
✅ Updated May 26, 2026: FDA Approval Confirmed On May 22, 2026, the FDA approved Datroway (datopotamab deruxtecan-dlnk, AstraZeneca/Daiichi Sankyo) for adults with unresectable or metastatic triple-negative breast cancer (TNBC) who are not candidates for PD-1/PD-L1 inhibitor therapy. This is the first TROP2-directed ADC approved in this setting and the first targeted therapy to demonstrate a statistically significant overall survival advantage over chemotherapy in first-line immunotherapy-ineligible metastatic TNBC. Important regulatory note: this indication was approved under accelerated approval based on objective response rate (63% vs. 29%) and duration of response (12.3 vs. 7.1 months) as the regulatory basis. Continued approval for this indication may be contingent upon verification and description of clinical benefit in the confirmatory trial. The PFS and OS data from TROPION-Breast02 (detailed below) provide the broader efficacy context but are not the formal basis of this particular approval. NCCN update: Following the approval, Datroway was added to the NCCN Clinical Practice Guidelines as a Category 1 preferred first-line treatment option for metastatic TNBC patients who are not candidates for immunotherapy. Global status: As of May 22, 2026, regulatory reviews are ongoing in the EU, China, Japan, Australia, Canada, Singapore, and Switzerland. Datroway’s full approved indication list now includes: HR-positive, HER2-negative metastatic breast cancer (approved January 2025); EGFR-mutated NSCLC after prior EGFR-directed therapy and platinum chemotherapy (accelerated approval); and metastatic TNBC ineligible for PD-1/PD-L1 inhibitor therapy (approved May 22, 2026, accelerated approval).
Triple-negative breast cancer is defined by what it lacks: no estrogen receptor, no progesterone receptor, no HER2 amplification. Those absences mean that the targeted therapies which have transformed outcomes in other breast cancer subtypes do not apply here. For decades, chemotherapy was the only systemic option. Then, in 2020, immunotherapy arrived for patients whose tumors expressed the PD-L1 protein. A meaningful advance for those patients. But not everyone qualifies.
Patients with metastatic TNBC who are ineligible for immunotherapy have historically had the fewest options and the worst outcomes of any breast cancer population. Their first-line treatment has remained standard cytotoxic chemotherapy, with all the toxicity that entails and a median overall survival below two years.
Datopotamab deruxtecan (Dato-DXd, brand name Datroway) is now seeking to change that. Developed by AstraZeneca and Daiichi Sankyo, the drug already received FDA approval in January 2025 for a different breast cancer subtype (HR-positive, HER2-negative). Now it has Priority Review for a new indication: first-line treatment of metastatic TNBC in patients who are not candidates for immunotherapy. The PDUFA date falls in Q2 2026. The Phase 3 TROPION-Breast02 trial, published in the Annals of Oncology in April 2026, produced results that oncologists are calling a potential new standard of care.
Triple-Negative Breast Cancer: The Biology, the Burden, and the Disparities
Triple-negative breast cancer accounts for approximately 15% of all breast cancer diagnoses in the United States, roughly 35,000 new cases per year. Despite representing a minority of breast cancer cases, it accounts for a disproportionate share of breast cancer deaths because of its aggressive biology, its relative resistance to treatment, and its tendency to be diagnosed at younger ages and at more advanced stages.
The racial disparities in TNBC are well documented and clinically significant. Black women are diagnosed with TNBC at roughly twice the rate of white women. They are more likely to be diagnosed at younger ages and more advanced stages. And despite these higher incidence rates, access to specialist oncology care and novel therapies has historically been unequal. Any advance in TNBC outcomes is therefore not just an oncologic milestone but a health equity issue.
| Who is ineligible for immunotherapy in TNBC, and why this population matters Since 2020 and 2021, PD-L1 checkpoint inhibitors (atezolizumab and then pembrolizumab) have been approved as first-line options for metastatic TNBC. Pembrolizumab with chemotherapy is now the standard of care for PD-L1-positive metastatic TNBC, and it produces a meaningful survival benefit in that population. However, PD-L1 positivity is not universal in TNBC. Depending on the assay and scoring method used, approximately 40 to 60 percent of metastatic TNBC patients have PD-L1-positive tumors. The remainder, along with patients who cannot receive immunotherapy due to autoimmune disease, organ transplant status, or other contraindications, fall into the immunotherapy-ineligible category. TROPION-Breast02 enrolled specifically and exclusively these patients. This is the population for which first-line treatment has remained unchanged at standard chemotherapy for decades, and the population for which Dato-DXd is seeking approval. |
What Is Dato-DXd and How Does It Work?
