| 📌 The essentials On May 8, 2026, the FDA approved Bizengri (zenocutuzumab-zbco, Partner Therapeutics) for adults with advanced, unresectable or metastatic cholangiocarcinoma harboring a neuregulin 1 (NRG1) gene fusion with disease progression on or after prior systemic therapy. This is the first FDA-approved targeted therapy specifically for NRG1 fusion-positive (NRG1+) cholangiocarcinoma. Bizengri’s third approved indication: it was previously approved in December 2024 for NRG1+ non-small cell lung cancer and NRG1+ pancreatic adenocarcinoma. Bizengri is now the only approved therapy for NRG1+ solid tumors across three different cancer types. The approval was expedited by a Commissioner’s National Priority Voucher (CNPV), awarded May 6, 2026 and used to compress the review timeline. The clinical basis: Phase 1/2 eNRGy trial (NCT02912949), cholangiocarcinoma cohort of 19 evaluable patients. ORR: 36.8% (95% CI 16.3 to 61.6%). Duration of response: 2.8 to 12.9 months. Regulatory designations: Breakthrough Therapy Designation (October 2025), Orphan Drug Designation (February 2026). Critical testing requirement: NRG1 fusions must be detected using comprehensive molecular testing, specifically tissue-based RNA sequencing, to reliably identify eligible patients. DNA-based testing alone may miss NRG1 fusions. Dosing: 750 mg IV every 2 weeks. |
|---|
Cholangiocarcinoma, commonly called bile duct cancer, is an aggressive malignancy arising from the epithelial cells lining the bile ducts. It is rare, accounting for approximately 3% of all gastrointestinal cancers globally, but deadly: the five-year survival rate for metastatic disease is below 10%, and most patients are diagnosed at stages where surgery is not possible.
The treatment landscape for cholangiocarcinoma has evolved rapidly in recent years. Several actionable molecular targets have been identified in subsets of the disease, including FGFR2 fusions, IDH1 mutations, BRAF V600E mutations, HER2 amplification, and now NRG1 fusions. Each molecular subset represents a small fraction of the total cholangiocarcinoma population, but targeted therapy for each has produced response rates substantially higher than chemotherapy alone in those patients who carry the specific molecular alteration.
On May 8, 2026, patients with NRG1 fusion-positive cholangiocarcinoma gained their first approved targeted option. Bizengri (zenocutuzumab-zbco), a bispecific antibody targeting HER2 and HER3, was approved based on a 36.8% objective response rate in 19 evaluable patients in the eNRGy trial cholangiocarcinoma cohort. In a disease with no prior approved targeted therapy for this molecular subset, that number represents a clinically meaningful new option for a population that has had very few.
What NRG1 Fusions Are and Why They Matter Across Multiple Cancers
To understand why Bizengri works across NSCLC, pancreatic cancer, and now cholangiocarcinoma, it helps to understand what an NRG1 fusion is and what biological pathway it activates.
The NRG1 gene and neuregulin signaling
NRG1 (neuregulin 1) encodes a family of growth factor proteins called neuregulins that are ligands for HER3 (ErbB3), a member of the HER receptor tyrosine kinase family. When neuregulin 1 binds HER3, it triggers HER3 to heterodimerize preferentially with HER2 (ErbB2), forming a signaling complex that activates downstream proliferation and survival pathways including PI3K/AKT and MAPK/ERK.
In normal tissue, NRG1 signaling through HER3/HER2 is tightly regulated and context-dependent. In cancers with NRG1 gene fusions, the NRG1 coding sequence is joined to the sequence of a partner gene, creating a fusion protein that is expressed at abnormally high levels, constitutively activates HER3/HER2 signaling, and drives cancer cell proliferation in a fusion-dependent manner.
