| 📌 The essentials On June 24, 2026, the FDA approved two new first-line indications for Trodelvy (sacituzumab govitecan-hziy, Gilead Sciences) in adults with unresectable locally advanced or metastatic triple-negative breast cancer (TNBC): Indication 1 (monotherapy): as a single agent for adults with unresectable locally advanced or metastatic TNBC who are not candidates for PD-1 or PD-L1 inhibitor-based therapy. Supported by ASCENT-03. Indication 2 (combination): in combination with pembrolizumab (Keytruda) or pembrolizumab and berahyaluronidase alfa-pmph (Keytruda Qlex) for adults with unresectable locally advanced or metastatic TNBC whose tumors express PD-L1 (combined positive score [CPS] at or above 10) as determined by an FDA-authorized test. Supported by ASCENT-04/KEYNOTE-D19. These are new first-line approvals; Trodelvy was previously approved for second-line and later treatment in TNBC (2020) and HR+/HER2-low breast cancer (2023). The clinical basis: ASCENT-03 (NCT05382299): 558 patients, first-line TNBC ineligible for PD-(L)1 inhibitors, randomized 1:1 to sacituzumab govitecan 10 mg/kg days 1 and 8 of a 21-day cycle versus physician’s choice chemotherapy. Median PFS 9.7 months versus 6.9 months; HR 0.62 (95% CI 0.50 to 0.77; p less than 0.0001); 38% reduction in risk of progression or death. Median DOR 12.2 months versus 7.2 months. ORR 48% versus 46%. OS data immature. ASCENT-04/KEYNOTE-D19 (NCT05382286): 443 patients, first-line PD-L1-positive (CPS at or above 10) TNBC, randomized to sacituzumab govitecan plus pembrolizumab versus physician’s choice chemotherapy plus pembrolizumab. Median PFS 11.2 months versus 7.8 months; HR 0.65 (95% CI 0.51 to 0.84; p=0.0009); 35% reduction in risk of progression or death. Confirmed ORR 61% versus 55%. OS not reached in either arm at data cutoff. Mechanism: sacituzumab govitecan is a Trop-2-directed antibody-drug conjugate (ADC) that delivers the topoisomerase I inhibitor SN-38 specifically to Trop-2-expressing cancer cells. Trop-2 is highly expressed in TNBC. Boxed warnings: severe neutropenia; severe diarrhea. Both are manageable with established protocols. |
|---|
Triple-negative breast cancer is defined by what it lacks: no estrogen receptor expression, no progesterone receptor expression, and no HER2 overexpression. That combination of absences eliminates three of the most productive therapeutic targets in modern breast cancer medicine. There is no endocrine therapy. There is no HER2-directed antibody. For decades, the treatment toolkit for TNBC was essentially the same chemotherapy regimens that oncology had in the 1990s.
The arrival of pembrolizumab plus chemotherapy for PD-L1-positive TNBC in 2021 represented the last major first-line shift. But pembrolizumab only helps patients whose tumors express PD-L1 at adequate levels, roughly half of the metastatic TNBC population. For the other half, the patients with PD-L1-negative disease or contraindications to immunotherapy, the standard of care in 2025 was still first-line chemotherapy.
That remained true for more than 20 years after TNBC was first defined as a distinct subtype. As Dr. Javier Cortés, Head of the International Breast Cancer Center in Spain and principal investigator of ASCENT-03, put it: the ASCENT-03 outcome represents the first clinically meaningful advance for this patient population in more than 20 years.
The June 24, 2026 FDA approvals give Trodelvy (sacituzumab govitecan-hziy, Gilead Sciences) a first-line role across the full spectrum of metastatic TNBC, whether or not the patient is eligible for immunotherapy, based on two Phase 3 trials both published in the New England Journal of Medicine.
What Triple-Negative Breast Cancer Is and Why It Has Been So Hard to Treat
Breast cancer is not one disease. It is a collection of molecularly distinct subtypes with different drivers, different natural histories, and different therapeutic vulnerabilities. The most common subtypes, hormone receptor-positive breast cancers, are driven by estrogen and progesterone signaling and are treated with endocrine therapies that can maintain disease control for years. HER2-positive cancers are driven by HER2 amplification and are effectively treated with targeted antibodies and antibody-drug conjugates. Both subtypes have seen dramatic survival improvements over the past 30 years.