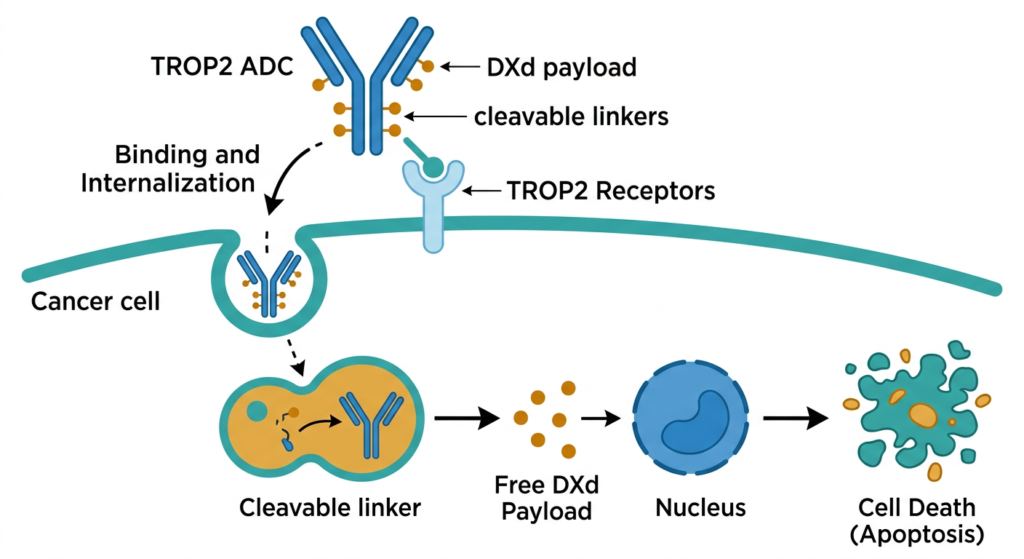
Datopotamab deruxtecan is an antibody-drug conjugate, part of the same drug class as trastuzumab deruxtecan (Enhertu/T-DXd) and sacituzumab govitecan (Trodelvy). All ADCs share the same general architecture: an antibody that recognizes a target protein on cancer cell surfaces, linked to a chemotherapy payload. The antibody finds the cancer cell, binds to it, is internalized, and releases the payload inside the cell.
Dato-DXd’s target is TROP2 (trophoblast cell-surface antigen 2), a protein expressed at high levels on the surface of many solid tumors, including the majority of TNBC tumors. The payload is DXd, a topoisomerase I inhibitor derived from exatecan. When the ADC is internalized into TROP2-expressing tumor cells, the linker is cleaved and DXd is released inside the cell, interfering with DNA replication and causing cancer cell death.
The linker technology is an important distinguishing feature. The cleavable tetrapeptide-based linker used in Dato-DXd is designed to be stable in the bloodstream but cleaved efficiently inside cells. This stability reduces off-target payload release in circulation, which contributes to a lower rate of hematologic toxicity compared to some earlier ADC platforms. The same DXd payload and linker technology is used in T-DXd (Enhertu), which explains the shared class safety signal of interstitial lung disease and stomatitis across both drugs.
