| 📌 The essentials Gattex (teduglutide, Takeda) is a GLP-2 analog approved for adults and children aged 1 year and older with short bowel syndrome (SBS) who are dependent on parenteral nutrition. Mechanism: teduglutide binds GLP-2 receptors on subepithelial myofibroblasts and enteric neurons, triggering paracrine release of growth factors that increase villus height, crypt depth, intestinal blood flow, and barrier integrity. The net result is increased absorptive surface area and reduced need for intravenous nutrition support. FDA approval: December 21, 2012 for adults; extended to pediatric patients aged 1 year and older in subsequent approvals. Last pediatric exclusivity expired May 16, 2026. Seven patent litigation cases have been filed by generic challengers. The STEPS pivotal trial: 63% of patients achieved at least a 20% reduction in parenteral nutrition volume at 24 weeks versus 30% with placebo (p less than 0.001). Long-term extension data: 16 of 134 patients (approximately 12%) achieved complete parenteral nutrition independence after a mean of 89 weeks of teduglutide treatment. Annual cost: exceeds $700,000 for adults at current list price. Cost-effectiveness modeling has found that teduglutide does not meet traditional cost-effectiveness thresholds except in subpopulations achieving maximum benefit. Mandatory colonoscopy surveillance: colonoscopy within 6 months before initiating Gattex and every 5 years thereafter is required due to the theoretical risk of accelerating growth of pre-existing colorectal polyps or neoplasia. Note on regulatory pathway: teduglutide is a recombinant 33-amino acid peptide. Follow-on products may proceed via biosimilar aBLA or via 505(b)(2) NDA or ANDA pathways depending on the FDA’s regulatory classification, a determination that may differ for individual manufacturers. |
|---|
| 📚 About this series: the 2026 Loss of Exclusivity Watch This is Post 7 of HED’s 2026 Loss of Exclusivity series, tracking the ten major drugs losing U.S. exclusivity this year. The full series covers: Xolair (omalizumab) • Pomalyst (pomalidomide) • Opsumit (macitentan) • Januvia/Janumet (sitagliptin) • Simponi (golimumab) • Mavenclad (cladribine) • Gattex (teduglutide) • Trintellix (vortioxetine) • Briviact (brivaracetam) • Xeljanz (tofacitinib). Each post follows the same format: what the drug is and how it works, what the clinical evidence shows, who uses it and why, and what the entrance of competition means for patients, prescribers, and the market. |
|---|
There is a small corner of clinical medicine where patients survive on bags of liquid nutrition delivered directly into a vein, every night, sometimes for the rest of their lives. A pump. A central line catheter tunneled under the skin. Hours tethered to an IV pole before they can sleep. The condition is called intestinal failure, and for patients with short bowel syndrome, it is not a temporary inconvenience. It is the permanent consequence of having lost so much of their small intestine that what remains cannot absorb enough nutrients to sustain life.
Short bowel syndrome (SBS) is a rare disorder with known physical, psychosocial, and economic burdens and significant morbidity and mortality. Many individuals with SBS require long-term home parenteral nutrition (PN). The most common etiologies in adults are Crohn’s disease and mesenteric ischemia. Intestinal anatomy and remnant bowel length are prognostic for parenteral nutrition dependency, and achieving enteral autonomy confers a meaningful survival advantage.
Gattex (teduglutide) is unusual even by orphan drug standards because its mechanism is not suppression, replacement, or blockade. It asks the intestine to grow. Teduglutide is a GLP-2 analog that reduces dependence on parenteral nutrition in patients with SBS by promoting enterocytic proliferation and increasing absorptive surface area. A drug that literally stimulates the remnant intestinal lining to expand, absorb more, and, for a meaningful fraction of patients, allow the eventual reduction or elimination of intravenous nutritional support. That is a fundamentally different therapeutic proposition from most drugs in medicine.
Gattex was approved by the FDA on December 21, 2012 for adult patients with SBS dependent on parenteral support, and later expanded to include pediatric patients aged 1 year and older. Its last pediatric exclusivity expired on May 16, 2026. Seven patent litigation cases have been filed by generic challengers, indicating strong commercial interest in launch. No follow-on product has yet been approved.
