| 📌 The essentials On April 24, 2026, following an Executive Order signed by President Trump on April 18, the FDA announced a series of regulatory actions to accelerate development of psychedelic-based medicines for serious mental illness. Four distinct actions: (1) Three Commissioner’s National Priority Vouchers (CNPVs) issued to Compass Pathways (psilocybin/TRD), Usona Institute (psilocybin/MDD), and Transcend Therapeutics/Otsuka (methylone/PTSD). (2) The first U.S. clinical study of an ibogaine derivative (noribogaine, DemeRx NB) cleared to proceed. (3) Final guidance issued on clinical trial design for serotonin-2A agonists. (4) The overarching political context of an executive order directing HHS to accelerate access to treatments for depression, PTSD, and substance use disorders. None of these drugs are currently FDA-approved. This post focuses on what the clinical evidence actually shows for each program, where legitimate scientific promise lies, and what questions remain genuinely open. |
|---|
Treatment-resistant depression affects an estimated 30% of people with major depressive disorder, roughly 100 million people globally who have tried multiple medications without adequate relief. PTSD affects 13 million Americans, and fewer than half respond adequately to available first-line treatments. These are large populations with severe unmet need, and they have been waiting for something meaningfully better for a long time.
On April 24, 2026, the FDA announced a series of regulatory actions to accelerate the development of psychedelic-based medicines, specifically serotonin-2A agonists and related compounds, for serious mental illness. Three companies received Commissioner’s National Priority Vouchers (CNPVs). An early-phase clinical study of a derivative of ibogaine was cleared to proceed. And final guidance on how to design clinical trials for this drug class was issued.
These actions followed an Executive Order signed by President Trump on April 18, directing HHS to accelerate access to treatments for serious mental illness, with explicit mention of psychedelic therapies and veterans. The political context is real and worth acknowledging, but it does not determine whether the underlying science is sound. This post focuses on what the evidence actually shows for each program, where the genuine clinical promise lies, and what legitimate scientific questions remain open.
What the FDA Actually Did on April 24
There are four distinct actions in the April 24 announcement, and they are not all equal in regulatory significance:
| Action | What it means | What it does not mean |
|---|---|---|
| 3 CNPVs issued (Compass, Usona, Transcend/Otsuka) | FDA review compressed to approximately 1 to 2 months after NDA submission, versus the standard 10 to 12 months | Not an approval; not an efficacy endorsement. The NDA must still be submitted and reviewed. |
| Noribogaine IND cleared (DemeRx NB) | First-ever U.S. clinical study of an ibogaine derivative can proceed. Phase 1 only. | The drug is not approved. Phase 1 tests safety and dosing in a small controlled sample. |
| Final guidance issued on serotonin-2A agonist trial design | Sponsors now have a definitive FDA framework for how to design psychedelic drug trials, addressing the unique scientific challenges of blinding and endpoints. | Does not lower the bar for evidence; specifies what is needed. |
| Executive Order context | Signals political priority and may increase resource allocation and FDA engagement speed | Does not change the legal standard for approval: substantial evidence of safety and efficacy |
| What is a Commissioner’s National Priority Voucher (CNPV)? The CNPV program was launched in 2025 as a way to compress the FDA review timeline for drugs designated as national health priorities. A CNPV compresses the FDA’s review to approximately 1 to 2 months from NDA submission, compared to the standard 10 to 12 months. Earlier in 2026, CNPVs were used to approve Foundayo (orforglipron, oral GLP-1 for obesity) in 50 days and Wegovy HD in 54 days. For psychedelic drugs, a CNPV does not mean the FDA has pre-approved the drug or concluded it works. It means the FDA will prioritize and accelerate its review once a complete application is submitted. The drugs still need to demonstrate substantial evidence of safety and efficacy through their NDA package. A company that submits an NDA and receives a CNPV could still receive a Complete Response Letter if the evidence is insufficient, as happened with MDMA/Lykos, which did not have a CNPV but illustrates the principle. |
|---|
COMP360 (Compass Pathways): Two Phase 3 Trials, Both Positive
Of the three CNPV recipients, Compass Pathways has by far the most mature clinical evidence package. COMP360 is a synthetic, proprietary formulation of psilocybin, the active compound in psychoactive mushrooms, being developed for treatment-resistant depression (TRD), defined as inadequate response to at least two adequate courses of antidepressant therapy.