Triple-negative breast cancer accounts for approximately 10 to 15% of all breast cancers, but its clinical impact is disproportionate to its prevalence. TNBC is more common in younger women and is overrepresented in women of African descent, for whom the incidence rate is approximately double that of white women. It tends to grow rapidly and metastasize early. Unlike hormone receptor-positive disease, which can smolder for years before progressing, TNBC often spreads and becomes lethal within months of metastatic diagnosis.
The five-year survival rate for metastatic TNBC is approximately 12%, compared with 28% for other metastatic breast cancer subtypes. Nearly half of patients diagnosed with metastatic TNBC never receive a second line of therapy, making the first line of treatment the most consequential decision in their care. That clinical reality is the context within which both ASCENT-03 and ASCENT-04 must be understood.
The PD-L1 split that defines the treatment landscape
The 2021 approval of pembrolizumab plus chemotherapy (KEYNOTE-522) for PD-L1-positive metastatic TNBC was a meaningful advance, but it created a fork in the treatment pathway. To receive pembrolizumab, patients must have PD-L1 expression with a combined positive score (CPS) at or above 10, as measured by the PD-L1 IHC 22C3 pharmDx assay. Patients who are PD-L1-negative by this criterion, or who have contraindications to checkpoint inhibition (autoimmune conditions, organ transplantation, severe prior immune-related adverse events), have not been eligible for the pembrolizumab combination and have faced first-line chemotherapy alone.
ASCENT-03 is specifically designed for this PD-L1-ineligible population. ASCENT-04 targets the PD-L1-positive population and asks whether replacing chemotherapy with an ADC as the partner to pembrolizumab improves on the current standard.
The Science: What Sacituzumab Govitecan Is and How It Works
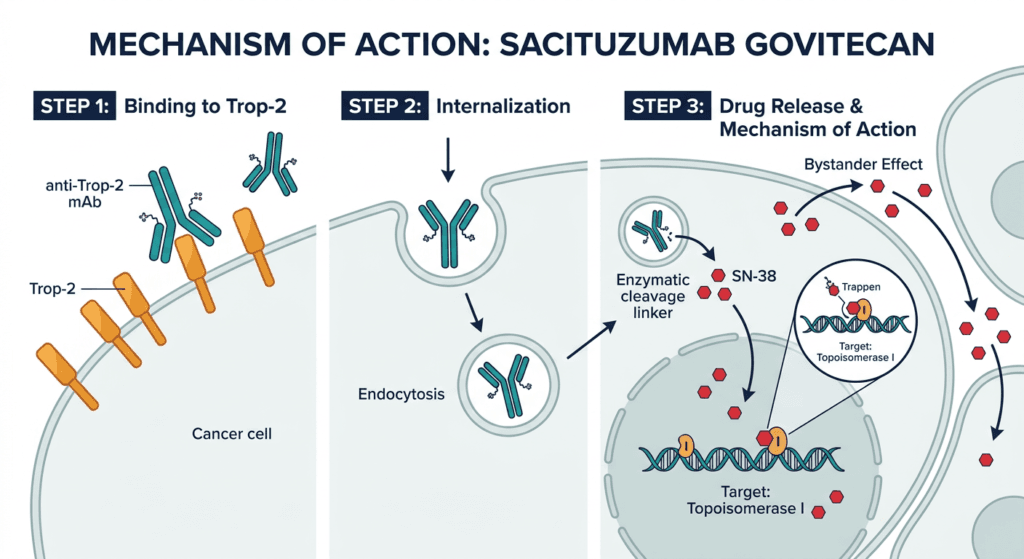
Sacituzumab govitecan is an antibody-drug conjugate (ADC): a targeted delivery vehicle that combines a cancer-specific antibody with a cytotoxic drug payload, connected by a chemical linker designed to release the payload preferentially inside tumor cells.
The three components of sacituzumab govitecan are:
The antibody: anti-Trop-2. Trop-2 (trophoblast cell-surface antigen 2) is a transmembrane glycoprotein that is highly expressed on the surface of many epithelial cancer cells, including the vast majority of TNBC tumors. Its expression in normal adult tissues is comparatively low, making it a useful tumor-targeting antigen. The anti-Trop-2 antibody in sacituzumab govitecan binds to Trop-2-expressing cancer cells and is internalized through receptor-mediated endocytosis, bringing the payload inside the cell.
The linker: hydrolysable. Unlike ADCs with stable, non-cleavable linkers that only release payload inside target cells, the hydrolysable linker in sacituzumab govitecan releases some active payload in the tumor microenvironment after internalization. This creates a “bystander effect”: neighboring cancer cells that may express lower levels of Trop-2 are also exposed to SN-38, potentially expanding the drug’s activity beyond the highest-Trop-2-expressing cells.