NRG1 fusions are found across multiple solid tumor types but are rare in each individual cancer: prevalence estimates of approximately 0.2% of all solid tumors, with higher rates in certain histologies. In cholangiocarcinoma, NRG1 fusions are estimated to occur in approximately 1 to 2% of cases, representing a very small molecular subset of an already rare cancer. In the United States, this translates to only a few hundred patients per year.
| The testing challenge: why DNA sequencing alone may miss NRG1 fusions NRG1 fusions are gene rearrangements that join introns of two different genes. Because the fused protein is produced from the rearranged mRNA rather than from a simple point mutation or small insertion/deletion, RNA-based sequencing (which reads transcribed mRNA) detects NRG1 fusions more reliably than standard DNA-based next-generation sequencing. Partner Therapeutics specifically noted in the approval documentation that comprehensive molecular testing, particularly tissue-based RNA sequencing, is essential to reliably detect NRG1 fusions and identify eligible patients. Oncologists managing cholangiocarcinoma patients should ensure that their molecular profiling platform includes RNA-based fusion detection, as DNA sequencing alone may produce false-negative results. This is a critical testing consideration that distinguishes NRG1 fusion detection from some other molecular targets in oncology. |
|---|
What Zenocutuzumab Is and How It Works
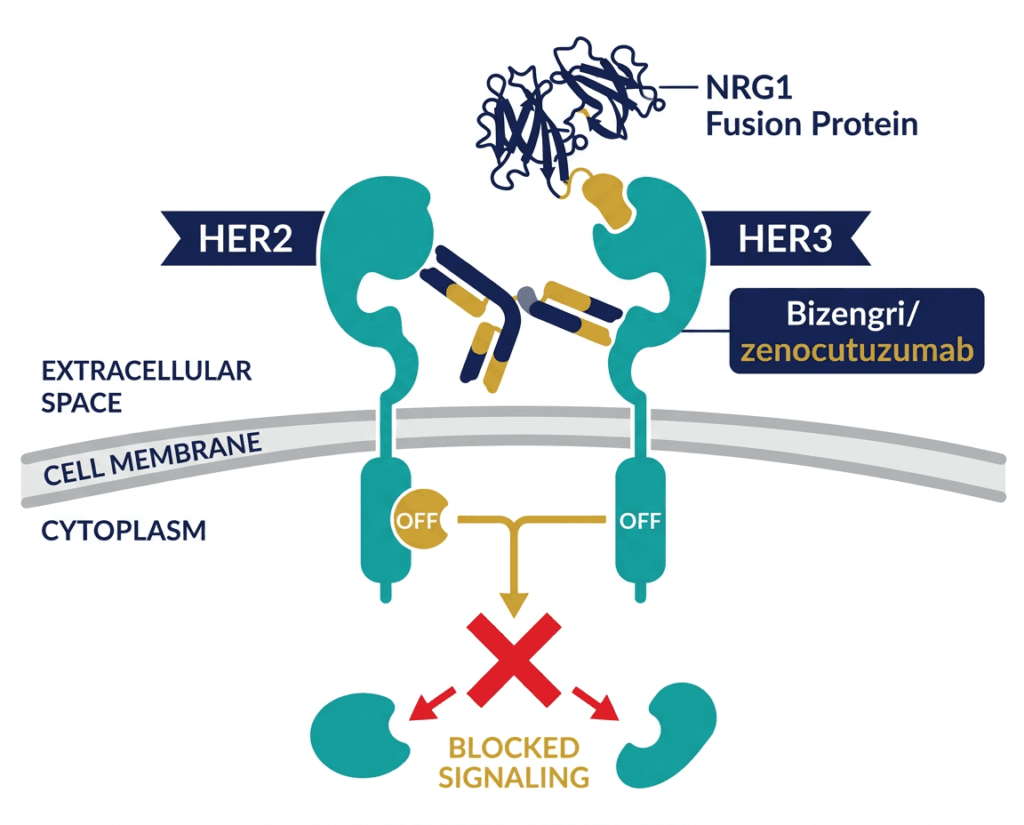
Zenocutuzumab (brand name Bizengri) is a bispecific antibody, meaning it is engineered to bind two different molecular targets simultaneously. Specifically, it targets both HER2 and HER3 simultaneously using a single antibody molecule. This dual targeting is the key to its mechanism in NRG1 fusion-positive tumors.
The mechanism of action exploits a specific vulnerability in NRG1 fusion-driven cancer cells:
In NRG1+ tumors, the fusion protein acts as an overexpressed HER3 ligand, continuously stimulating HER3 on the cancer cell surface to heterodimerize with HER2. Zenocutuzumab blocks this process by binding both HER3 and HER2 simultaneously: its HER3-binding arm prevents the NRG1 fusion protein from docking with HER3, while its HER2-binding arm prevents HER2 from forming its signaling-competent heterodimer with HER3. The result is that the constitutive NRG1 fusion-driven HER3/HER2 signaling loop is interrupted at two points simultaneously.
