
| 📌 Updated May 1, 2026: FDA Approval Confirmed The FDA approved vepdegestrant (Veppanu) on May 1, 2026, more than five weeks ahead of the June 5 PDUFA date. This post has been updated throughout to reflect the approval. For a companion analysis covering both this approval and the ODAC vote against camizestrant the day before, see: The FDA Said Yes to One ESR1 Drug and No to Another. |
|---|
For most of the past decade, the standard treatment arc for ER-positive, HER2-negative metastatic breast cancer has followed a recognizable sequence. First-line CDK4/6 inhibitor plus endocrine therapy. Disease progression. A second endocrine therapy, often fulvestrant. Progression again. Options narrowing.
A significant portion of patients progressing on that arc carry a specific tumor mutation in the ESR1 gene that makes their cancer actively resistant to standard endocrine therapies. Their tumors have evolved to activate the estrogen receptor without estrogen. For these patients, the question is not whether the disease will progress but how much time and quality of life can be preserved between progression events.
Vepdegestrant (Veppanu), developed by Arvinas and Pfizer, was approved by the FDA on May 1, 2026. It is designed specifically for this population. What makes it scientifically distinctive is not just its efficacy data but the mechanism. Vepdegestrant is a PROTAC: a drug that destroys its target protein rather than blocking it. It is the first drug of this type ever cleared in oncology.
The ESR1 Mutation Problem: How Tumors Learn to Ignore Endocrine Therapy
ER-positive breast cancer is driven by estrogen signaling through the estrogen receptor, a protein encoded by the ESR1 gene. Standard endocrine therapies work by either suppressing estrogen production (aromatase inhibitors) or blocking estrogen from binding to the receptor (fulvestrant). This works well initially. The problem develops over time.
Under the selective pressure of prolonged endocrine therapy, tumor cells can acquire point mutations in the ligand-binding domain of ESR1, the region where estrogen normally attaches to activate the receptor. These mutations cause the receptor to adopt an active conformation even in the absence of estrogen. The tumor has effectively rewired itself to bypass the treatment. The cancer grows because it no longer needs the hormone the therapy is trying to suppress.
This is not a rare edge case. Studies show ESR1 mutations are present in approximately 20 to 40% of ER+/HER2- metastatic breast cancer patients who have received prior aromatase inhibitor therapy, and the prevalence increases substantially with treatment lines, reaching as high as 59% in ctDNA analysis of patients in later lines. The broad adoption of CDK4/6 inhibitors in combination with aromatase inhibitors as the first-line standard has actually accelerated ESR1 mutation emergence, because the CDK4/6 inhibitor extends the duration of aromatase inhibitor exposure and thus the selective pressure for ESR1 mutations.
| Why ctDNA testing matters for this patient population ESR1 mutations are generally not present at initial diagnosis — they are acquired under treatment pressure. This means testing the primary tumor biopsy taken at diagnosis will miss them in most cases. Detection requires liquid biopsy (circulating tumor DNA, or ctDNA) testing on a blood sample taken after disease progression. ASCO and NCCN guidelines recommend ctDNA testing for ESR1 mutations in patients with ER+/HER2- advanced breast cancer progressing on endocrine therapy, because ESR1 mutation status now directly informs treatment selection. The FDA simultaneously approved the Guardant360 CDx as the companion diagnostic for identifying patients eligible for vepdegestrant. If you have ER+/HER2- advanced breast cancer and have not had ctDNA testing, discuss it with your oncologist. |
|---|
What Is a PROTAC? The Chemistry Behind a New Era of Cancer Drugs
To understand what makes vepdegestrant different from everything that came before, it helps to understand how conventional targeted therapies work and where they fall short.
Most existing targeted therapies, aromatase inhibitors, kinase inhibitors, CDK4/6 inhibitors, work by occupying the active site of a target protein and blocking its function. The analogy often used is a key and a lock: the drug sits in the lock and prevents the key from working. The protein is inhibited but remains present.
There are two fundamental problems with this approach in cancer. First, tumors can develop mutations that change the shape of the binding site, so the inhibitor no longer fits. The protein is still there; it’s just not blocked anymore. Second, some cancer-driving proteins don’t have conveniently accessible active sites at all, making conventional inhibition impossible. These are sometimes described as “undruggable” targets, a category that has driven decades of failed drug development attempts.