The payload: SN-38. SN-38 is the active metabolite of irinotecan, a topoisomerase I inhibitor. Topoisomerase I is an enzyme that relieves torsional stress in DNA during replication by creating temporary single-strand breaks. SN-38 traps topoisomerase I in a complex with DNA, preventing the breaks from being resealed. The result is irreversible DNA double-strand breaks during replication, triggering apoptosis. SN-38 is approximately 100 to 1,000 times more potent than irinotecan itself. The ADC delivery format allows higher intratumoral concentrations of SN-38 than would be tolerable with systemic irinotecan.
The drug-to-antibody ratio (DAR) of sacituzumab govitecan is approximately 7.6, meaning roughly 7 to 8 SN-38 molecules are attached per antibody. This high DAR, unusual among approved ADCs, contributes to the drug’s potency at Trop-2-expressing tumors.
ASCENT-03: The Monotherapy Indication
Design
ASCENT-03 (NCT05382299) was a Phase 3, multicenter, open-label, randomized trial enrolling 558 adults with unresectable locally advanced or metastatic TNBC who had not received prior systemic therapy for advanced disease and who were not candidates for PD-1 or PD-L1 inhibitor therapy. The enrollment criteria specifically required that patients either had PD-L1-negative tumors (CPS below 10) or had PD-L1-positive tumors but could not receive immunotherapy due to comorbidities.
Patients were randomized 1:1 to:
- Sacituzumab govitecan 10 mg/kg IV on days 1 and 8 of a 21-day cycle
- Physician’s choice chemotherapy (paclitaxel, nab-paclitaxel, or gemcitabine plus carboplatin)
The primary endpoint was progression-free survival (PFS) per blinded independent central review (BICR). Key secondary endpoints included overall survival (OS), objective response rate (ORR), duration of response (DOR), and safety.
Results
At a median follow-up of 13.2 months, sacituzumab govitecan demonstrated a statistically significant and clinically meaningful improvement in PFS compared with chemotherapy, with a median PFS of 9.7 months versus 6.9 months, representing a 38% reduction in the risk of disease progression or death (HR 0.62; 95% CI 0.50 to 0.78; p less than 0.0001). BioSpace
| Endpoint | Sacituzumab govitecan | Chemotherapy (TPC) | Result |
|---|---|---|---|
| Median PFS (BICR) | 9.7 months (95% CI 8.1 to 11.1) | 6.9 months (95% CI 5.6 to 8.2) | HR 0.62 (95% CI 0.50 to 0.77); p less than 0.0001 |
| Risk reduction in progression or death | 38% | Reference | — |
| ORR | 48% (95% CI 42% to 54%) | 46% (95% CI 40% to 52%) | Comparable |
| Median DOR | 12.2 months (95% CI 9.7 to 13.8) | 7.2 months (95% CI 5.7 to 8.4) | Substantially longer with SG |
| Median PFS2 (time to next progression) | 18.2 months (95% CI 15.9 to NR) | 14.0 months (95% CI 12.5 to 17.4) | HR 0.70 (95% CI 0.55 to 0.90) |
| OS | Data immature (37% maturity at cutoff) | Data immature | No OS detriment observed |
Source: Cortés J et al. Sacituzumab Govitecan in Untreated, Advanced Triple-Negative Breast Cancer. NEJM. 2025. doi:10.1056/NEJMoa2511734. ASCENT-03, abstract LBA20, ESMO 2025.
The ORR was 48% with sacituzumab govitecan versus 46% with chemotherapy, with similar rates but a substantially longer median DOR with sacituzumab govitecan (12.2 months versus 7.2 months). The PFS benefit was consistent across prespecified subgroups, including patients with poor prognostic features such as disease recurrence within one year of prior curative therapy. FDA
The treatment discontinuation rate due to adverse events was lower with sacituzumab govitecan than with chemotherapy, a finding that supports the tolerability of the ADC relative to standard cytotoxic regimens in this population.
ASCENT-04/KEYNOTE-D19: The Combination Indication
Design
ASCENT-04/KEYNOTE-D19 (NCT05382286) was a Phase 3, multicenter, open-label, randomized trial enrolling 443 adults with locally advanced or metastatic TNBC who had not received prior systemic therapy for advanced disease and whose tumors expressed PD-L1 at a CPS of 10 or greater, confirmed centrally using the PD-L1 IHC 22C3 pharmDx assay.