This post covers what short bowel syndrome and intestinal failure actually are, why teduglutide’s GLP-2 mechanism is scientifically distinctive, what the STEPS pivotal trial and long-term extension data show, what the mandatory colonoscopy surveillance requirement means and why it exists, the cost and access reality of a drug exceeding $700,000 per year, and what the LOE means for a patient population that is both tiny and profoundly treatment-dependent.
What Short Bowel Syndrome Is and What Living With It Looks Like
The small intestine in a healthy adult measures roughly six to seven meters in length. It is the primary site of nutrient and fluid absorption, where digested food crosses from the gut lumen into the bloodstream and where fats, proteins, carbohydrates, vitamins, and minerals are taken up to sustain every organ and process in the body.
SBS in adults is characterized by the European Society for Clinical Nutrition and Metabolism as the clinical condition associated with a remaining small bowel in continuity of less than 200 cm. When that much intestine is absent, either surgically removed or non-functional, what remains cannot absorb enough to sustain the person without supplemental support. The result is intestinal failure.
SBS can develop at any age and from multiple causes:
| Cause | Population | Notes |
|---|---|---|
| Crohn’s disease with repeated resections | Adults | Cumulative surgical bowel loss over years of disease; most common adult SBS etiology |
| Mesenteric ischemia | Adults, often older | Vascular occlusion leading to extensive bowel necrosis; often acute and catastrophic |
| Volvulus (intestinal twisting) | Any age | Can occur in neonates (midgut volvulus) or adults |
| Necrotizing enterocolitis (NEC) | Premature neonates | Leading cause of SBS in pediatric populations; premature gut tissue undergoes inflammatory necrosis |
| Gastroschisis and congenital abnormalities | Neonates | Congenital bowel defects requiring extensive resection at birth |
| Trauma or radiation enteritis | Adults | Less common; direct physical injury or radiation damage to bowel |
The clinical consequences of intestinal failure are multisystemic. Patients must receive total parenteral nutrition (TPN), intravenous delivery of all macronutrients, micronutrients, electrolytes, and fluids. Home PN typically requires 10 to 16 hours of infusion per night through a central venous catheter. The catheter is a permanent source of risk: central line-associated bloodstream infections (CLABSIs) are a leading cause of morbidity and death in this population. Long-term PN also causes parenteral nutrition-associated liver disease, cholestatic damage that can progress to cirrhosis and liver failure over years, particularly in children. It is this PN dependence that is responsible for the majority of morbidity and mortality associated with SBS, including catheter infections and PN-induced cholestatic liver dysfunction.
In the United States, the prevalence of SBS-associated intestinal failure requiring home PN is estimated at roughly 10,000 to 15,000 adults and several thousand children. It is genuinely rare, which is why Gattex received orphan drug designation and why its development took decades from the initial discovery of its target hormone.
The Science: What GLP-2 Does and Why Teduglutide Was Engineered the Way It Was
The story of teduglutide begins with a discovery made in the 1990s about a gut hormone most people have never heard of: glucagon-like peptide-2 (GLP-2).
GLP-2 is a 33-amino acid peptide secreted by L-cells in the distal small intestine and colon in response to food intake. It acts as a trophic hormone for the intestinal epithelium. When researchers administered GLP-2 to mice, the results were striking: GLP-2 produced a 50% increase in small bowel weight, significantly taller villi, and deeper crypts, with no effect on other organs. This identified GLP-2 as a specific intestinal growth factor and immediately suggested therapeutic potential for intestinal failure.
The problem with using native GLP-2 as a drug is its half-life: approximately 7 minutes. The enzyme DPP-4, the same dipeptidyl peptidase-4 that sitagliptin (covered in Post 4 of this LOE series) inhibits, rapidly cleaves and inactivates native GLP-2 in circulation. A drug with a 7-minute half-life would require continuous intravenous infusion, not a practical therapeutic option.
A single amino acid substitution, replacing glycine with alanine at position 2, renders teduglutide resistant to DPP-4 degradation, extending its half-life from approximately 7 minutes to approximately 2 hours. This single amino acid change is the molecular engineering that made teduglutide viable as a once-daily subcutaneous injection rather than a continuous infusion.