Compass has completed the primary endpoints of both Phase 3 trials in this program, and both are positive:
| Trial | Design | Primary endpoint result |
|---|---|---|
| COMP005 | Randomized, double-blind; single 25 mg dose vs. placebo; approximately 568 patients; North America and Europe | MADRS score difference at week 6: 3.6 points versus placebo (p less than 0.001). Highly statistically significant and clinically meaningful. |
| COMP006 | Randomized, double-blind; two fixed doses (3 weeks apart) of 25 mg vs. 1 mg; approximately 568 patients | MADRS difference between 25 mg and 1 mg at week 6: 3.8 points (p less than 0.001). Durable effects; 26-week data expected Q3 2026. |
The MADRS (Montgomery-Asberg Depression Rating Scale) is the most widely used validated scale for measuring depression severity in clinical trials. A difference of 3.6 to 3.8 points is considered clinically meaningful, particularly in a treatment-resistant population where previous antidepressants have failed. Across two robust Phase 3 trials involving more than 1,000 participants combined, COMP360 produced consistent, highly statistically significant results at the primary endpoint, a result that is notable in a population where proving benefit has historically been challenging.
Critically, the Data Safety Monitoring Board for the program reported no evidence of a clinically meaningful imbalance in suicidality between treatment and placebo arms in either COMP005 or COMP006, a reassuring finding for a drug used in a depressed population with elevated baseline suicide risk. The most common adverse events were headache, nausea, and visual hallucinations, the large majority occurring on the day of administration and resolving within 24 hours.
Compass has indicated it plans to submit an NDA to the FDA in Q4 2026. With a CNPV in hand, review could potentially be completed in early 2027.
Usona Institute: Psilocybin for Major Depressive Disorder
The Usona Institute is a Wisconsin-based nonprofit developing PSIL201, a psilocybin formulation for major depressive disorder (MDD) rather than treatment-resistant depression. The distinction matters: MDD is a broader population that includes patients for whom first-line antidepressants may have provided partial or inadequate response but who do not meet the stricter TRD definition.
Usona’s program received FDA Breakthrough Therapy designation in 2019, one of the earliest such designations for a psychedelic drug. It is currently in Phase 3. Phase 2 trial data showed rapid, sustained reductions in depressive symptoms in many participants, with benefits persisting at six months after a single session, a durability profile notably different from daily antidepressants, which require continuous dosing.
As a nonprofit, Usona’s structure is oriented around access and affordability rather than investor return. The CNPV accelerates its path to FDA review once Phase 3 data is complete.
Transcend Therapeutics / Otsuka: Methylone for PTSD
The third CNPV went to TSND-201, a methylone-based treatment for PTSD being developed by Transcend Therapeutics and in the process of being acquired by Otsuka. This is the most scientifically interesting and the most clinically immature of the three programs.
Methylone is a synthetic entactogen, a compound that produces empathogenic and prosocial effects, structurally related to MDMA but with a different pharmacological profile. It targets similar receptor systems (serotonin, dopamine, norepinephrine) but is thought to have reduced cardiovascular effects and a somewhat shorter duration of action than MDMA. Transcend received FDA Breakthrough Therapy designation for TSND-201 in July 2025.
TSND-201 met its primary endpoint in a Phase 2 study, showing significant improvement on the Clinician-Administered PTSD Scale (CAPS-5) compared to placebo, the same validated scale used in the MDMA/Lykos trials. The program is now entering Phase 3. A CNPV for a Phase 3-stage program is less immediately actionable than for a program preparing an NDA, but it signals FDA’s willingness to prioritize the review once Phase 3 data is available.