Patients were randomized to:
- Sacituzumab govitecan 10 mg/kg IV days 1 and 8 of a 21-day cycle plus pembrolizumab 200 mg IV on day 1 every 3 weeks (n=221)
- Physician’s choice chemotherapy plus pembrolizumab 200 mg IV on day 1 every 3 weeks (n=222)
The primary endpoint was PFS by BICR.
Results
At a data cutoff of March 3, 2025, sacituzumab govitecan plus pembrolizumab led to a median PFS of 11.2 months (95% CI 9.3 to 16.7) versus 7.8 months (95% CI 7.3 to 9.3) with chemotherapy plus pembrolizumab, translating to a 35% reduction in the risk of disease progression or death (HR 0.65; 95% CI 0.51 to 0.84; p less than 0.001). Patient Care Online
| Endpoint | SG plus pembrolizumab | Chemo plus pembrolizumab | Result |
|---|---|---|---|
| Median PFS (BICR) | 11.2 months (95% CI 9.3 to 16.7) | 7.8 months (95% CI 7.3 to 9.3) | HR 0.65 (95% CI 0.51 to 0.84); p=0.0009 |
| Risk reduction in progression or death | 35% | Reference | — |
| 6-month PFS rate | 72% (95% CI 65% to 77%) | 63% (95% CI 56% to 70%) | — |
| 12-month PFS rate | 48% (95% CI 41% to 56%) | 38% (95% CI 31% to 45%) | — |
| Confirmed ORR | 61% (95% CI 55% to 68%) | 55% (95% CI 48% to 62%) | — |
| Median OS | Not reached | Not reached | Immature; no OS detriment |
Source: Tolaney SM et al. Sacituzumab govitecan plus pembrolizumab in first-line PD-L1-positive TNBC. ASCO 2025 / NEJM 2025. doi:10.1056/NEJMoa2511736. ASCENT-04/KEYNOTE-D19 NCT05382286.
An important contextual note: 43% of patients on the chemotherapy-plus-pembrolizumab arm crossed over to receive sacituzumab govitecan as a single agent in the second line, accounting for 81% of those who received subsequent treatment. The fact that the combination still showed statistically significant PFS benefit despite high crossover to the ADC in the control arm’s next line is a meaningful finding, because crossover typically dilutes the OS benefit in second-line crossover-heavy trials. Patient Care Online
Dr. Sara M. Tolaney, MD, MPH, chief of the Division of Breast Oncology at Dana-Farber Cancer Institute and principal investigator for ASCENT-04, described the combination as resulting in a statistically significant and clinically meaningful improvement in PFS in the first-line PD-L1-positive metastatic TNBC setting.
The Approval Framework: Two Indications Split by PD-L1 Status
The two new approvals create a rational treatment framework that mirrors how oncologists already stratify TNBC patients before initiating first-line therapy:
| Patient profile | New first-line standard of care | Trial support |
|---|---|---|
| TNBC, not eligible for PD-(L)1 inhibitor therapy (PD-L1 CPS below 10, or contraindicated) | Trodelvy monotherapy (sacituzumab govitecan) | ASCENT-03 |
| TNBC, PD-L1 CPS at or above 10 (confirmed by FDA-authorized assay) | Trodelvy plus Keytruda or Keytruda Qlex (sacituzumab govitecan plus pembrolizumab) | ASCENT-04 |
The key practical implication for oncology teams: PD-L1 testing using the 22C3 pharmDx assay is now a required step in first-line treatment planning for metastatic TNBC. This test was already standard of care at many centers for the pembrolizumab decision; the new approvals make it universal.
Ricki Fairley, co-founder and CEO of TOUCH, The Black Breast Cancer Alliance, noted that because so many patients may never receive subsequent lines of therapy, the ability to start with an effective option like Trodelvy with or without Keytruda in the first line is critical, particularly given TNBC’s disproportionate impact on Black women.
Trodelvy’s Complete Indication Picture After June 2026
Trodelvy now holds approvals across multiple settings in TNBC and beyond: Contagion Live
| Indication | Approval date | Key trial |
|---|---|---|
| Previously treated (at or above 2 prior lines) metastatic TNBC | April 2020 | ASCENT |
| Previously treated unresectable locally advanced or metastatic HR+/HER2-low breast cancer after endocrine therapy | February 2023 | TROPiCS-02 |
| First-line metastatic TNBC, not eligible for PD-(L)1 inhibitors (monotherapy) | June 24, 2026 | ASCENT-03 |
| First-line metastatic TNBC, PD-L1 CPS at or above 10 (plus pembrolizumab) | June 24, 2026 | ASCENT-04 |
Safety: What Prescribers and Patients Need to Know
Sacituzumab govitecan carries a boxed warning for two serious adverse reactions, both attributable to the SN-38 topoisomerase I inhibitor payload.