The PROTAC approach: degrade instead of block
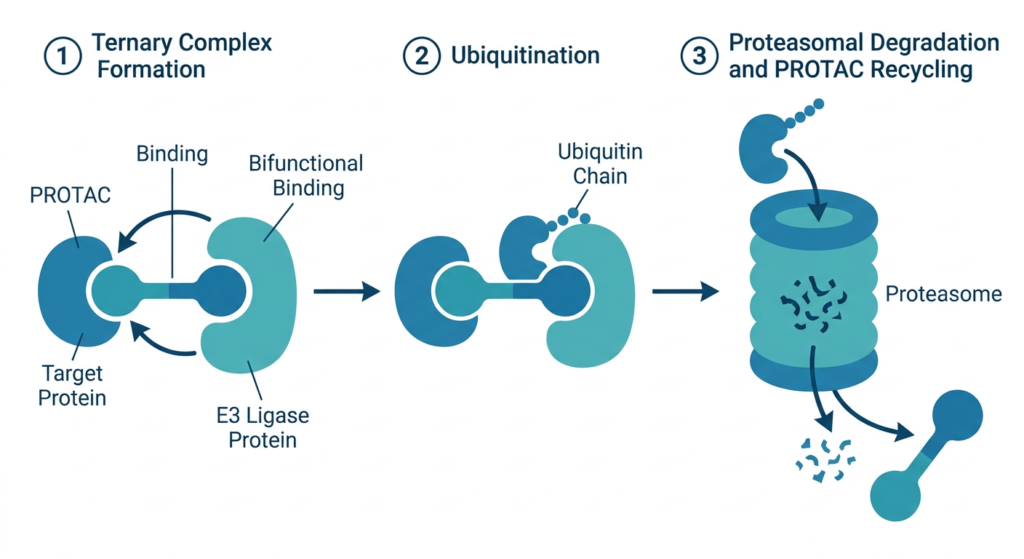
PROTAC stands for PROteolysis TArgeting Chimera. It is a bifunctional molecule: one end binds to the cancer-driving target protein (in vepdegestrant’s case, the estrogen receptor), and the other end recruits an E3 ubiquitin ligase. This ligase is part of the cell’s own protein disposal machinery, the ubiquitin-proteasome system. When both ends of the PROTAC connect their respective targets, the cell’s disposal machinery tags the cancer protein with ubiquitin chains. The tagged protein is then threaded through the proteasome, essentially a molecular shredder, and destroyed.
Once the protein is degraded, the PROTAC is released and can recruit the next copy of the target protein for destruction. This catalytic recycling means each PROTAC molecule can degrade multiple copies of the target, potentially making high drug concentrations less necessary. Because the mechanism destroys the protein rather than occupying its active site, resistance through active-site mutation is far harder. The tumor cannot mutate away from destruction the way it can mutate away from blockade.
| Feature | Traditional inhibitor (e.g., fulvestrant) | PROTAC (vepdegestrant) |
|---|---|---|
| Mechanism | Binds to and blocks target protein function | Recruits cell’s own disposal machinery to degrade target protein entirely |
| Target protein after treatment | Present but inhibited | Eliminated |
| Resistance pathway | Active-site mutations allow escape | Harder to mutate away from degradation |
| Drug efficiency | Must maintain continuous occupancy (stoichiometric) | Each molecule can be recycled (catalytic) |
| Druggability range | Requires accessible active site | Can target proteins without conventional drug-binding pockets |
| Administration | Intramuscular injection (fulvestrant) | Oral, once daily (vepdegestrant) |
The VERITAC-2 Trial: What the Data Shows and What It Doesn’t
The FDA approval is based on data from VERITAC-2 (NCT05654623), a global, randomized, open-label Phase 3 trial. It enrolled 624 patients with ER+/HER2- advanced or metastatic breast cancer whose disease had progressed on prior CDK4/6 inhibitor plus endocrine therapy. Patients were stratified by ESR1 mutation status and presence of visceral disease, then randomized 1:1 to receive vepdegestrant 200 mg orally once daily or fulvestrant 500 mg by intramuscular injection. VERITAC-2 data were presented at the 2025 ASCO Annual Meeting and simultaneously published in The New England Journal of Medicine.