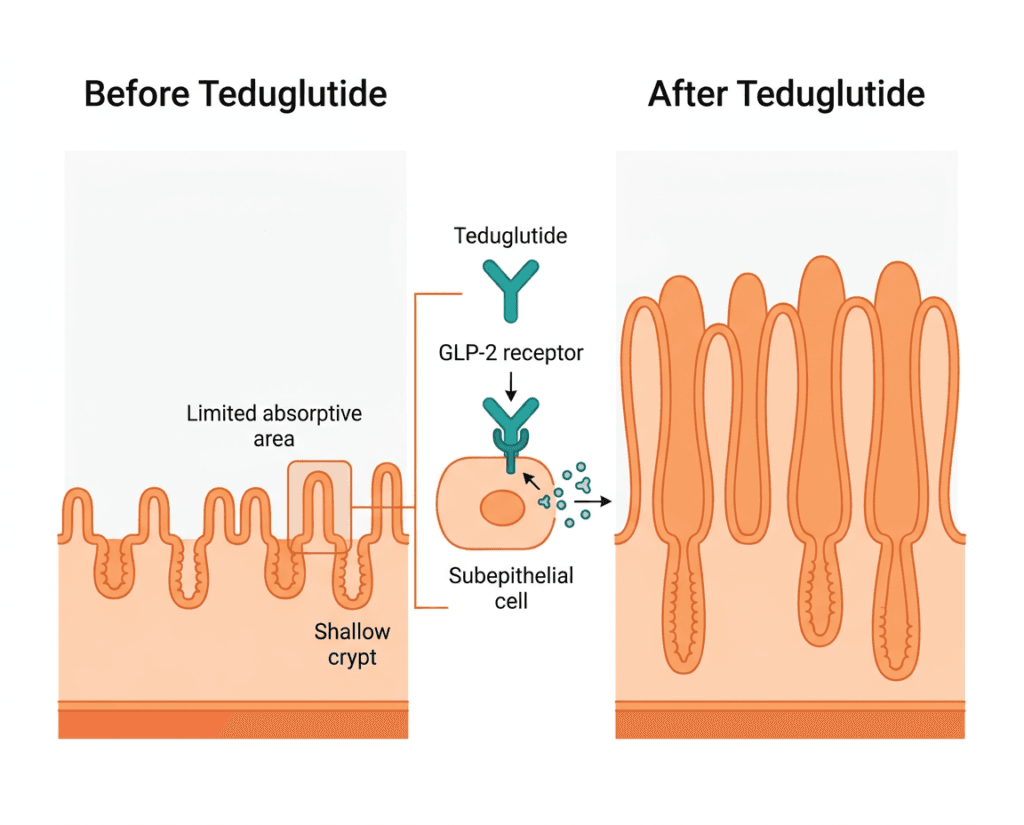
The mechanism through which GLP-2 and teduglutide promote intestinal growth is indirect: GLP-2 receptors are not expressed on intestinal epithelial cells themselves. Instead, GLP-2 binds receptors on subepithelial myofibroblasts and enteric neurons, triggering paracrine release of growth factors that promote villus growth, crypt proliferation, barrier repair, and reduced inflammation.
The downstream effects are multiple and coordinated: teduglutide reduces accelerated gastric emptying and gastric hypersecretion, increases intestinal blood flow, promotes the growth of enterocytes, increases villus height and crypt depth, improves intestinal barrier function, and accelerates the process of intestinal adaptation. The sum of these effects is an intestinal lining that is structurally larger, better perfused, and more functionally capable of absorbing fluid and nutrients, meaning the same length of remnant bowel can do more work than it could before teduglutide.
The STEPS Trial and Clinical Evidence
STEPS (Study of Teduglutide Effectiveness in Parenteral Nutrition-Dependent Short Bowel Syndrome) was the pivotal Phase 3 trial that supported Gattex’s 2012 FDA approval. It enrolled 86 adult patients with SBS-associated intestinal failure dependent on parenteral nutrition, randomizing them to teduglutide 0.05 mg/kg/day subcutaneous injection or placebo for 24 weeks.
| Outcome | Placebo | Teduglutide 0.05 mg/kg/day | Significance |
|---|---|---|---|
| Achieved at least 20% PN volume reduction at Week 24 | 30% of patients | 63% of patients | p less than 0.001 |
| Mean PN volume reduction | approximately 2 liters per week | approximately 4.4 liters per week | Statistically significant |
| Patients achieving at least 1 day/week reduction in PN days | 27% | 54% | Statistically significant |
| Villus height increase | Not significant | Significant increase | Structural intestinal growth confirmed |
| Plasma citrulline increase | — | Significant increase | Citrulline as biomarker of functional enterocyte mass |
The 20% PN volume reduction threshold used as the primary endpoint was specifically chosen because it represents a clinically meaningful reduction in infusion time and catheter infection risk. Reducing PN by 20% or more translates to roughly 1 to 2 fewer infusion nights per week for some patients, which has measurable quality-of-life implications.
