| 📌 The essentials On May 27, 2026, the FDA approved Decnupaz (pivekimab sunirine-pvzy, AbbVie) for adults with blastic plasmacytoid dendritic cell neoplasm (BPDCN), an ultra-rare and aggressive hematologic malignancy. This is the second FDA-approved therapy for BPDCN and the first CD123-directed antibody-drug conjugate to receive FDA approval. Decnupaz is a first-in-class agent approved for both treatment-naive and relapsed or refractory BPDCN, making it applicable across all lines of therapy. Regulatory designations: Breakthrough Therapy Designation, Orphan Drug Designation, Priority Review. The clinical basis: Phase 1/2 CADENZA trial (NCT03386513), 84 adult patients (33 treatment-naive, 51 relapsed or refractory), open-label, single-arm. Primary endpoint: complete remission or clinical complete remission (CR/CRc) rate. Treatment-naive: 69.7% CR/CRc rate (95% CI 51.3 to 84.4%) at 21.5 months median follow-up; median duration of CR/CRc 9.7 months. Relapsed or refractory: 15.7% CR/CRc rate (95% CI 7.0 to 28.6%) at 24.1 months median follow-up; median duration of CR/CRc 9.2 months. Bridging to transplant: 39.4% of treatment-naive patients proceeded to post-study stem cell transplantation, a critical finding in a disease where bridging to transplant is a primary treatment goal. Boxed warning: hepatotoxicity including hepatic veno-occlusive disease (VOD). Dosing: 0.045 mg/kg intravenously over 15 to 30 minutes once every 3 weeks (21-day cycle). |
|---|
There are diseases that most physicians will never see in a career, not because they are mild or easily ignored, but because they are so rare that the entire diagnosed population in the United States numbers in the hundreds per year. Blastic plasmacytoid dendritic cell neoplasm is one of them.
BPDCN is an aggressive blood cancer that arises from plasmacytoid dendritic cell precursors, presenting most often in older adults as skin lesions combined with bone marrow involvement and sometimes rapid spread to other organs. It carries a historically poor prognosis: median overall survival in historical series without transplantation has ranged from 8 to 14 months. The only previously approved targeted therapy for BPDCN was tagraxofusp (Elzonris), a CD123-directed cytotoxin approved in 2018, leaving a significant gap particularly in the relapsed and refractory setting.
On May 27, 2026, the FDA approved Decnupaz (pivekimab sunirine-pvzy), a first-in-class CD123-directed antibody-drug conjugate developed by AbbVie (originally by ImmunoGen before AbbVie’s 2024 acquisition), for adult patients with BPDCN in both treatment-naive and relapsed or refractory settings. The approval is based on the CADENZA trial, which enrolled 84 patients across a disease population so rare that the trial itself represents one of the largest BPDCN clinical datasets ever assembled.
What BPDCN Is and Why It Is So Difficult to Treat
The cell of origin
BPDCN arises from the malignant transformation of plasmacytoid dendritic cell precursors, a rare subset of immune cells that normally circulate in blood and reside in lymphoid tissues. Plasmacytoid dendritic cells (pDCs) are specialized innate immune cells responsible primarily for producing large quantities of type I interferons in response to viral infection. In BPDCN, these precursors undergo malignant transformation and proliferate in a manner that is neither classically leukemic nor typically lymphomatous but shares features of both.
The disease was historically confusing to classify, previously known as agranular CD4+ CD56+ hematodermic neoplasm or blastic NK-cell lymphoma before its origin from pDC precursors was established. Its current classification as a distinct entity in the World Health Organization classification of hematologic malignancies reflects this now-understood biology.
Clinical presentation and typical course
BPDCN presents most commonly in adults over 60, with a strong male predominance (approximately 3:1 male-to-female ratio). The hallmark presentation is cutaneous involvement: bruise-like or reddish-brown skin lesions, nodules, or widespread plaques that can be widespread on the body surface. Bone marrow involvement is present in most patients at diagnosis, and peripheral blood involvement (leukemic phase) develops in many. The liver, spleen, and lymph nodes are other common sites.
An important clinical complexity is that BPDCN frequently presents concurrently with or evolves from other hematologic malignancies, including chronic myelomonocytic leukemia (CMML), myelodysplastic syndromes (MDS), and other myeloid neoplasms. In the CADENZA trial, 11 of the 33 treatment-naive patients had prior or concurrent cancer diagnoses in addition to BPDCN, reflecting real-world disease complexity.
