| 📌 The essentials On February 10, 2026, the FDA approved pembrolizumab (Keytruda, Merck) in combination with paclitaxel, with or without bevacizumab, for adult patients with platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal carcinoma whose tumors express PD-L1 (combined positive score, or CPS, of at least 1). The approval covers patients who have received one or two prior lines of systemic therapy. This is the first FDA-approved immunotherapy for ovarian cancer in history. The clinical basis: KEYNOTE-B96/ENGOT-ov65 (NCT05116189), a randomized, double-blind, placebo-controlled Phase 3 trial in 643 patients, showed median overall survival of 18.2 months versus 14.0 months with placebo (HR 0.76; p=0.0053) in the PD-L1 CPS of 1 or higher population. The first statistically significant OS benefit ever demonstrated by an immune checkpoint inhibitor in ovarian cancer. A companion diagnostic requirement: Tumor testing with the PD-L1 IHC 22C3 pharmDx assay confirming CPS of 1 or higher is required before treatment. This is a requirement, not a recommendation. |
|---|
Ovarian cancer has resisted immunotherapy for decades. Every major trial of immune checkpoint inhibitors in this disease came back negative or borderline, results that didn’t survive longer follow-up. The field watched other gynecologic cancers, particularly cervical and endometrial, respond to PD-1 blockade while ovarian cancer remained stubbornly outside that story.
That changed on February 10, 2026.
The FDA approved pembrolizumab (Keytruda, Merck) in combination with paclitaxel, with or without bevacizumab, for adult patients with platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal carcinoma whose tumors express PD-L1 (CPS of at least 1). The approval covers patients who have received one or two prior lines of systemic therapy.
It is the first FDA-approved immunotherapy for ovarian cancer in history.
This post covers what platinum resistance means and why it matters, what KEYNOTE-B96 showed across its primary and key secondary endpoints, how to read the survival data carefully, what the companion diagnostic approval means in practice, and what questions are still open.
Platinum Resistance: Why This Setting Is So Hard to Treat
Most women with advanced ovarian cancer respond well to their first-line treatment, typically surgery followed by platinum-based chemotherapy, often combined with a taxane and increasingly with PARP inhibitors as maintenance. Response rates in the frontline setting can exceed 70 to 80%.
The problem is recurrence. About 70 to 80% of patients with advanced ovarian cancer relapse after initial treatment. When recurrence happens, the most important prognostic factor is how quickly it occurs after the last platinum therapy. Patients whose disease progresses more than six months after platinum are classified as platinum-sensitive and can be retreated with platinum. Patients whose disease progresses within six months are classified as platinum-resistant.
Platinum resistance is a watershed moment in the treatment arc. Non-platinum options, including weekly paclitaxel, pegylated liposomal doxorubicin, gemcitabine, and bevacizumab, produce response rates in the 10 to 20% range and median progression-free survival measured in months. Median overall survival in platinum-resistant ovarian cancer has historically ranged from roughly 12 to 16 months. These patients carry significant unmet need, and the disease is hard to control with anything currently available.
That is the context in which the KEYNOTE-B96 results need to be understood.
The KEYNOTE-B96 Trial: Design and Patient Population
KEYNOTE-B96 (also known as ENGOT-ov65, NCT05116189) was a multicenter, randomized, double-blind, placebo-controlled Phase 3 trial enrolling 643 patients with histologically confirmed epithelial ovarian, fallopian tube, or primary peritoneal carcinoma. Eligibility required:
- Platinum-resistant disease, defined as radiographic progression within six months of the last platinum-based regimen
- One or two prior lines of systemic therapy for ovarian carcinoma
- At least one prior platinum-based chemotherapy regimen
- Measurable disease by RECIST v1.1
Patients with primary platinum-refractory disease, meaning progression during or immediately after first-line platinum, were excluded.
Patients were randomized 1:1 to pembrolizumab plus weekly paclitaxel (80 mg/m² on days 1, 8, and 15 of each 3-week cycle), with or without bevacizumab (10 mg/kg every two weeks), or placebo plus the same backbone. Bevacizumab use was at investigator’s discretion and was a stratification factor. Stratification also included geographic region and PD-L1 expression by CPS.