Long-term extension data told a more complete story about what the drug can achieve over time. A post-hoc analysis of the teduglutide clinical trial program, including two Phase 3 trials and their extension studies, revealed that 16 of 134 patients (approximately 12%) gained complete oral or enteral autonomy from nutritional support after a median of 5 years of previous PN dependence, after a mean duration of 89 weeks of teduglutide treatment. Complete PN independence can occur later in the course of therapy, even after one to two years of administration, meaning that patients and clinicians who see partial benefit early should not discontinue prematurely before the full adaptive potential of the intestine has been realized.
Complete PN independence is the most profound outcome in SBS management: a patient who no longer needs nightly IV nutrition, no longer requires a central line catheter, and can eat and drink without fear that what they consume cannot sustain them. Achieving it in 12% of a population that has been PN-dependent for a median of 5 years is a clinically meaningful milestone, even if the majority of patients achieve meaningful PN reduction rather than full independence.
The Colonoscopy Requirement: Why It Exists and What It Means Clinically
This is the safety element most distinctive to teduglutide and the one most directly tied to its mechanism.
Because teduglutide stimulates intestinal epithelial cell proliferation, it also theoretically accelerates the growth of any pre-existing neoplastic or pre-neoplastic tissue. GLP-2 analog activity on intestinal crypts is not selective between normal mucosa and polyps. The FDA’s response to this theoretical risk is mandatory surveillance: colonoscopy of the entire colon with removal of polyps should be performed within 6 months prior to initiating Gattex therapy and every 5 years thereafter, or more frequently as clinically indicated.
The practical implications for patients are significant. In SBS patients, many of whom are older adults with multiple comorbidities, a history of extensive GI surgery, and significant differences in intestinal anatomy, colonoscopy preparation and procedure carries higher procedural risk than in the average screening population. The discussion of whether colonoscopy surveillance is feasible and appropriate for a given patient should be part of the informed consent process before initiating teduglutide.
Importantly, the clinical trial data showed that polyp rates on teduglutide were not dramatically elevated compared to placebo: a pilot study found the occurrence of polyps was similar before and after treatment and included only low-grade dysplastic lesions. The surveillance requirement is precautionary rather than based on an established excess malignancy signal. Nonetheless, it is mandatory per the prescribing information and should not be deferred.
The Safety Profile
| Safety item | Details | Clinical guidance |
|---|---|---|
| Colorectal neoplasia (warning) | Potential for accelerated polyp or neoplasia growth due to GLP-2 intestinal proliferative mechanism. Colorectal polyps identified in clinical trials. | Colonoscopy within 6 months before initiating; every 5 years during therapy or more often as clinically indicated. Discontinue in patients with active GI malignancy. |
| Fluid and electrolyte disturbances | Improved intestinal absorption can alter fluid and electrolyte balance rapidly, particularly in patients concurrently receiving PN. | Monitor fluid and electrolyte balance carefully when initiating therapy. PN volumes may need reduction within weeks. Over-absorption leading to fluid overload is possible, particularly in patients with cardiac or renal comorbidities. |
| Intestinal obstruction | Cases reported; may reflect underlying SBS anatomy or the effect of increased intestinal motility and tone. | Evaluate for obstruction if symptoms develop. Temporary discontinuation may be required; permanent discontinuation if obstructive symptoms recur. |
| Biliary and pancreatic disease | Cholecystitis, cholangitis, cholestasis, and pancreatitis reported in post-marketing experience. | Discontinue if these complications develop. Monitor for symptoms especially in patients with prior biliary disease. |
| Stoma output changes | Patients with stomas may experience significant increases in stoma output with improved absorption. | Monitor stoma output; adjust hydration and PN accordingly. |
| Acceleration of underlying GI disease | In patients with residual GI disease such as Crohn’s, the trophic effect could theoretically accelerate underlying pathology. | Clinical judgment required; monitor for exacerbation of underlying disease. |
| Cardiac comorbidity | Fluid retention risk relevant in patients with heart failure or reduced cardiac function. | Use with caution; careful monitoring of fluid status required. |
| Renal impairment | Dose reduction to 0.025 mg/kg once daily required in patients with moderate to severe renal impairment (eGFR below 60 mL/min/1.73m²). | Check kidney function at baseline and monitor during therapy. |
| Injection site reactions | Common: redness, pain at the site of subcutaneous injection. | Rotate injection sites. |
The Cost Reality: When a Drug Exceeds $700,000 a Year
The current list price for adult dosing of teduglutide exceeds $700,000 per year. For pediatric patients, weight-based dosing produces lower daily doses and somewhat lower annual costs, but still reaches hundreds of thousands of dollars.