Disease progression is typically rapid. Without effective treatment, the course from initial presentation to systemic organ involvement can be weeks to months.
| The CD123 target: why BPDCN is uniquely susceptible CD123, the interleukin-3 receptor alpha chain (IL-3Rα), is a cell surface protein that is highly and consistently overexpressed on BPDCN cells across virtually all patients with the disease. IL-3 signaling through CD123 promotes the survival and proliferation of pDC precursors, and in BPDCN, this overexpression is not incidental but functionally important to the malignant cell’s biology. The near-universal CD123 overexpression in BPDCN makes it one of the best-matched malignancies for CD123-targeted therapy of any cancer type. Both approved BPDCN therapies, tagraxofusp and now Decnupaz, exploit this target. The CADENZA trial required CD123 positivity confirmed by flow cytometry or immunohistochemistry for enrollment, ensuring that all patients in the trial had the target expression pattern needed for the drug to work. |
|---|
How Decnupaz Works: A First-in-Class ADC Mechanism
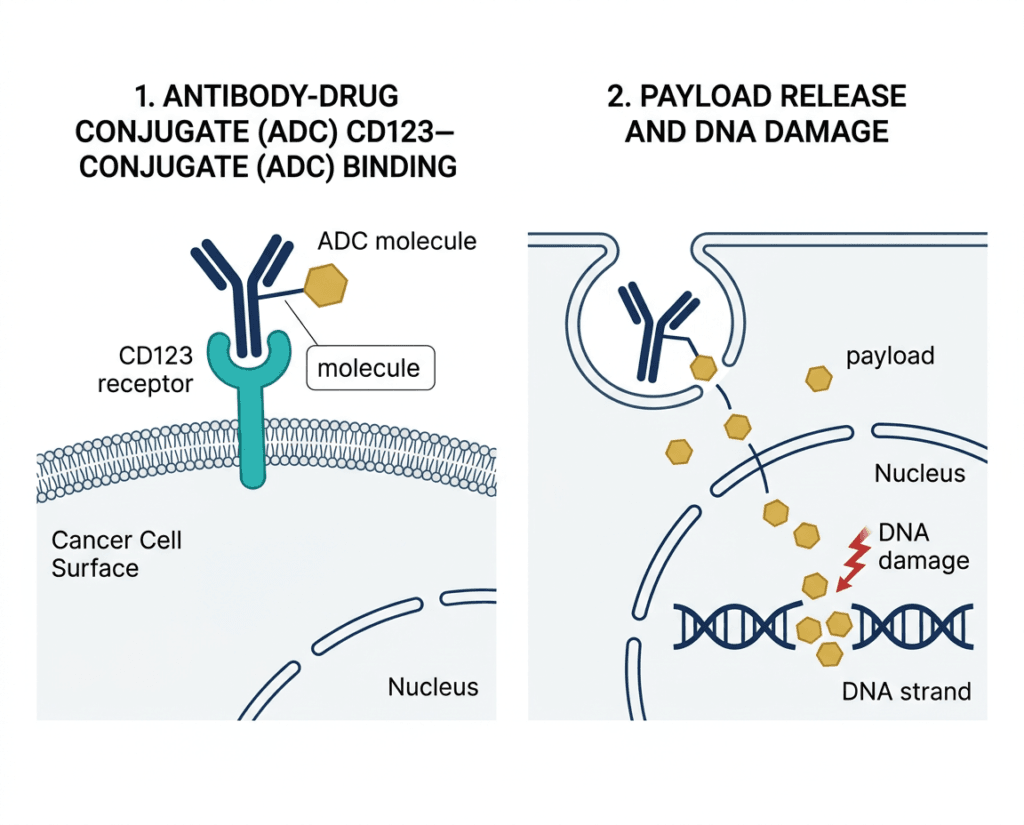
Decnupaz (pivekimab sunirine-pvzy) is an antibody-drug conjugate (ADC) with three distinct components:
The antibody: A high-affinity anti-CD123 monoclonal antibody that binds specifically to CD123 expressed on BPDCN cells. When the antibody binds CD123, the drug-receptor complex is internalized into the cell.
The linker: A cleavable linker that connects the antibody to the payload. After internalization, the linker is cleaved by intracellular enzymes, releasing the active payload inside the cancer cell.
The payload: An indolinobenzodiazepine pseudodimer (IGN), a potent DNA alkylating agent that alkylates DNA and causes single-strand DNA breaks without crosslinking. The mechanism of single-strand DNA damage without crosslinking is pharmacologically distinct from conventional alkylating chemotherapy, which typically crosslinks DNA. This distinction is designed to produce cytotoxicity in the targeted cancer cells while limiting some of the toxicity patterns associated with conventional alkylators.
This mechanism is what makes pivekimab sunirine a first-in-class agent: no previously approved drug uses an indolinobenzodiazepine pseudodimer payload in an ADC. The combination of the CD123-targeting antibody with this specific payload represents a novel mechanistic approach to BPDCN treatment.