Severe neutropenia (boxed warning): Grade 3 or higher neutropenia occurred in 43% of sacituzumab govitecan-treated patients in ASCENT-03. Neutropenia is the most clinically significant toxicity and requires proactive management. Granulocyte colony-stimulating factor (G-CSF) prophylaxis is strongly recommended and substantially reduces the severity and duration of neutropenic episodes. Complete blood count monitoring before each dose is standard. Dose reduction or delay may be required for severe neutropenia. Sanofi
Severe diarrhea (boxed warning): SN-38 causes significant gastrointestinal toxicity through its topoisomerase I inhibition in intestinal epithelium. Grade 3 or higher diarrhea occurred in 9% of sacituzumab govitecan-treated patients in ASCENT-03, compared with 16% with anemia in the chemotherapy arm. Management includes early loperamide at the first sign of loose stools and dose modification for persistent severe diarrhea. Patients with UGT1A1*28 homozygous genotype (reduced SN-38 glucuronidation) are at higher risk for both neutropenia and diarrhea and require dose reduction. Sanofi
Additional key safety information:
| Safety item | Details | Clinical guidance |
|---|---|---|
| Severe neutropenia (boxed warning) | Grade 3 or higher neutropenia in approximately 43% in ASCENT-03; febrile neutropenia possible | G-CSF prophylaxis strongly recommended; CBC before each dose; dose modification per prescribing information |
| Severe diarrhea (boxed warning) | Grade 3 or higher in approximately 9%; early-onset (within days of infusion) common | Loperamide at first sign of loose stools; dose modification for severe or persistent diarrhea |
| UGT1A1 genotype | Patients homozygous for UGT1A128 (poor metabolizers) have reduced SN-38 clearance and higher toxicity risk | Starting dose reduction to 7.5 mg/kg recommended in homozygous UGT1A128 patients |
| Nausea and vomiting | Common; manageable with antiemetics | Prophylactic antiemetics recommended; anti-nausea medications as needed |
| Hypersensitivity and infusion reactions | Severe reactions including anaphylaxis reported | Premedication; monitoring during infusion; resuscitation capability required |
| Embryo-fetal toxicity | SN-38 can cause fetal harm | Effective contraception during treatment and for 6 months after last dose for females; 3 months for males |
| Pembrolizumab-related toxicities (combination indication) | Immune-mediated adverse reactions including pneumonitis, colitis, hepatitis, endocrinopathies; infusion reactions | Refer to Keytruda prescribing information for full immune-related AE management guidance |
| Serious adverse reactions in ASCENT-03 CheckRare | Occurred in 26% of patients; fatal adverse reactions in 2.5% | Close clinical monitoring; dose modification per prescribing information |
What This Means for Patients and Oncology Teams
For patients with metastatic TNBC not eligible for immunotherapy
This population has had no meaningful treatment advance since TNBC was defined more than 20 years ago. ASCENT-03 represents the first clinically meaningful advance for this patient population in over 20 years, according to Dr. Cortés. The 38% reduction in progression risk, the nearly 3-month improvement in median PFS (9.7 versus 6.9 months), and the dramatically longer duration of response (12.2 versus 7.2 months) constitute a clinically significant departure from what chemotherapy alone has provided. Pfizer
For oncologists managing these patients: sacituzumab govitecan monotherapy is now an FDA-approved first-line standard for PD-(L)1-ineligible metastatic TNBC. The G-CSF prophylaxis requirement and the UGT1A1 genotype assessment should be part of the treatment initiation workup.
For patients with PD-L1-positive metastatic TNBC
The ASCENT-04 data establishes sacituzumab govitecan plus pembrolizumab as a new first-line option for patients with CPS at or above 10, with a 35% reduction in progression risk over the prior standard of chemotherapy plus pembrolizumab. The combination’s 11.2-month median PFS and 61% ORR represent a meaningful improvement over what was achievable in this setting.
The combination requires PD-L1 testing before initiation, coordination of the ADC and checkpoint inhibitor schedules, and management of both SN-38 toxicities (neutropenia, diarrhea) and potential immune-mediated adverse events from pembrolizumab.