The primary endpoint was investigator-assessed progression-free survival (PFS) by RECIST v1.1, evaluated first in the PD-L1 CPS of 1 or higher population, then in the ITT population. Overall survival was a key secondary endpoint.
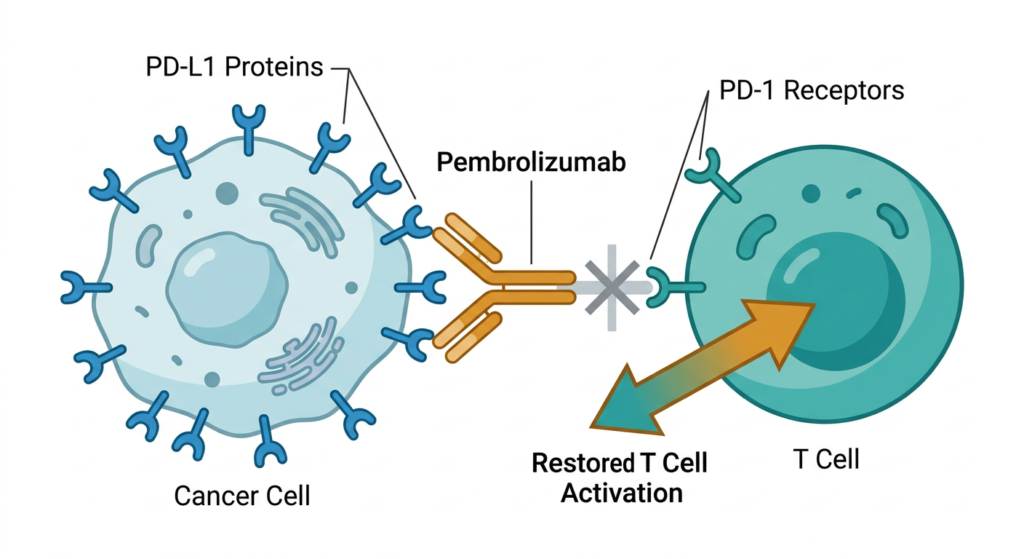
| What is PD-L1 CPS and why does it determine eligibility? PD-L1 Combined Positive Score (CPS) measures PD-L1 protein expression across tumor cells, tumor-associated lymphocytes, and macrophages. A CPS of 1 or higher means at least 1 PD-L1-staining cell per 100 tumor cells was detected. This is a relatively low threshold: in KEYNOTE-B96, approximately 466 of 643 patients (roughly 72%) had CPS of 1 or higher. The FDA approval is restricted to CPS of 1 or higher patients, where both PFS and OS benefits were demonstrated. The ITT population also showed significant PFS improvement, but the OS benefit was most clearly established in the CPS of 1 or higher group. This matters in practice: before receiving this regimen, a patient’s tumor must be tested with the FDA-approved companion diagnostic, the PD-L1 IHC 22C3 pharmDx assay, and return a CPS of 1 or higher result. This is a requirement, not a recommendation. |
|---|
The Results: Progression-Free Survival and Overall Survival
The trial conducted two pre-specified interim analyses. The second (IA2), with a data cutoff of May 5, 2025, was presented at ESMO Congress 2025 in Berlin in October 2025 and formed the basis for the February 2026 FDA approval. Final OS data were subsequently published in The Lancet in April 2026.
Progression-Free Survival
In the PD-L1 CPS of 1 or higher population (n=466), median PFS was 8.3 months with pembrolizumab versus 7.2 months with placebo, with a hazard ratio of 0.72 (95% CI 0.58 to 0.89; p=0.0014). The 12-month PFS rate was 35.2% for pembrolizumab versus 22.6% for placebo.
In the ITT population (all 643 patients), median PFS was 8.3 versus 6.4 months (HR 0.70; 95% CI 0.58 to 0.84; p less than 0.0001), with 12-month PFS rates of 33.1% versus 21.3%.
These are statistically significant and clinically meaningful improvements in a setting where six months of progression-free survival is often considered a reasonable benchmark.
