | Interferons, glatiramer acetate, dimethyl fumarate | Daily, weekly, or biweekly, indefinitely | Low to moderate | Lower side effect burden; lower efficacy ceiling |
| High-efficacy maintenance | Natalizumab, ocrelizumab, ofatumumab | Monthly or biweekly injections/infusions, indefinitely | Moderate to high | High efficacy; ongoing immunosuppression |
| Induction/immune reconstitution | Cladribine, alemtuzumab | Short course over 2 years, then monitor | High or highly active | Durable remission possible; distinct safety profile |
| S1P receptor modulators | Siponimod, ozanimod, fingolimod | Daily oral, indefinitely | Moderate to high | Cardiac monitoring at initiation; rebound risk on discontinuation |
The ORACLE-MS study extended cladribine’s evidence base to patients at their first clinical demyelinating event, the earliest stage of MS diagnosis, showing that cladribine tablets significantly reduced the risk of clinically definite MS compared with placebo. This evidence base is relevant for neurologists seeing patients at initial presentation, though the approved U.S. indication remains restricted to relapsing forms with prior inadequate response.
The Safety Profile
Cladribine’s safety profile reflects its mechanism: a drug that depletes lymphocytes will affect the immune system’s ability to fight infections and carries a malignancy risk that requires ongoing attention.
| Safety item | Details | Clinical guidance |
|---|---|---|
| Lymphopenia | Dose-dependent reduction in lymphocyte counts is expected and is part of the mechanism. Grade 3 lymphopenia occurred in approximately 25% of patients at the 3.5 mg/kg dose; Grade 4 in 0.7%. | Lymphocyte counts must be measured at baseline and during treatment. Do not initiate Year 2 treatment if lymphocyte count has not recovered to the specified threshold. |
| Serious infections | Increased risk due to lymphocyte depletion, including opportunistic infections and reactivation of latent viruses. | Screen for active infections before initiating. Vaccination status should be reviewed and updated at least 4 to 6 weeks before treatment. |
| Herpes zoster | Zoster infections occurred at higher rates in cladribine-treated patients than placebo in clinical trials. | Consider prophylactic antiviral therapy. Patients should be vaccinated against varicella-zoster if not immune before starting cladribine. Live zoster vaccine is contraindicated once treatment begins. |
| Malignancy | Increased risk of malignancy is a class concern for immune reconstitution therapies. A signal was observed in longer-term datasets. | Not recommended in patients with current malignancy. Ongoing cancer screening recommended. Risk-benefit discussion required. |
| Embryo-fetal toxicity (boxed warning) | Cladribine is teratogenic and genotoxic based on animal studies. May cause fetal harm. | Effective contraception required during treatment and for 6 months after the last dose in both female and male patients. Pregnancy testing required before each treatment cycle. Not for use during pregnancy or breastfeeding. |
| Renal impairment | Dose adjustment required in patients with moderate-to-severe renal impairment (CrCl below 60 mL/min). Not studied in severe hepatic impairment. | Assess renal function before initiating. |
| Live vaccines | Contraindicated during treatment due to immunosuppression. | Update all live vaccines before treatment. No live vaccines during the cladribine treatment course. |
The teratogenicity boxed warning creates contraception requirements for women and men of reproductive potential extending 6 months after the last dose, reflecting the genotoxicity concern.
The Patent Story: How Generics Arrived Early
Mavenclad’s patent situation is one of the most significant stories in the 2026 LOE landscape, not because it followed the expected course, but because it did not.
Merck KGaA held multiple patents protecting cladribine tablets for MS, including patents covering specific dosing regimens. Multiple generic manufacturers, including Apotex, Aurobindo, and Accord/Intas, filed Paragraph IV certifications challenging those patents as invalid or not infringed. Merck pursued litigation to defend them.
An appeals court upheld a decision by the U.S. Patent Office that two dosing regimen patents for Mavenclad were invalid. Apotex received full FDA approval for its generic version of cladribine tablets, with the first generic launches arriving in December 2025, roughly 10 to 11 months earlier than Merck had anticipated.