| Dato-DXd versus sacituzumab govitecan (Trodelvy): both target TROP2, but differently Sacituzumab govitecan (Trodelvy) is the other FDA-approved TROP2-directed ADC in breast cancer. It is approved for previously treated metastatic TNBC and for HR-positive HER2-negative metastatic breast cancer. Both it and Dato-DXd target TROP2, but they use different antibodies, different payloads (SN-38 for sacituzumab vs. DXd for datopotamab), and different linker technologies. The practical difference shows up in the safety profile: sacituzumab govitecan has higher rates of hematologic toxicity (neutropenia, diarrhea) while Dato-DXd’s signature toxicities are stomatitis and ocular surface events. Neither has been compared head-to-head in TNBC. They occupy different approved settings, and the question of how to sequence them in the metastatic TNBC treatment landscape is one the field will need to work out as approvals evolve. The panel discussion at OncLive noted that differences in linker technology and payload between the two drugs may influence clinical outcomes, but no definitive comparative data exists. Clinicians should be familiar with both safety profiles to counsel patients appropriately. |
TROPION-Breast02: Design and Full Results
Trial design
TROPION-Breast02 (NCT05374512) was a randomized, open-label, international Phase 3 trial conducted across multiple countries. Between May 2022 and June 2024, 644 patients with previously untreated, locally recurrent inoperable or metastatic TNBC who were not candidates for PD-1/PD-L1 inhibitors were randomized 1:1 to Dato-DXd (6 mg/kg intravenously every 3 weeks, n=323) or investigator’s choice of chemotherapy (ICC, n=321). ICC options included paclitaxel, nab-paclitaxel, carboplatin, capecitabine, or eribulin mesylate. Randomization was stratified by geographic region, disease-free interval, and PD-L1 status.
The trial had dual primary endpoints: progression-free survival by blinded independent central review (BICR) per RECIST 1.1, and overall survival. Both primary endpoints were required to demonstrate statistical significance for the trial to be considered successful. Achieving both is a notable distinction in a disease setting where OS data is often immature at the time of initial analysis.
Efficacy results
| Efficacy endpoint | Dato-DXd (n=323) | Chemotherapy (n=321) |
| Median PFS (BICR) | 10.8 months (95% CI 8.6–13.0) | 5.6 months (95% CI 5.0–7.0) |
| PFS hazard ratio | 0.57 (95% CI 0.47–0.69; p<0.0001) | Reference |
| Risk reduction in progression/death | 43% | Reference |
| 12-month PFS rate | 45.6% | 25.6% |
| 18-month PFS rate | 32.7% | 16.8% |
| Median OS | 23.7 months | 18.7 months |
| OS hazard ratio | 0.79 (21% reduction in risk of death; p<0.05) | Reference |
| Median treatment duration | 6.7 months | 4.1 months |
| Patients on treatment at data cutoff | Longer than chemo arm | Shorter duration |
The PFS result is the most striking number: 10.8 versus 5.6 months is a near doubling of the time to disease progression or death. The 12-month PFS rates tell a related story: at one year, 45.6% of patients on Dato-DXd were progression-free, compared to 25.6% on chemotherapy. At 18 months, those rates were 32.7% versus 16.8%.
The OS result of 23.7 versus 18.7 months represents approximately five additional months of survival, with a statistically significant hazard ratio of 0.79. Having both PFS and OS meet statistical significance in the same trial is an important finding. Many oncology trials achieve PFS endpoints but fail to translate that into an OS benefit, sometimes because subsequent therapies after disease progression equalize outcomes across arms. TROPION-Breast02 demonstrated both.
The 6.7 versus 4.1 month median treatment duration favoring Dato-DXd is an indirect measure of tolerability: patients stayed on the experimental treatment longer, suggesting the drug was manageable enough to continue. That observation is supported by the safety data.
For patients with ER-positive disease, a separate PROTAC-based therapy is simultaneously under FDA review. Read about it here.
Safety: A Different Toxicity Profile Than Chemotherapy
Dato-DXd does not look like chemotherapy in its safety profile. Where chemotherapy predominantly causes hematologic toxicity (neutropenia, anemia, febrile neutropenia), Dato-DXd’s characteristic adverse effects are mucosal (stomatitis) and ocular. This difference matters for patient counseling and clinical management.
| Safety metric | Dato-DXd | Chemotherapy (ICC) |
| Any treatment-related adverse event | 93% | 83% |
| Grade 3 or higher TRAEs | 33% | 29% |
| Serious treatment-related AEs | 9% | 8% |
| Discontinuation due to TRAEs | 4% | 7% |
| Treatment-related deaths | 0 | 0 |
| Stomatitis (all grade) | 57% | Lower |
| Nausea (all grade) | 45% | Lower |
| Alopecia (all grade) | 41% | 21% |
| Ocular surface events (grade 1, dry eye/keratitis) | 24% | 3% |
| ILD/pneumonitis (drug-related, adjudicated) | Less than 1% | Less than 1% |
| Hematologic toxicity (neutropenia, anemia) | Lower than chemo arm | Predominant toxicity |
Several aspects of this safety data are worth emphasizing for clinical context. First, discontinuation due to treatment-related adverse events was actually lower with Dato-DXd (4%) than with chemotherapy (7%). This means patients on the experimental arm were less likely to stop treatment because of toxicity despite the higher overall rate of any adverse event. The profile is different, not simply worse.