Overall Survival
Among the 466 PD-L1 CPS of 1 or higher patients, median OS was 18.2 months in the pembrolizumab arm versus 14.0 months with placebo, a hazard ratio of 0.76 (95% CI 0.61 to 0.94; p=0.0053). The 12-month OS rate was 69.1% versus 59.3%. The 18-month OS rate was 51.5% versus 38.9%.
A four-month improvement in median OS. The first statistically significant overall survival benefit ever shown by an immune checkpoint inhibitor in ovarian cancer.
| Endpoint | Pembrolizumab plus chemo | Placebo plus chemo | HR (95% CI) | P-value |
|---|---|---|---|---|
| Median PFS (CPS of 1 or higher) | 8.3 months | 7.2 months | 0.72 (0.58 to 0.89) | 0.0014 |
| Median PFS (ITT) | 8.3 months | 6.4 months | 0.70 (0.58 to 0.84) | less than 0.0001 |
| Median OS (CPS of 1 or higher) | 18.2 months | 14.0 months | 0.76 (0.61 to 0.94) | 0.0053 |
| 12-month OS (CPS of 1 or higher) | 69.1% | 59.3% | — | — |
| 18-month OS (CPS of 1 or higher) | 51.5% | 38.9% | — | — |
Source: KEYNOTE-B96/ENGOT-ov65 Phase 3 trial, IA2 (data cutoff May 5, 2025). Final OS data: The Lancet, April 2026. FDA approval: February 10, 2026.
How to Read These Numbers Carefully
A four-month improvement in median OS is real and clinically meaningful in this setting, particularly given the historical absence of any survival benefit from immunotherapy in ovarian cancer. But it is worth understanding what the numbers do and don’t tell us.
The hazard ratio of 0.76 means that at any given point during the trial, patients in the pembrolizumab arm had a 24% lower risk of death than those in the placebo arm. This is not a cure. It is a reduction in the rate of events that translates into prolonged survival for a meaningful portion of patients. The 18-month OS rate shifting from 38.9% to 51.5% is the clearest way to see this: at 18 months, roughly one in eight additional patients were alive in the pembrolizumab arm compared to the placebo arm.
The approval is restricted to CPS of 1 or higher. About 72% of patients in KEYNOTE-B96 met this threshold, so most platinum-resistant ovarian cancer patients would be eligible for testing, but not all will test positive.
Median survival describes the midpoint of the distribution, not individual patient outcomes. Some patients in the pembrolizumab arm had substantially longer survival than 18 months. The final OS data from The Lancet publication provides a clearer view of the tail of the survival curve, which will help clarify whether there is a subset of patients with especially durable benefit, the pattern that checkpoint inhibitors sometimes produce in other tumors.
The Companion Diagnostic: What the PD-L1 Test Means in Practice
The FDA simultaneously approved the PD-L1 IHC 22C3 pharmDx assay (Agilent Technologies) as a companion diagnostic for identifying eligible patients. Tumor PD-L1 testing confirming CPS of 1 or higher is required before treatment, not optional.
The 22C3 pharmDx assay is the same companion diagnostic used in pembrolizumab approvals across multiple other tumor types, including cervical, endometrial, esophageal, and gastric cancers. At most academic medical centers and major oncology practices, this test is already part of the standard pathology workflow. At community oncology centers or in lower-resource settings, access to and turnaround time on the assay is a practical consideration worth discussing with the treating team.
Tumor tissue for PD-L1 testing can come from the original diagnosis or a recurrence biopsy. Given that PD-L1 expression can change with disease progression, some oncologists may prefer more recently collected tissue, though the label does not mandate this.
| What about bevacizumab? The approved regimen is pembrolizumab plus paclitaxel, with or without bevacizumab. Bevacizumab (Avastin) is an anti-VEGF antibody with established activity in ovarian cancer, including in the platinum-resistant setting. Its use in KEYNOTE-B96 was at investigator discretion and was a stratification factor. Patients with contraindications to anti-VEGF therapy, such as certain cardiovascular risk factors, recent major surgery, a history of GI perforation, or significant proteinuria, can receive pembrolizumab plus paclitaxel without bevacizumab. Review the full Keytruda prescribing information for complete contraindication guidance. |
|---|
Why Previous Immunotherapy Trials in Ovarian Cancer Failed, and Why This One Didn’t
The history of checkpoint inhibitor trials in ovarian cancer before KEYNOTE-B96 is largely a story of negative results. Earlier Phase 3 trials, including atezolizumab plus chemotherapy in frontline and maintenance settings, did not demonstrate meaningful survival improvements. Single-agent anti-PD-1 trials showed modest response rates of 10 to 15% in unselected ovarian cancer patients.