In the Merck versus Apotex case, the court invalidated specific claims of U.S. Patent No. 7,713,947 and U.S. Patent No. 8,377,903, both covering cladribine dosing regimens for treating MS. The claims were found invalid as obvious under 35 U.S.C. § 103, following the Federal Circuit’s binding ruling in Merck Serono S.A. v. Hopewell Pharma Ventures, Inc. in 2025. The court found that the specific dosing regimen claimed in the patents was an obvious extension of what skilled practitioners would have arrived at from prior art, not a novel inventive step warranting patent protection.
This outcome has implications beyond Mavenclad. It demonstrates that method-of-use patents, covering how a drug is dosed rather than what the drug is, face a higher obviousness hurdle when the underlying molecule and its general clinical use are already known. Cladribine had been used in medicine for decades before Mavenclad’s development for MS; the composition-of-matter patent on the molecule had long expired. The only protection Merck had was the MS dosing regimen, and the Federal Circuit concluded that regimen was obvious.
The Merck KGaA versus Aurobindo Pharma case, involving three patents covering cladribine treatment regimens for MS, closed February 2, 2026, after 1,116 days of litigation. Multiple additional ANDA filers are in the pipeline, and the competitive generic landscape for cladribine tablets is expected to expand through 2026 and into 2027.
The Pricing and Access Reality
Brand-name Mavenclad costs approximately $99,500 per annual treatment course at list price. Generic cladribine tablets are currently priced at approximately $15,000 to $22,000 per course, though pricing is still stabilizing as additional manufacturers enter.
A discount of 75 to 85% off list price is significant. For uninsured patients or those in health systems where list price matters, the difference between $100,000 and $15,000 to $22,000 per year represents a transformative access change.
For commercially insured patients, the calculation is more nuanced. Brand Mavenclad may actually cost less than generic at the point of care because of manufacturer copay assistance programs. With insurance plus EMD Serono’s copay assistance program, many commercially insured patients pay $0 to $25 per course. This dynamic, where originator copay assistance makes the brand cheaper for insured patients while the system-level cost remains high, is a familiar feature of the specialty pharmaceutical market and partly explains why payer pressure rather than patient demand drives generic conversion in high-cost specialty drugs.
For uninsured patients, Medicare patients who cannot benefit from commercial copay assistance, and patients in markets without robust insurance coverage, generic entry is materially impactful. The MS patient advocacy community has long flagged Mavenclad’s price as an access barrier, and the generic arrival, even at $15,000 to $22,000, is a meaningful step toward broader reach, particularly as generic competition deepens and prices decline further.
What patients currently on Mavenclad should know: generic cladribine tablets are bioequivalent to Mavenclad. The active ingredient, the dose, and the clinical mechanism are identical. A formulary switch from brand to generic cladribine is therapeutically equivalent. As always, confirm the transition with your neurologist, particularly to ensure that the monitoring schedule and contraception requirements are not disrupted during a coverage or formulary change.
What This Means for the MS Treatment Landscape
Mavenclad’s generic availability matters beyond the economics of a single drug. The MS treatment landscape has historically been dominated by drugs requiring indefinite continuous use, with patient adherence, injection burden, infusion logistics, and continuous immunosuppression as consequences. An affordable short-course oral induction therapy opens a clinical and economic niche that previously existed but was priced out of reach for many patients and health systems.
For neurologists managing MS patients: the arrival of generic cladribine creates a moment to revisit whether any patients who have been hesitant due to cost could now access this therapy. Patients with highly active MS who have not responded adequately to first-line agents, and who value the induction treatment model over continuous daily therapy, are the clearest candidates for this conversation.
For patients with MS who have been following the Mavenclad story: the fundamental science behind cladribine, selective immune reconstitution, durable memory B cell depletion, and a finite treatment course rather than indefinite therapy, is unchanged by the patent invalidation. The pill that cost $100,000 per year and the pill that costs $15,000 to $22,000 per year are the same molecule, with the same mechanism, producing the same clinical effect. The landscape has changed; the biology has not.