Efficacy results
| Endpoint | Vepdegestrant | Fulvestrant |
|---|---|---|
| ESR1-mutated subpopulation (n=270) | ||
| Median PFS (BICR) | 5.0 months (95% CI 3.7 to 7.4) | 2.1 months (95% CI 1.9 to 3.5) |
| Hazard ratio | 0.58 (95% CI 0.43 to 0.78) | Reference |
| p-value | less than 0.001 | — |
| Risk reduction | 43% | — |
| Treatment ongoing at analysis | 33% | 12% |
| Overall population (ITT, n=624) | ||
| Median PFS (BICR) | 3.8 months (95% CI 3.7 to 5.3) | 3.6 months (95% CI 2.6 to 4.0) |
| Hazard ratio (ITT) | 0.83 (95% CI 0.69 to 1.01) | Reference |
| p-value (ITT) | 0.07, NOT statistically significant | — |
| Overall survival | Immature at analysis | — |
| The ITT miss is the most important nuance in this dataset The VERITAC-2 trial had two primary endpoints: PFS in the ESR1-mutated subpopulation and PFS in the overall intent-to-treat (ITT) population. Vepdegestrant met the first. It did not meet the second: overall ITT PFS was 3.8 versus 3.6 months (HR 0.83, p=0.07), which missed statistical significance. This matters for how the FDA scoped the approval. The indication is specifically for patients with ESR1-mutated tumors, not all comers with ER+/HER2- advanced disease. The drug does not appear to add meaningful benefit in the absence of this mutation. This pattern has been seen before: elacestrant (Orserdu), the currently approved oral SERD for this population, similarly showed its benefit confined to the ESR1-mutated subgroup in the EMERALD trial. The biology makes sense: patients whose tumors don’t carry ESR1 mutations are progressing through other resistance mechanisms that ESR1-targeting drugs don’t address. The clinical implication is that biomarker testing is not optional here. ESR1 mutation status is the selection criterion. |
|---|
Safety Profile: What the Trial Showed
Vepdegestrant was generally well tolerated, with no unexpected safety signals in VERITAC-2. The FDA label includes important warnings about QTc interval prolongation and embryo-fetal toxicity that clinicians and patients should be aware of.
| Adverse Event | Vepdegestrant | Fulvestrant |
|---|---|---|
| Fatigue (all grade) | 26.6 to 27% | 16% |
| Elevated ALT (all grade) | 14.4% | 10% |
| Elevated AST (all grade) | 14.4% | 10% |
| Nausea (all grade) | 13% | 9% |
| Grade 3 or higher adverse events | 23.4% | 17.6% |
| Treatment discontinuation due to AEs | 2.9% | 0.7% |
| QTc prolongation | Signal present; routine monitoring required per label | Not a labeled concern |
| New or unexpected safety signals | None identified | — |
The elevated liver enzyme findings (ALT and AST) were predominantly low-grade and did not commonly lead to discontinuation. Fatigue at 27% versus 16% is meaningfully higher than with fulvestrant and worth discussing with patients proactively. The QTc prolongation signal in the label requires routine electrocardiogram monitoring during treatment, particularly when vepdegestrant is used in combination with other QTc-prolonging agents. The 2.9% discontinuation rate due to adverse events, while slightly higher than fulvestrant’s 0.7%, remains low in absolute terms for a heavily pre-treated metastatic population.
Where Vepdegestrant Fits: The ESR1-Mutated Treatment Landscape
Vepdegestrant is not the first drug developed specifically for ESR1-mutated ER+ metastatic breast cancer, but it is the first PROTAC in this space. Understanding where it sits relative to elacestrant requires knowing the current options.
| Drug | Class | FDA Status | Key Trial |
|---|---|---|---|
| Fulvestrant (Faslodex) | SERD (injection) | Approved, current standard | Multiple trials; no ESR1-specific indication |
| Elacestrant (Orserdu) | Oral SERD | Approved January 2023, ESR1-mutated ER+/HER2- MBC | EMERALD: PFS 2.8 vs 1.9 months (ESR1m), HR 0.55 |
| Vepdegestrant (Veppanu) | Oral PROTAC ER degrader | Approved May 1, 2026, ESR1-mutated ER+/HER2- MBC | VERITAC-2: PFS 5.0 vs 2.1 months (ESR1m), HR 0.58 |
The natural comparison is to elacestrant, the only previously approved oral SERD for ESR1-mutated ER+ metastatic breast cancer. Elacestrant showed PFS of 2.8 versus 1.9 months in the ESR1-mutated population of EMERALD (HR 0.55). Vepdegestrant showed 5.0 versus 2.1 months (HR 0.58). The numerics look more favorable for vepdegestrant, but these are separate trials with different patient populations, different prior treatment histories, and different control arms. Cross-trial comparisons are unreliable and should not be used to conclude one drug is superior to the other. No head-to-head trial exists.
What the landscape now offers is two approved oral options in the ESR1-mutated second-line setting, with different mechanisms and safety profiles. The sequencing question — which drug to use in which patient, and what comes after progression on either — is one the field will be working through over the next several years as real-world experience accumulates.