Several factors likely contributed. Ovarian cancer has a relatively immunosuppressive tumor microenvironment, with high regulatory T cell infiltration, immunosuppressive cytokines, and ascites fluid that dampens immune activity. Tumor mutational burden is generally lower than in cancers like melanoma or lung cancer that respond robustly to checkpoint inhibitors. And earlier trials often did not select for PD-L1 expression.
KEYNOTE-B96 made design choices that may have improved its chances. The combination with weekly paclitaxel, a metronomic dosing schedule thought to have immunomodulatory properties alongside its cytotoxic effects, may have made the tumor microenvironment more permissive to immune infiltration. The CPS of 1 or higher selection enriched for a more immunologically accessible population. These are mechanistic hypotheses with biological plausibility, not proven causal explanations, but they provide a rational basis for why this combination in this specific population succeeded where broader efforts did not.
Safety: What Patients and Clinicians Need to Know
The safety profile of the pembrolizumab combination in KEYNOTE-B96 was consistent with prior pembrolizumab trials. No new safety signals were identified.
Pembrolizumab carries immune-mediated adverse reactions as a class, the consequence of broadly activating the immune system. These can affect virtually any organ system.
Key immune-mediated risks:
- Pneumonitis: inflammation of the lungs; monitor for new or worsening respiratory symptoms
- Colitis: diarrhea and abdominal pain; may require corticosteroids or discontinuation
- Hepatitis: elevated liver enzymes; regular LFT monitoring during treatment
- Endocrinopathies: thyroid dysfunction, adrenal insufficiency, type 1 diabetes mellitus, hypophysitis
- Nephritis: elevated creatinine; monitor renal function
- Dermatologic reactions: rash, rare severe skin reactions including Stevens-Johnson syndrome
Most immune-mediated adverse reactions are manageable with corticosteroids if caught early. The prescribing information outlines detailed management algorithms, including when to hold versus permanently discontinue pembrolizumab.
Other warnings:
Infusion-related reactions: fever, chills, hypotension, and bronchospasm are possible. Standard premedication and monitoring protocols apply.
Embryo-fetal toxicity: pembrolizumab can cause fetal harm. Women of reproductive potential should use effective contraception during treatment and for at least four months after the final dose.
Dosing:
The approved pembrolizumab dose is 200 mg IV every three weeks or 400 mg IV every six weeks, until disease progression, unacceptable toxicity, or up to 24 months of treatment. Pembrolizumab is administered before paclitaxel and bevacizumab when given on the same day.
Keytruda Qlex, a subcutaneous formulation combining pembrolizumab with berahyaluronidase alfa-pmph, was also approved. The subcutaneous dose is 395 mg/4,800 units every three weeks or 790 mg/9,600 units every six weeks, and can be administered in approximately five to ten minutes rather than the 30-minute IV infusion. For patients receiving multiple cycles over months of treatment, this is a real reduction in clinic time.
Open Questions and the Road Ahead
The KEYNOTE-B96 approval opens a new chapter in ovarian cancer treatment, but several clinical questions will shape how the approval is used in practice.
How durable is the benefit?
The final OS data in The Lancet provides longer follow-up than the interim analysis. The field will be watching for a favorable tail on the survival curve, the pattern suggesting a subset of patients achieve especially prolonged disease control, which checkpoint inhibitors produce in some tumor types.
Does PD-L1 CPS fully capture who responds?