Second, stomatitis at 57% is high in absolute terms but predominantly low-grade. The OncLive panel reviewing these results noted that proactive oral care management, including steroid-based mouthwash protocols (expanded from the SWISH trial experience with everolimus), can substantially reduce the incidence and severity of high-grade stomatitis. Institutions implementing Dato-DXd will need nursing education focused on stomatitis prevention and grading.
Third, ocular surface events (dry eye, keratitis) at 24% are almost entirely grade 1 and manageable with lubricating eye drops and ophthalmologic monitoring. The ILD rate of less than 1% is consistent with the known Dato-DXd class signal, lower than what is seen with T-DXd at current doses. ILD monitoring, prompt evaluation of respiratory symptoms, and early intervention with corticosteroids for confirmed cases remain important clinical requirements.
Context: How This Fits Into the TNBC Treatment Landscape
If approved, Dato-DXd would become the first non-chemotherapy, non-immunotherapy first-line option for metastatic TNBC patients who cannot receive checkpoint inhibitors. The treatment landscape for this population would shift in two meaningful ways.
First, the starting line for subsequent treatment sequencing changes. Patients who progress on first-line Dato-DXd will have had an ADC with a specific toxicity profile and resistance pattern. How sacituzumab govitecan (Trodelvy), currently approved in previously treated metastatic TNBC, performs after Dato-DXd progression is not established. This sequencing question will drive post-approval research.
Second, the ADC revolution in breast cancer treatment is now reaching the TNBC immunotherapy-ineligible population specifically. T-DXd reshaped HER2-positive and HER2-low metastatic breast cancer. Sacituzumab govitecan improved outcomes in previously treated TNBC. Dato-DXd, if approved, would extend ADC-based first-line treatment into a subgroup previously limited to cytotoxic chemotherapy.
| What the TROPION-Breast01 trial (HR+/HER2- breast cancer) can teach us here Dato-DXd’s January 2025 FDA approval for HR-positive, HER2-negative metastatic breast cancer came from the TROPION-Breast01 trial. That trial met its primary PFS endpoint but did not achieve statistical significance on OS. The explanation offered by investigators was that subsequent ADC treatment in the control arm after disease progression may have equalized survival outcomes. TROPION-Breast02 in TNBC is different in a clinically important way: it achieved statistical significance on both PFS and OS. This distinction matters for the regulatory submission and for clinician confidence. When a trial achieves the survival endpoint and not just the surrogate, the benefit-risk assessment is on firmer ground. The difference in OS outcomes between the two trials also highlights how patient population and available subsequent therapies shape survival data. TNBC patients in TROPION-Breast02 had fewer subsequent treatment options after progression compared to HR+ patients, which may have allowed the OS benefit to emerge more clearly in this trial. |
What to Discuss With Your Oncologist Now
What This Approval Means for Patients With Immunotherapy-Ineligible Metastatic TNBC
Datroway is now FDA-approved and available for this population
Datroway (datopotamab deruxtecan-dlnk) is now an FDA-approved first-line option for adults with unresectable or metastatic TNBC who are not candidates for PD-1/PD-L1 inhibitor therapy. It is the first and only targeted therapy approved in this setting and the first to demonstrate a statistically significant OS advantage over chemotherapy in this population.
NCCN guidelines have been updated following the approval: Datroway is now listed as a Category 1 preferred first-line treatment option for immunotherapy-ineligible metastatic TNBC. Oncologists at NCCN member institutions will begin prescribing based on this recommendation immediately.
Understanding the accelerated approval pathway
The FDA approved the TNBC indication under accelerated approval, using objective response rate (ORR) and duration of response as the regulatory endpoints. The ORR with Datroway was 63% versus 29% with chemotherapy, and median duration of response was 12.3 versus 7.1 months. These are the formal bases for the approval.
This is important context for patients and clinicians. Accelerated approval means the FDA determined that the ORR and duration of response data were sufficiently compelling to authorize use now, while a confirmatory trial verifies long-term clinical benefit. The PFS (10.8 vs. 5.6 months) and OS (23.7 vs. 18.7 months) data from TROPION-Breast02 strongly support the treatment’s value but are not the formal regulatory basis for this approval.