For a detailed analysis of how the vepdegestrant approval compares to the same-day ODAC vote against camizestrant, and what both decisions reveal about ctDNA-guided treatment strategies, see our post: The FDA Said Yes to One ESR1 Drug and No to Another.
Beyond Vepdegestrant: Why a PROTAC Approval Matters for All of Cancer Medicine
The significance of vepdegestrant’s approval extends well beyond this particular drug and patient population. Dozens of PROTAC candidates are currently in clinical development for a range of cancers, and this first approval validates the entire platform in a way that decades of academic research could not.
The PROTAC approach is particularly promising for what oncologists call “undruggable” targets, proteins that drive cancer growth but don’t have accessible pockets for conventional inhibitors. Mutant KRAS, certain transcription factors, and specific fusion proteins have resisted decades of drug development attempts. PROTAC-based degradation sidesteps the binding-site requirement, potentially making these targets approachable for the first time.
In breast cancer specifically, ongoing trials are exploring vepdegestrant in combination with CDK4/6 inhibitors. The VERITAC-1 Phase 1/2 study established tolerability for the vepdegestrant plus palbociclib combination. If vepdegestrant demonstrates durable benefit in combination regimens, the scope of its utility could expand significantly beyond the current second-line monotherapy setting.
What This Means for Patients Right Now
Vepdegestrant (Veppanu) is now FDA-approved and commercially available. Here is what patients navigating ER+/HER2- metastatic breast cancer should know:
- If you have ER+/HER2- metastatic breast cancer and have progressed on CDK4/6 inhibitor-based therapy: ask your oncologist whether your tumor has been tested for ESR1 mutations via ctDNA liquid biopsy. This is increasingly the standard of care and directly affects which therapies are appropriate. The Guardant360 CDx is the FDA-approved companion diagnostic for this indication.
- If you already have an ESR1 mutation documented: both elacestrant (Orserdu) and vepdegestrant (Veppanu) are now approved options in this setting. Discuss with your oncologist which is appropriate for your situation.
- If you are in earlier lines of treatment: vepdegestrant is specifically approved for patients who have already received CDK4/6 inhibitor plus endocrine therapy. It is not a first-line option.
- Do not wait to have the ESR1 testing conversation. Whether or not you are currently considering vepdegestrant, ESR1 mutation status is clinically actionable today because of both approved agents.
The treatment landscape for ER+/HER2- metastatic breast cancer is evolving faster than at any point in the past decade. The key resources for staying current include NCCN Clinical Practice Guidelines, the Metastatic Breast Cancer Alliance, and Living Beyond Breast Cancer, which maintains patient-facing resources on ESR1 mutations, ctDNA testing, and treatment options in the endocrine-resistant setting.
Sources
NEJM primary publication: Hamilton E et al. Vepdegestrant, a PROTAC Estrogen Receptor Degrader, in Advanced Breast Cancer. New England Journal of Medicine. 2025. doi:10.1056/NEJMoa2505725
VERITAC-2 trial registration: NCT05654623. ClinicalTrials.gov.
Arvinas FDA approval announcement: Arvinas Announces FDA Approval of VEPPANU (vepdegestrant). GlobeNewswire. May 1, 2026.
AJMC approval coverage: FDA Approves Vepdegestrant for ESR1-Mutated, ER-Positive, HER2-Negative Advanced Breast Cancer. AJMC. May 2026.
VERITAC-2 study design (PMC): VERITAC-2: a Phase III study of vepdegestrant, a PROTAC ER degrader, versus fulvestrant in ER+/HER2- advanced breast cancer. PMC11524203.
ESR1 mutation prevalence: Comprehensive genomic profiling of ESR1 in HR+/HER2- MBC. PMC11420341.
Nature Reviews Clinical Oncology: PROTAC SERD vepdegestrant outperforms fulvestrant for advanced-stage ER+HER2- breast cancer harbouring acquired ESR1 mutations. Nat Rev Clin Oncol. 2025. doi:10.1038/s41571-025-01062-6
Elacestrant FDA approval: FDA approves elacestrant for ER-positive, HER2-negative, ESR1-mutated breast cancer. FDA.gov. January 2023.
Patient resources: NCCN Guidelines | MBC Alliance | Living Beyond Breast Cancer | Guardant360 CDx information
| Disclaimer: Health Evidence Digest provides general information about clinical trials and FDA regulatory processes for educational purposes. This content is not a substitute for professional medical advice. Treatment decisions for metastatic breast cancer should be made in close consultation with a qualified oncologist who can account for your individual diagnosis, tumor characteristics, and treatment history. |
|---|
Leave a Reply