CPS of 1 or higher is a broad threshold. Within the PD-L1-positive population there is likely meaningful heterogeneity in response. Future work will examine whether higher CPS thresholds, tumor mutational burden, microsatellite instability status, or tumor-infiltrating lymphocyte density can further refine patient selection.
What about earlier lines of therapy?
The positive KEYNOTE-B96 result will prompt investigators to ask whether pembrolizumab-containing regimens have a role in the frontline or maintenance setting in ovarian cancer. Several trials are already exploring this. The data in those settings will need to be evaluated on their own terms.
Sequencing after progression on this regimen:
The approval covers patients after one or two prior regimens. What comes next for patients who progress on pembrolizumab plus chemotherapy? The treatment landscape at third or later lines remains difficult, and ongoing trials will need to address sequencing questions. ClinicalTrials.gov is the primary resource for identifying open studies.
| Project Orbis: A Global Review Pathway This approval was reviewed under Project Orbis, an FDA Oncology Center of Excellence initiative enabling concurrent submission and review across multiple international regulatory agencies. For KEYNOTE-B96, FDA collaborated with Australia’s Therapeutic Goods Administration, Health Canada, and Switzerland’s Swissmedic. Project Orbis doesn’t mean all countries approve simultaneously; each agency makes its own decision. But it creates a framework for data sharing that can accelerate global access. The designation signals that review is underway or completed in partner countries. |
|---|
What This Means for Patients With Platinum-Resistant Ovarian Cancer
For patients who have progressed after one or two lines of therapy and are now facing platinum-resistant disease, the conversation with their oncologist includes a genuinely new option for the first time. Pembrolizumab plus paclitaxel, with or without bevacizumab, is not a marginal refinement. It is the first regimen to improve overall survival in this population in a Phase 3 trial.
The first step is PD-L1 testing. Patients whose disease has not been recently biopsied may want to discuss with their oncologist whether fresh tissue for biomarker testing is feasible and clinically appropriate at the time of progression.
For related coverage of how immunotherapy and ADC approvals are expanding across gynecologic and breast cancers in 2026, see our posts on Dato-DXd in triple-negative breast cancer, vepdegestrant and the first PROTAC approval in oncology, and what the FDA’s contrasting decisions on camizestrant and vepdegestrant reveal about the future of ESR1-guided treatment.
Patient advocacy organizations with resources for ovarian cancer include the Ovarian Cancer Research Alliance, the National Ovarian Cancer Coalition, and the Foundation for Women’s Cancer. All three maintain clinical trial databases and physician directories. Patients interested in trials evaluating pembrolizumab in earlier-line ovarian cancer settings can search for open studies at ClinicalTrials.gov.
Sources
KEYNOTE-B96 trial registration: NCT05116189. ClinicalTrials.gov.
Final OS publication: KEYNOTE-B96/ENGOT-ov65 final overall survival analysis. The Lancet. April 2026.
Merck press release: Merck Announces Phase 3 KEYNOTE-B96 Trial Met Primary Endpoint of Progression-Free Survival. May 2025. merck.com.
OncLive approval coverage: KEYNOTE-B96 Approval Reinforces the Shift Toward Biomarker-Driven Treatment in Recurrent PROC. OncLive. March 2026.
Clinical review: The role of chemo-immunotherapy in platinum-resistant ovarian cancer in light of the KEYNOTE-B96 trial. PubMed Central.
Keytruda prescribing information: Keytruda (pembrolizumab) and Keytruda Qlex Prescribing Information. Merck. 2026.
Keytruda Qlex FDA approval: FDA approves pembrolizumab and berahyaluronidase alfa-pmph (Keytruda Qlex) for multiple indications.
Companion diagnostic: PD-L1 IHC 22C3 pharmDx. FDA list of cleared or approved companion diagnostics.
Project Orbis: Project Orbis. FDA Oncology Center of Excellence.
Patient resources: Ovarian Cancer Research Alliance | National Ovarian Cancer Coalition | Foundation for Women’s Cancer | ClinicalTrials.gov
| Disclaimer: Health Evidence Digest provides general health and regulatory information for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Treatment decisions for ovarian cancer should be made in consultation with a board-certified gynecologic oncologist experienced in managing platinum-resistant disease. |
|---|