This dual blockade strategy is mechanistically rational for NRG1 fusion-driven tumors in a way that single-target approaches are not. Blocking only HER3 might be insufficient if HER2 can still be activated by other means; blocking both removes the substrate and the dimerization partner of the constitutively active signaling complex.
Zenocutuzumab does not work in tumors where HER2/HER3 signaling is activated by HER2 gene amplification or overexpression rather than NRG1 fusion. Its mechanism requires the NRG1 fusion to be the driver. This is why patient selection by molecular testing is not optional but essential for appropriate use.
Bizengri’s Three Approved Indications: A Tumor-Agnostic Approach to a Single Molecular Target
Bizengri is now approved across three cancer types defined by the same molecular alteration:
| Indication | Approval date | Setting |
|---|---|---|
| NRG1+ non-small cell lung cancer | December 4, 2024 | After prior systemic therapy |
| NRG1+ pancreatic adenocarcinoma | December 4, 2024 | After prior systemic therapy |
| NRG1+ cholangiocarcinoma (biliary tract) | May 8, 2026 | After prior systemic therapy |
This approval strategy, using one molecular biomarker to justify approval across histologically distinct cancers, is the definition of a tumor-agnostic or biomarker-driven approach. The NRG1 fusion is the target, and the tissue of origin is secondary. This pattern follows the FDA’s broader shift toward molecular rather than anatomical cancer classifications, exemplified by earlier tumor-agnostic approvals such as pembrolizumab for MSI-H/dMMR tumors and larotrectinib for TRK fusion-positive cancers.
The CNPV connection is also relevant here. For related coverage of how the CNPV program has been used to accelerate approvals for other conditions in 2026, see our post on the FDA’s fast-tracking of psychedelic drug programs for mental illness and our post on the first gene therapy for genetic deafness, the first gene therapy approved under CNPV.
The eNRGy Trial Cholangiocarcinoma Cohort: What the Evidence Shows
Trial design
eNRGy (NCT02912949) is a Phase 1/2, open-label, registrational, multicenter basket trial evaluating zenocutuzumab across multiple solid tumor types harboring NRG1 fusions. The basket design is appropriate for rare molecular alterations that appear across multiple histologies: rather than running a separate trial for each tumor type, a single trial enrolls all patients with the molecular target regardless of where the cancer originated.
The cholangiocarcinoma cohort enrolled patients with advanced, unresectable or metastatic cholangiocarcinoma harboring NRG1 gene fusions whose disease had progressed on or after prior systemic therapy. NRG1 fusion status was required to be confirmed by molecular testing.
Efficacy results
| Outcome | Cholangiocarcinoma cohort (n=19 evaluable) |
|---|---|
| Overall response rate (ORR) | 36.8% (95% CI 16.3 to 61.6%) |
| Number of confirmed responders | 7 of 19 patients |
| Duration of response | Range: 2.8 to 12.9 months |
| Assessment method | RECIST v1.1, blinded independent central review |
Source: FDA approval, May 8, 2026. Presented at AACR/NCI/EORTC Conference on Molecular Targets and Cancer Therapeutics, October 2025, Boston.
Interpreting the results in context
A 36.8% ORR in a 19-patient cohort must be understood within the context of several important facts.
The denominator is tiny because the disease is rare. NRG1 fusion-positive cholangiocarcinoma affects only an estimated few hundred Americans per year. Running a trial large enough to power a survival analysis in this population would take many years and deny patients in the interim a therapy that is producing clinically meaningful responses. The FDA’s standard for approvals in ultra-rare molecularly defined cancers appropriately accounts for this constraint.
The comparator context is chemotherapy. Historically, patients with advanced cholangiocarcinoma whose disease has progressed after first-line therapy have had very limited options with response rates in the range of 5 to 15% to second-line chemotherapy. A 36.8% ORR against this background represents a meaningfully differentiated result.