To contextualize this against the condition it treats: home parenteral nutrition itself is extremely expensive. Annual PN costs for an SBS patient in the United States range from approximately $150,000 to $300,000 or more per year depending on volume, complexity, and frequency of infusions. The economic case for teduglutide hinges on whether reducing PN dependence produces cost savings that offset the drug’s price.
Published cost-effectiveness modeling is sobering. Seidner et al. found that teduglutide does not meet traditional cost-effectiveness thresholds as a treatment for PN reduction in adult SBS patients compared with standard intestinal rehabilitation. Subpopulations demonstrating maximum benefit could represent cost-saving scenarios, and teduglutide becomes economically reasonable only if its cost is substantially reduced.
In practice, coverage decisions vary substantially by payer. Many commercial insurers cover teduglutide with prior authorization and documented PN dependence. Medicare and Medicaid coverage exists but may require appeals and documentation of medical necessity. For the approximately 12% of treated patients who achieve complete PN independence, the economic calculus shifts dramatically: eliminating the cost of home PN entirely changes the math. For the majority who achieve meaningful PN reduction without full independence, the system is paying more than $700,000 per year for a benefit that is real but falls short of the most transformative outcome.
Takeda’s patient support program provides access and financial assistance navigation for eligible patients. The Oley Foundation, which specifically serves home PN and tube-fed patients, and the National Organization for Rare Disorders are the primary patient community resources.
The Generic and Follow-On Landscape: Why This LOE Is Unique
Gattex’s LOE story has a wrinkle that distinguishes it from both the small-molecule generics (sitagliptin, cladribine) and the biologics (golimumab, omalizumab) in this series. Teduglutide is a recombinant 33-amino acid peptide, which places it in a regulatory category that the FDA has approached differently for different manufacturers over time.
Under the Biologics Price Competition and Innovation Act (BPCIA), large biologics follow the biosimilar aBLA pathway. However, for small peptides, the FDA has also permitted 505(b)(2) NDAs and in some cases standard ANDA pathways where clinical bridging studies can establish equivalence without a full biosimilar data package. The specific pathway for any given teduglutide follow-on product will depend on the FDA’s classification determination for that application. This regulatory ambiguity is not unique to teduglutide: the FDA has published guidance on peptide drug products noting that these determinations are made on a product-by-product basis.
Multiple generic or follow-on manufacturers have filed Paragraph IV patent challenges against Gattex, with seven patent litigation cases filed in total. Two cases remain active. The specific patents challenged cover composition of matter, manufacturing processes, and methods of treatment. The patient population is small enough, and the specialty care infrastructure required to manage SBS complex enough, that competitive launch dynamics here will look nothing like the broad retail pharmacy competition seen with sitagliptin or cladribine.
For patients currently on Gattex: access through Takeda’s specialty pharmacy network will continue unaffected by the LOE. Any formulary transitions to a follow-on product, when they eventually occur, should be managed through the gastroenterology or intestinal rehabilitation team overseeing the patient’s SBS care, not handled at a retail pharmacy level.
What This Means for Patients and Their Families
Short bowel syndrome and intestinal failure exist in a medical ecosystem that most people, including most physicians, have never directly encountered. Patients are managed at specialized intestinal rehabilitation programs at academic medical centers, with multidisciplinary teams including gastroenterologists, dietitians, pharmacists, nurses, and surgeons. The complexity of managing fluid balance, central line care, PN formulation, and the monitoring requirements for teduglutide means that this drug is never managed casually.
For patients currently on Gattex who are responding: treatment should not be discontinued without a specialist’s guidance. The intestinal adaptation that teduglutide has supported may regress over weeks to months after stopping. The colonoscopy surveillance requirement is mandatory throughout treatment, not optional.