The sequencing question and OS data
One important clinical caveat applies to both approvals: overall survival data were immature at the time of analysis for both ASCENT-03 and ASCENT-04. The PFS benefit is established and statistically significant, but whether first-line Trodelvy translates into longer overall survival will depend on mature OS data from ongoing follow-up. Given the high crossover rate in ASCENT-04 (43% of control arm patients received sacituzumab govitecan in the second line), the OS signal may be attenuated even if the drug provides genuine survival benefit. These are data to watch in updated analyses from both trials.
For patients and families navigating a new metastatic TNBC diagnosis: the National Breast Cancer Foundation, Susan G. Komen Foundation, and TOUCH, The Black Breast Cancer Alliance all maintain current patient resources including clinical trial locators and financial assistance navigation for Trodelvy access.
For related HED coverage on oncology ADC approvals and breast cancer treatment advances, see our prior coverage on Pomalyst (pomalidomide) and what the multiple myeloma treatment landscape looks like as generic competition arrives in the 2026 LOE series.
Sources
FDA approval announcement: FDA approves sacituzumab govitecan-hziy as monotherapy and in combination with pembrolizumab for first-line treatment of triple-negative breast cancer. FDA.gov. June 24, 2026.
Gilead press release: U.S. FDA approves Trodelvy for first-line treatment of metastatic triple-negative breast cancer. gilead.com. June 24, 2026.
ASCO Post approval summary: FDA Approves Sacituzumab Govitecan-hziy as Monotherapy and in Combination With Pembrolizumab for First-Line Treatment of TNBC. ascopost.com. June 2026.
Pharmacy Times clinical review: FDA Approves Sacituzumab Govitecan for First-Line Treatment of Advanced Triple-Negative Breast Cancer. pharmacytimes.com. June 2026.
BioPharm International clinical summary: Trop-2-Directed ADC Sacituzumab Govitecan Earns FDA Approval in First-Line Metastatic TNBC. biopharminternational.com. June 2026.
CancerNetwork detailed clinical summary: Sacituzumab Govitecan Receives FDA Approval Across 2 TNBC Indications. cancernetwork.com. June 2026.
OncLive: ASCENT-04 primary analysis and Dr. Tolaney commentary: Dr Tolaney on the FDA Approval of First-Line Sacituzumab Govitecan Plus Pembrolizumab for TNBC. onclive.com. June 2026.
ASCENT-03 primary NEJM publication: Cortés J et al. Sacituzumab Govitecan in Untreated, Advanced Triple-Negative Breast Cancer. New England Journal of Medicine. 2025. doi:10.1056/NEJMoa2511734.
ASCENT-03 ESMO 2025 abstract (LBA20): Cortés JC et al. Primary results from ASCENT-03. Presented at ESMO Congress 2025. October 19, 2025. Berlin, Germany.
ASCENT-03 trial registration: NCT05382299. ClinicalTrials.gov.
ASCENT-04 primary NEJM publication: Tolaney SM et al. Sacituzumab govitecan plus pembrolizumab in first-line PD-L1-positive TNBC. NEJM. 2025. doi:10.1056/NEJMoa2511736.
ASCENT-04 trial registration: NCT05382286. ClinicalTrials.gov.
ASCENT-04 PFS2 and subsequent therapy data: Kalinsky K et al. PFS2 and subsequent therapies in ASCENT-04. ASCO 2026.
ADC mechanism and Trop-2 biology: Antibody-Drug Conjugates in Cancer Therapy. PMC7734386.
Sacituzumab govitecan StatPearls: Sacituzumab Govitecan. StatPearls. NCBI.
TNBC overview: Triple-Negative Breast Cancer. StatPearls. NCBI.
Pembrolizumab plus chemo TNBC approval (KEYNOTE-522): FDA approves pembrolizumab for triple-negative breast cancer. FDA.gov.
ACS TNBC overview: Triple-Negative Breast Cancer. cancer.org.
Patient resources: National Breast Cancer Foundation | Susan G. Komen Foundation | TOUCH, The Black Breast Cancer Alliance | Gilead Trodelvy patient support
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice. Trodelvy (sacituzumab govitecan-hziy) carries a boxed warning for severe neutropenia and severe diarrhea. Treatment decisions for metastatic TNBC, including the choice between monotherapy and combination regimens and the role of PD-L1 testing in treatment planning, should be made in close collaboration with a board-certified medical oncologist experienced in breast cancer management. |
|---|
Leave a Reply