The basket trial precedent is established. The NSCLC and pancreatic cancer approvals from December 2024 were based on the same eNRGy trial using the same basket design. In the NSCLC cohort (n=30), the ORR was 33% with a median duration of response of 7.4 months. In the pancreatic cohort (n=30), the ORR was 40% with a median duration of 5.9 months. The cholangiocarcinoma ORR of 36.8% is consistent with the pattern observed across tumor types in this molecular subset, further supporting the NRG1 fusion as a clinically actionable driver across histologies.
| Why small basket trial cohorts are acceptable for molecular-rare cancers The FDA’s framework for tumor-agnostic and rare molecular alteration approvals recognizes that conventional large randomized trial design is not feasible when the target population may number in the hundreds rather than thousands. The standard applied is whether the evidence is clinically meaningful and sufficiently robust to support a reliable benefit-risk assessment. For Bizengri in NRG1+ cholangiocarcinoma, the 36.8% ORR from a prospectively conducted, centrally reviewed cohort in a registrational basket trial, in a disease with no approved targeted therapy and historically poor response to chemotherapy, meets this standard. The approval was also supported by the mechanistic coherence of responses across three tumor types in the same trial, which substantially strengthens the interpretation of the cholangiocarcinoma cohort data. |
|---|
Safety
The safety profile of zenocutuzumab in the cholangiocarcinoma cohort was consistent with its established profile across other NRG1+ tumor types in eNRGy.
Common adverse reactions (consistent with class and mechanism): infusion-related reactions, fatigue, nausea, diarrhea, musculoskeletal pain, decreased appetite.
Serious adverse reactions: Serious infusion-related reactions can occur and require premedication per the prescribing information and monitoring during each infusion.
Left ventricular dysfunction: HER2-targeting antibodies carry a class risk of cardiotoxicity including left ventricular dysfunction and decreased ejection fraction. Monitor cardiac function per prescribing information. Patients with pre-existing significant cardiac disease require careful evaluation before initiating treatment.
Embryo-fetal toxicity: Zenocutuzumab targets HER2 and HER3, growth factor receptors that play roles in fetal development. Females of reproductive potential should use effective contraception during treatment and for 7 months after the last dose. Males should use effective contraception during treatment and for 4 months after the last dose.
For the complete adverse event profile and dose modification guidance, the full prescribing information should be reviewed before initiating treatment.
Dosing and Administration
| Parameter | Details |
|---|---|
| Dose | 750 mg intravenous infusion |
| Schedule | Every 2 weeks (14-day cycle) |
| Premedication | Per prescribing information before each infusion |
| Setting | Healthcare facility capable of managing infusion reactions |
| Continue until | Disease progression or unacceptable toxicity |
The CNPV Connection: How the Approval Was Expedited
The Bizengri cholangiocarcinoma approval used the Commissioner’s National Priority Voucher (CNPV) program for the first time in an oncology/rare cancer setting. The CNPV was awarded to Partner Therapeutics on May 6, 2026, and the FDA approved the cholangiocarcinoma indication just two days later on May 8, 2026. The CNPV compressed the standard review timeline by applying priority review resources immediately, accelerating access to a therapy for a population with urgent unmet need.
The CNPV’s use in NRG1+ cholangiocarcinoma reflects the FDA’s recognition that rare molecular subsets of aggressive cancers can represent conditions of national health significance warranting the same acceleration tools applied to other priority public health areas.
What This Means for Patients and Clinicians
For patients with cholangiocarcinoma
If you have been diagnosed with cholangiocarcinoma and your tumor has not yet been tested for NRG1 fusions, this approval is a reason to discuss molecular testing with your oncologist. NRG1 fusions are rare in this cancer type, but they are actionable: if present, Bizengri is now an FDA-authorized option after disease progression on prior systemic therapy.
Comprehensive molecular testing platforms that include RNA-based fusion detection are available at major academic centers and through commercial laboratory services. Testing requirements and ordering should be discussed with your oncologist.
For oncologists managing cholangiocarcinoma
The approval of zenocutuzumab completes a third actionable molecular subset for cholangiocarcinoma (alongside FGFR2 fusions, IDH1 mutations, and HER2 amplification/overexpression). Comprehensive molecular profiling including RNA-based sequencing at the time of diagnosis or upon progression is increasingly essential for identifying all available targeted options.