For related HED coverage on MS treatment advances in 2026, see our post on the FDA approval of Ocrevus (ocrelizumab) for relapsing-remitting MS in pediatric patients aged 10 and older, which covers the OPERETTA 2 trial data and the comparison between ocrelizumab and fingolimod in the pediatric setting.
Sources
Mavenclad FDA approval: FDA approves cladribine tablets for relapsing forms of multiple sclerosis. FDA.gov. March 29, 2019.
Merck KGaA LOE impact statement: Merck KGaA signals end of Mavenclad’s blockbuster era. FirstWord Pharma. March 5, 2026.
Generic cladribine availability: Generic Mavenclad Availability. drugs.com.
Generic pricing: Cladribine 2026: What Patients Need to Know. Medfinder. March 2026. | How to Save Money on Cladribine in 2026. Medfinder. May 2026.
Patent invalidation (Apotex case): Merck vs. Apotex: Cladribine MS Patents Ruled Invalid as Obvious. PatSnap Eureka. February 2026.
Patent litigation (Aurobindo case): Merck KGaA vs. Aurobindo Pharma: Cladribine MS Patent Dispute Closes. PatSnap Eureka. March 2026.
CLARITY trial primary publication: Giovannoni G et al. A Placebo-Controlled Trial of Oral Cladribine for Relapsing Multiple Sclerosis. NEJM. 2010;362:416–426. doi:10.1056/NEJMoa0902533.
CLARITY trial registration: NCT00213135. ClinicalTrials.gov.
CLARITY Extension: Giovannoni G et al. Safety and efficacy of cladribine tablets in patients with RRMS: results from the CLARITY extension. Mult Scler. 2018;24:1594–1604. PMID 29307230.
Memory B cell depletion mechanism: Baker D et al. Cladribine treatment of MS is associated with depletion of memory B cells. J Neurol. 2017;264:2052–2060. PMC5937883.
SIRT classification: Baker D et al. Potential mechanisms of action related to the efficacy and safety of cladribine. Multiple Sclerosis and Related Disorders. 2019. PMID 31362145.
Lymphocyte reconstitution kinetics: Comi G et al. Changes in lymphocytes, neutrophils and immunoglobulins in year-1 cladribine treatment. Multiple Sclerosis and Related Disorders. 2021.
ORACLE-MS (clinically isolated syndrome): Leist TP et al. Effect of Oral Cladribine on Time to Conversion to Clinically Definite MS. JAMA Neurol. 2014;71(10):1278–1286. doi:10.1001/jamaneurol.2014.1947.
Cladribine StatPearls: Cladribine. StatPearls. NCBI.
MS overview: Multiple Sclerosis. StatPearls. NCBI.
Interferon betas: Interferon Beta. StatPearls. NCBI.
Alemtuzumab FDA approval: FDA approves alemtuzumab for multiple sclerosis. FDA.gov.
Lymphopenia: Lymphopenia. StatPearls. NCBI.
Herpes zoster: Herpes Zoster. StatPearls. NCBI.
Mavenclad prescribing information: Mavenclad (cladribine) tablets Prescribing Information. EMD Serono.
National MS Society disease types: Types of MS. nationalmssociety.org.
Patient resources: National Multiple Sclerosis Society | Can Do MS | EMD Serono Mavenclad patient support
| Disclaimer: Health Evidence Digest provides general information about FDA approvals, loss of exclusivity events, and health research for educational purposes. This content is not a substitute for professional medical advice. Multiple sclerosis treatment decisions, including the choice of disease-modifying therapy and transitions between brand-name and generic products, should be made in close collaboration with a board-certified neurologist specializing in MS. Patients must follow all pregnancy prevention and monitoring requirements associated with cladribine therapy. |
|---|
Leave a Reply