For patients or families newly diagnosed with SBS and learning about treatment options: the conversation about teduglutide belongs at a center with intestinal rehabilitation expertise. The drug’s complexity, from the colonoscopy prerequisite to the fluid monitoring to the PN dose adjustments triggered by improving absorption, requires a team that manages this routinely. The Oley Foundation maintains a provider directory and connects SBS patients with peer support networks.
For pediatric patients: the expanded approval to children as young as 1 year old, and the long-term case reports of children weaned from PN dependence with teduglutide, represent a genuinely hopeful development in a disease where neonatal-onset SBS has historically carried sobering long-term outcomes.
For related HED coverage on other pediatric gastroenterological approvals and rare disease drug access, see our post on Linzess (linaclotide) expanding its approval to children as young as 2 years old for functional constipation and our post on Hepcludex (bulevirtide), the first FDA-approved treatment for hepatitis delta, both covering the rare disease treatment access landscape in 2026.
Sources
Gattex FDA approval: FDA approves teduglutide for short bowel syndrome. FDA.gov. December 21, 2012.
Gattex prescribing information: Gattex (teduglutide) Prescribing Information. Takeda Pharmaceuticals. 2024.
Patent expiry and generic interest: GATTEX Loss of Exclusivity. DrugPatentWatch.
GLP-2 discovery and teduglutide engineering: Drucker DJ et al. The Discovery of GLP-2 and Development of Teduglutide for Short Bowel Syndrome. ACS Pharmacology and Translational Science. 2019. doi:10.1021/acsptsci.9b00016.
GLP-2 mechanism review: GLP-2 and intestinal adaptation. PMC6720278.
DPP-4 and incretin system: Ahrén B. DPP-4 Inhibition and the Path to Clinical Proof. Frontiers in Endocrinology. 2019. PMC6593050.
Long-term PN independence data: Drucker DJ et al. ACS Pharmacology and Translational Science. 2019.
SBS epidemiology and PN dependence: Winkler M, Tappenden K. Epidemiology, survival, costs, and quality of life in adults with SBS. Nutr Clin Pract. 2023;38(S1):S17–S26. doi:10.1002/ncp.10964. | Siddiqui MT et al. Short-bowel syndrome: epidemiology, hospitalization trends, in-hospital mortality, and healthcare utilization. JPEN. 2021;45(7):1441–1455. doi:10.1002/jpen.2051.
Cost-effectiveness modeling: Seidner DL et al. Cost-effectiveness of teduglutide in adult patients with SBS. JPEN. 2020. PMC7307185.
Gattex cost reference: Gattex (teduglutide) prices and financial assistance. MedicalNewsToday. June 2025.
SBS StatPearls: Short Bowel Syndrome. StatPearls. NCBI.
Total parenteral nutrition: Total Parenteral Nutrition. StatPearls. NCBI.
PN-associated liver disease: Parenteral Nutrition-Associated Cholestasis. PMC6547003.
Mesenteric ischemia: Mesenteric Ischemia. StatPearls. NCBI.
Necrotizing enterocolitis: Necrotizing Enterocolitis. StatPearls. NCBI.
Crohn’s disease: Crohn’s Disease. NIDDK.
Orphan drug program: Orphan Drug Act. FDA.gov.
BPCIA biosimilar pathway: Biosimilars. FDA.gov.
CLABSI infections: Central Line-Associated Bloodstream Infections. CDC.
NIDDK SBS overview: Short Bowel Syndrome. NIDDK.
HED internal references: LOE Post 4: Januvia/sitagliptin | Linzess pediatric approval post | Hepcludex hepatitis delta post
Patient resources: Oley Foundation | National Organization for Rare Disorders | Gattex patient support
| Disclaimer: Health Evidence Digest provides general information about FDA approvals, loss of exclusivity events, and health research for educational purposes. This content is not a substitute for professional medical advice. Short bowel syndrome and intestinal failure require management by specialized multidisciplinary intestinal rehabilitation teams. Decisions about initiating, continuing, or transitioning from teduglutide therapy should be made in close collaboration with a gastroenterologist or intestinal rehabilitation specialist experienced in SBS management. Drug pricing information reflects estimates at time of publication and is subject to change. |
|---|
Leave a Reply