For patients whose NRG1 fusion status has not been determined, RNA sequencing should be requested specifically if standard next-generation sequencing panels are DNA-only. NRG1 fusions may be underdetected in DNA-based panels due to their intronic structure.
Clinical trial opportunities
Additional clinical development of zenocutuzumab in earlier lines and in combination regimens is ongoing. ClinicalTrials.gov and ClinicalTrials.gov for zenocutuzumab broadly list currently enrolling studies for patients interested in investigational options.
The Cholangiocarcinoma Foundation is the leading U.S. patient advocacy organization for bile duct cancer and maintains current information on approved therapies, clinical trials, and specialist referral resources. The American Liver Foundation and NCI cholangiocarcinoma information provide clinical and research overviews.
For related HED coverage of other molecularly targeted oncology approvals, see our post on Lifyorli (relacorilant) and the novel cortisol-resistance mechanism in platinum-resistant ovarian cancer and our post on Datroway (datopotamab deruxtecan) achieving its third approved indication in triple-negative breast cancer.
Sources
FDA approval announcement: FDA approves zenocutuzumab-zbco for advanced, unresectable or metastatic cholangiocarcinoma. FDA.gov. May 8, 2026.
Partner Therapeutics press release: Partner Therapeutics Announces FDA Approval of BIZENGRI (zenocutuzumab-zbco) for NRG1 Fusion-Positive Cholangiocarcinoma Following Receipt of FDA Commissioner’s National Priority Voucher. partnertx.com. May 11, 2026.
CNPV award press release: Partner Therapeutics Announces Receipt of FDA Commissioner’s National Priority Voucher for Bizengri in NRG1 Fusion-Positive Cholangiocarcinoma. drugs.com. May 6, 2026.
CancerNetwork clinical coverage: FDA Approves Zenocutuzumab in NRG1+ Cholangiocarcinoma Post Systemic Therapy. cancernetwork.com. May 2026.
Targeted Oncology clinical coverage: FDA Approves Zenocutuzumab for NRG1 Fusion-Positive Cholangiocarcinoma. targetedonc.com. May 2026.
PharmExec approval coverage: FDA Approves Bizengri for Adults with NRG1 Fusion-Positive Cholangiocarcinoma. pharmexec.com. May 2026.
ONS clinical summary: FDA Approves Zenocutuzumab-Zbco for Advanced, Unresectable, or Metastatic Cholangiocarcinoma. ons.org. May 2026.
eNRGy trial registration: NCT02912949. ClinicalTrials.gov.
Bizengri original FDA approval (NSCLC/pancreas, December 2024): FDA approves zenocutuzumab-zbco for non-small cell lung cancer and pancreatic adenocarcinoma. FDA.gov. December 2024.
AACR/NCI/EORTC 2025 CCA presentation: Schram AM, Cleary JM, Arnold D, et al. Zenocutuzumab efficacy and safety in advanced NRG1+ cholangiocarcinoma: analysis from the phase 2 eNRGy trial. Presented at AACR/NCI/EORTC Conference, October 2025, Boston.
NRG1 and HER signaling review: NRG1-HER3 signaling in cancer. PMC7297124.
Zenocutuzumab mechanism: Bispecific antibodies targeting HER2/HER3. PMC9891442.
NRG1 gene: NRG1 gene. NCBI.
Cholangiocarcinoma overview: Bile Duct Cancer. American Cancer Society.
FDA tumor-agnostic drug approvals: Tumor Agnostic Approvals. FDA.gov.
CNPV program: Commissioner’s National Priority Voucher. FDA.gov.
Breakthrough Therapy Designation: Breakthrough Therapy. FDA.gov.
Orphan Drug Designation: Designating an Orphan Product. FDA.gov.
Patient resources: Cholangiocarcinoma Foundation | American Liver Foundation: Bile Duct Cancer | NCI Cholangiocarcinoma | ClinicalTrials.gov: zenocutuzumab
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Treatment decisions for cholangiocarcinoma, including molecular testing decisions and therapy selection, should be made in consultation with a qualified oncologist experienced in biliary tract malignancies. Molecular testing for NRG1 fusions requires appropriate RNA-based sequencing; consult your oncologist about which testing platform is appropriate. |
|---|