| Why methylone and not MDMA? The Lykos rejection context The MDMA/PTSD story is the essential backdrop for understanding why methylone is receiving attention. Lykos Therapeutics spent years developing MDMA-assisted therapy for PTSD and submitted an NDA with Phase 3 data showing 71% of patients no longer met PTSD criteria after treatment (versus roughly 48% on placebo). The FDA rejected it in August 2024 and issued a Complete Response Letter. The FDA’s concerns with the Lykos application were multiple: questions about functional unblinding (MDMA’s subjective effects make it nearly impossible for patients to not know whether they received drug or placebo, potentially inflating self-reported outcomes); concerns about trial conduct integrity; and questions about the standardization of the psychotherapy component. An FDA advisory committee voted 10 to 1 that the benefits did not outweigh the risks. A retraction of several early Lykos trial papers compounded the credibility issues. Methylone enters this space as a structurally related compound that may offer similar therapeutic mechanisms with potentially cleaner trial methodology, if the blinding and conduct issues that plagued MDMA development can be avoided. The final guidance issued April 24 specifically addresses these challenges for the entire class. |
|---|
Noribogaine: The First Ibogaine Derivative to Enter U.S. Clinical Trials
The most novel regulatory action in the April 24 announcement is the IND clearance for DemeRx NB to begin a Phase 1 clinical study of noribogaine hydrochloride for alcohol use disorder. The FDA described it as the first instance in which the agency has allowed a clinical study of a derivative of ibogaine in the United States.
What is ibogaine, and why the interest?
Ibogaine is a psychoactive alkaloid derived from the root bark of the Tabernanthe iboga shrub, native to West Central Africa. It has been used in ceremonial contexts by the Bwiti tradition for generations and has been studied for its potential to interrupt addiction, particularly opioid and alcohol dependence, through a mechanism quite different from psilocybin or MDMA. Ibogaine appears to act on multiple receptor systems simultaneously, including opioid receptors, NMDA receptors, serotonin transporters, and sigma receptors, and produces a prolonged, intense visionary experience often described as a life review.
The clinical interest in ibogaine for addiction is supported by observational data and case reports suggesting dramatic reductions in opioid withdrawal symptoms and prolonged periods of abstinence after a single treatment. Researchers at Stanford and elsewhere have documented cases of significant improvement in PTSD and traumatic brain injury symptoms following ibogaine treatment in settings outside the United States where it is legal.
Why noribogaine rather than ibogaine itself?
Ibogaine carries a serious safety concern that has prevented its clinical development in the U.S.: cardiac arrhythmia. Ibogaine blocks cardiac potassium channels (hERG), prolonging the QTc interval and creating a risk of potentially fatal ventricular arrhythmias. Several deaths have been reported in unregulated ibogaine treatment settings, attributed to this cardiac mechanism.
Noribogaine is ibogaine’s primary metabolite, the compound the body converts ibogaine into after administration. It retains many of ibogaine’s pharmacological properties but appears to have a reduced cardiac safety burden based on preclinical and early human data. DemeRx NB’s Phase 1 study will evaluate noribogaine’s safety, tolerability, and pharmacokinetics in a closely monitored clinical setting, the foundational data needed before any larger efficacy studies could proceed.
The FDA’s IND clearance is not an endorsement of efficacy. It means the agency has reviewed the preclinical safety package and determined it is adequate to proceed with first-in-human studies under controlled conditions. The noribogaine program is at the very beginning of the clinical development pathway.
The Final Guidance: Why Trial Design Is the Central Scientific Challenge
The fourth action, the issuance of final guidance on designing clinical trials for serotonin-2A agonists, is arguably the most durable of the four. It addresses the core methodological challenges that have haunted psychedelic clinical research for decades and that contributed directly to the Lykos rejection.
Psychedelic drugs create unique clinical trial design problems that do not apply to conventional pharmaceuticals:
Functional unblinding: Psychedelics produce unmistakable subjective effects. Participants almost invariably know whether they received the active drug or placebo, which can inflate self-reported outcomes through expectancy effects and therapeutic relationship dynamics. The guidance addresses this through active placebo comparators, pre-specified blinding assessment, and outcome measure selection.
The psychotherapy component: Most psychedelic treatment protocols pair drug administration with structured psychotherapy sessions, including preparation, dosing, and integration. How to standardize, manualize, and report this component so that an approved therapy is reproducible in clinical practice has been a major regulatory challenge. The guidance provides foundational recommendations.
Session monitoring requirements: These are not drugs you take at home. Administration occurs in monitored clinical settings, often all-day sessions with trained therapists present. The logistics of adequate monitoring, adverse event capture, and patient safety require specific infrastructure specifications.
Outcome measure selection: Traditional depression and PTSD rating scales were not designed to capture the kind of rapid, potentially lasting shifts in symptomatology that psychedelic therapies may produce. The guidance addresses which endpoints are acceptable for demonstrating clinical benefit.