Continued approval may be contingent upon the outcome of the confirmatory trial. This does not mean the drug will be removed from the market; it means AstraZeneca and Daiichi Sankyo must verify the clinical benefit findings as the follow-up matures.
What to discuss with your oncologist now
- Has your tumor been tested for PD-L1 expression? If your tumor is PD-L1 positive and you have no contraindications to immunotherapy, pembrolizumab plus chemotherapy remains the approved standard of care.
- If you are not a PD-1/PD-L1 candidate, Datroway is now an FDA-authorized first-line option you can discuss with your oncologist as an alternative to standard cytotoxic chemotherapy.
- Ask about stomatitis prevention protocols and ocular monitoring, which are the key toxicity management considerations with Datroway.
- Ask whether your oncology center has experience with Datroway from the TROPION-Breast02 trial enrollment or from the HR+/HER2- TNBC approval earlier in 2025.
- If you are enrolled in or considering a clinical trial involving Datroway, discuss how this approval affects your options with your treating oncologist.
Global availability
For patients outside the United States: Datroway has not yet been approved by the EMA, Health Canada, PMDA (Japan), or TGA (Australia) for the TNBC indication. Regulatory submissions are under review in multiple markets. Check the most current status with your oncologist or the national regulatory authority in your country.
For patients and families navigating a TNBC diagnosis, the Triple Negative Breast Cancer Foundation, Susan G. Komen, and the National Cancer Institute Cancer Center directory continue to be the best starting points for treatment resources, clinical trial information, and support programs.
Sources
OncLive Phase 3 results: TROPION-Breast02 Data Support Dato-DXd as New First-Line SOC in Triple-Negative Breast Cancer. OncLive. April 2026.
OncLive Priority Review: FDA Grants Priority Review to Frontline Dato-DXd for Metastatic TNBC Ineligible for Immunotherapy. OncLive. 2026.
OncLive panel discussion: Findings for Frontline Dato-DXd From TROPION-Breast02 in Immunotherapy-Ineligible TNBC. OncLive. May 2026.
OncoDaily safety summary: Datopotamab Deruxtecan Improves PFS and OS in First-Line Advanced TNBC in TROPION-Breast02. OncoDaily. April 2026.
Cancer Nursing Today: Datopotamab Deruxtecan Expands First-Line Treatment Options in Metastatic TNBC. May 2026.
CancerNetwork overview: How Dato-DXd and the TROPION Trials Are Transforming Solid Tumor Research. CancerNetwork. May 2026.
AstraZeneca Priority Review announcement: DATROWAY granted Priority Review in the US as 1st-line treatment for patients with metastatic TNBC who are not candidates for immunotherapy. AstraZeneca. 2026.
TROPION-Breast01 context: FDA approves datopotamab deruxtecan for HR+/HER2- breast cancer. FDA.gov. January 2025.
Patient resources: NCI Cancer Center directory | Susan G. Komen | TNBC Foundation
FDA approval announcement: FDA approves datopotamab deruxtecan-dlnk for unresectable or metastatic triple-negative breast cancer. FDA.gov. May 22, 2026.
AstraZeneca/Daiichi Sankyo press release: DATROWAY approved in the US as first TROP2-directed ADC for 1st-line treatment of patients with metastatic TNBC. businesswire.com. May 22, 2026.
PharmExec approval coverage: FDA Approves Datroway for Patients with Metastatic Triple-Negative Breast Cancer Who Are Not PD-1/PD-L1 Inhibitor Candidates. pharmexec.com. May 2026.
AJMC approval coverage: Datopotamab Deruxtecan Wins First-Line FDA Approval for Immunotherapy-Ineligible Triple-Negative Breast Cancer. ajmc.com. May 2026.
Healio approval coverage: Datroway nabs FDA approval for immunotherapy-ineligible triple-negative breast cancer. healio.com. May 2026.
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice. The TNBC indication for Datroway was approved under accelerated approval; continued approval may be contingent upon confirmatory trial results. Treatment decisions for metastatic TNBC should be made in close consultation with a qualified oncologist who can account for your individual diagnosis, treatment history, and tumor biology. |
|---|
Leave a Reply