This guidance having moved from draft to final, incorporating public comment, means that sponsors now have a definitive framework rather than interpretable draft recommendations. For companies preparing NDAs, this reduces regulatory uncertainty and should make clinical trial design decisions more defensible.
Reading This Evenhandedly: What This Signals and What It Does Not
The psychedelic medicine space has attracted both credible science and significant hype, and the April 24 announcement has elements of both. An honest assessment requires holding both simultaneously.
What the evidence legitimately supports
The Compass psilocybin program for TRD has now produced two positive Phase 3 trials with consistent, statistically significant, and clinically meaningful results. This is real evidence of a real effect in a population where existing treatments have genuinely failed. The Usona Phase 2 MDD data is encouraging. The DSMB’s finding of no meaningful imbalance in suicidality in either Compass trial is reassuring for the safety profile.
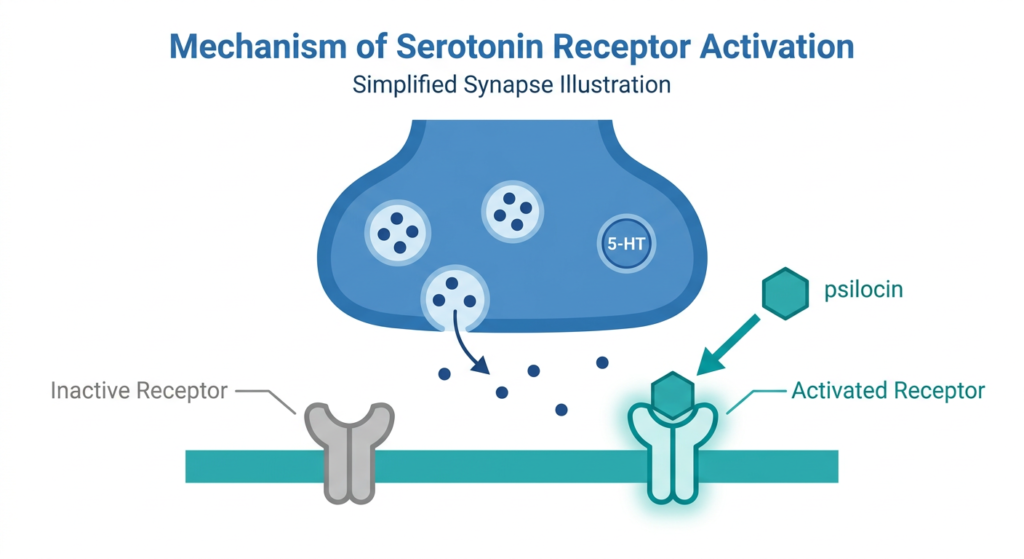
These drugs work through a distinctive mechanism: psilocybin is converted in the body to psilocin, which acts as an agonist at serotonin-2A receptors densely expressed in cortical regions. The result is a temporary but profound disruption of the default mode network, the brain’s self-referential processing hub, which is hyperactive in depression and PTSD. There is a growing body of neuroimaging and mechanistic research supporting this model.
What remains genuinely uncertain
Long-term durability: How long do the benefits last after a 1 to 2 dose treatment? The 26-week COMP006 data, expected Q3 2026, will be the first rigorous window into this question for TRD. Phase 2 psilocybin data has shown benefits at 3 to 6 months; whether this holds at 1 to 2 years is not yet known from controlled trials.
The blinding problem: Functional unblinding remains the most serious methodological challenge for the class. Even with the new guidance, the question of how much of the observed effect is genuine pharmacology versus expectancy and therapeutic relationship is not fully resolved. The 1 mg active comparator dose in the Compass trials is an attempt to address this, but it remains a subject of legitimate scientific debate.
Scalability: Psychedelic-assisted therapy as currently practiced requires significant infrastructure: trained therapists, all-day monitoring sessions, preparation and integration support. How this translates into real-world healthcare delivery, at what cost, and with what fidelity to trial protocols is an open question with major access implications.
The political acceleration: The executive order framing, particularly the emphasis on veterans and ibogaine specifically, reflects lobbying by specific interest groups. Political enthusiasm for a treatment does not validate or invalidate its science, but the concentration of federal attention on specific compounds driven partly by political rather than purely scientific prioritization is worth tracking as the field moves forward.
In the April 24 announcement, FDA Commissioner Marty Makary, MD, MPH stated that as this field moves forward, it is critical that drug development be grounded in sound science and rigorous clinical evidence, describing this standard as what the nation’s veterans and all Americans suffering from these conditions deserve. The standard he named, substantial evidence of safety and efficacy through rigorous clinical trials, is the one against which the approvals that follow will be judged. The CNPV accelerates the clock; it does not change the threshold.
Are you following the psychedelic medicine pipeline as a patient, clinician, or researcher?
The treatment-resistant depression and PTSD populations represent tens of millions of people for whom existing treatments have provided inadequate relief. If the Compass NDA, backed by two positive Phase 3 trials, results in an approved drug in 2027, it will be a genuine clinical advance for a population that has been waiting a long time. The noribogaine program is further out but scientifically interesting. The methylone/PTSD program sits in a space where the need is enormous and the precedent from MDMA’s rejection is recent and instructive.
For patients with treatment-resistant depression or PTSD interested in the clinical trial landscape, ClinicalTrials.gov is the most current source for open enrollment studies. The Multidisciplinary Association for Psychedelic Studies (MAPS) and Compass Pathways both maintain current information on trial availability. For general mental health resources, the National Alliance on Mental Illness (NAMI) and the 988 Suicide and Crisis Lifeline (call or text 988) are available 24 hours a day. We will continue tracking this space as the Compass NDA submission and the COMP006 26-week data approach.
Sources
FDA press announcement: FDA Accelerates Action on Treatments for Serious Mental Illness Following Executive Order. April 24, 2026. fda.gov
Executive Order: White House. Accelerating Medical Treatments for Serious Mental Illness. April 18, 2026. whitehouse.gov
FDA final guidance: Clinical Trials of Serotonin-2A Agonists for the Development of Mental Health-Related Indications: Guidance for Industry. FDA.gov. April 2026.
CNPV recipients: Compass, Usona and Transcend score FDA national priority vouchers amid Trump administration’s psychedelic push. Fierce Biotech. April 2026.
CNN coverage: FDA moves to fast-track review of psilocybin and methylone for mental health. CNN. April 24, 2026.
Psychedelic Alpha: Breaking: FDA Awards Priority Review Vouchers to Otsuka, Compass, and Usona. psychedelicalpha.com. April 24, 2026.
NBC News: FDA grants quick review for 3 psychedelic drug trials. nbcnews.com. April 24, 2026.
COMP005 Phase 3 results: Compass Pathways Successfully Achieves Primary Endpoint in First Phase 3 Trial Evaluating COMP360 Psilocybin for TRD. ir.compasspathways.com. June 23, 2025.
COMP006 Phase 3 results: Compass Pathways Successfully Achieves Primary Endpoint in Second Phase 3 Trial Evaluating COMP360. ir.compasspathways.com. February 17, 2026.
Psychiatric Times: COMP360 Psilocybin for Treatment-Resistant Depression Achieves Primary Endpoint in Phase 3 Trial. psychiatrictimes.com. February 2026.
MDMA/Lykos rejection (NPR): FDA rejects MDMA, disappointing drugmaker Lykos and psychedelics industry. npr.org. August 9, 2024.
Lykos CRL context (STAT News): FDA criticism of MDMA-assisted therapy is an opportunity for psychedelic medicine. STAT News. October 2025.
MAPS statement: MAPS Statement on FDA’s Public Release of Complete Response Letter for MDMA-assisted Therapy. maps.org. September 4, 2025.
Stanford ibogaine study: Ibogaine Treatment Outcomes for Veterans. Stanford Medicine. 2023.
Patient resources and crisis support: NIMH Depression | NIMH PTSD | NAMI | 988 Suicide and Crisis Lifeline | ClinicalTrials.gov: psilocybin depression | MAPS | Compass Pathways
| Disclaimer: Health Evidence Digest provides general information about FDA regulatory updates and health research for educational purposes. This content is not a substitute for professional medical advice. None of the drugs discussed in this post — psilocybin (COMP360, PSIL201), methylone (TSND-201), or noribogaine — are currently FDA-approved treatments. If you are experiencing symptoms of depression, PTSD, or another mental health condition, please consult a qualified healthcare provider. Crisis support is available 24/7 by calling or texting 988. |
|---|
Leave a Reply