Decnupaz differs from tagraxofusp in mechanism: tagraxofusp is a CD123-directed cytotoxin that consists of IL-3 fused to truncated diphtheria toxin, producing cell killing through a protein synthesis inhibition mechanism. Decnupaz delivers a DNA-damaging payload via ADC technology, offering a different mechanism of action for patients who have failed or cannot receive tagraxofusp.
The CADENZA Trial: Full Results
Design
CADENZA (NCT03386513) is a multicenter, open-label, single-arm Phase 1/2 trial that enrolled adults aged 18 and older with BPDCN with CD123 positivity confirmed by flow cytometry or immunohistochemistry and no evidence of active central nervous system disease. Two distinct cohorts were enrolled:
- Treatment-naive BPDCN (n=33): patients with no prior BPDCN-directed systemic therapy
- Relapsed or refractory BPDCN (n=51): patients who had received at least one prior line of therapy
The primary efficacy endpoint was the rate of complete remission (CR) or clinical complete remission (CRc). CR was defined as complete resolution of all BPDCN manifestations with full hematologic recovery. CRc was defined as complete resolution of all BPDCN manifestations with incomplete hematologic recovery (analogous to the CRi designation used in AML).
Primary endpoint results: treatment-naive cohort
| Outcome | Treatment-naive BPDCN (n=33) |
|---|---|
| CR/CRc rate | 69.7% (95% CI 51.3 to 84.4%) |
| Number of patients achieving CR/CRc | 23 of 33 |
| Median follow-up | 21.5 months |
| Median duration of CR/CRc | 9.7 months (95% CI 2.9 to not estimable) |
| Patients proceeding to post-study stem cell transplantation | 39.4% (13 of 33) |
| Median overall survival (all treatment-naive, n=33) | 16.6 months (95% CI 11.4 to not reached) |
| 12-month OS rate | 64% (95% CI 44.9 to 77.5%) |
| 18-month OS rate | 44% (95% CI 26.7 to 60.3%) |
Primary endpoint results: relapsed or refractory cohort
| Outcome | Relapsed or refractory BPDCN (n=51) |
|---|---|
| CR/CRc rate | 15.7% (95% CI 7.0 to 28.6%) |
| Number of patients achieving CR/CRc | 8 of 51 |
| Median follow-up | 24.1 months |
| Median duration of CR/CRc | 9.2 months (range 2.7 to 27.6 plus months) |
Source: CADENZA trial, NCT03386513. FDA approval notice, May 27, 2026. OncLive and Targeted Oncology clinical coverage.
The transplant bridge finding: the most clinically important secondary result
In the treatment-naive cohort, 39.4% of patients (13 of 33) proceeded to post-study stem cell transplantation after achieving response with Decnupaz. This finding is critically important in BPDCN because allogeneic stem cell transplantation is the only treatment approach associated with potential long-term cure in this disease. The primary role of induction therapy in BPDCN is often conceptualized as achieving a remission deep enough to bridge the patient to transplant while they remain in adequate condition to tolerate it.
A CR/CRc rate of 69.7% in treatment-naive patients, with 39.4% successfully bridging to transplant, represents a meaningful clinical achievement for a disease where achieving remission adequate for transplant eligibility has historically been extremely difficult.
The durability finding in the relapsed or refractory cohort also deserves specific attention: the median CR/CRc duration of 9.2 months in heavily pretreated patients, in a setting where overall response rates are low (15.7%), means that the patients who do respond achieve durable remissions comparable in length to those seen in the treatment-naive setting. This suggests that the drug’s mechanism produces meaningful responses when it works, across disease stages.
| Why single-arm trial data is accepted for ultra-rare cancer approvals BPDCN affects an estimated 500 to 1,000 patients per year in the United States. Running a randomized controlled trial with a placebo or active comparator arm in a disease this rare would take many years of enrollment, during which patients in the control arm would face disease progression without the study drug. The FDA routinely accepts single-arm evidence for ultra-rare malignancies when: the disease has an established and poor natural history; the effect size (here, 69.7% CR/CRc versus historical rates well below this) is large enough to be interpretable without a concurrent control; and adequate regulatory designations (Breakthrough, Orphan) are in place. The CADENZA approval follows this same logic used for tagraxofusp in 2018 and for multiple other ultra-rare cancer approvals. The absence of a randomized comparator reflects the rarity of the disease, not a weakness in the evidence standard applied. |
|---|
Safety: What the Prescribing Information Covers
Boxed warning: hepatotoxicity including hepatic veno-occlusive disease
Decnupaz carries a boxed warning for hepatotoxicity, including hepatic veno-occlusive disease (VOD), also called sinusoidal obstruction syndrome. VOD is a serious condition in which small hepatic veins are obstructed, causing liver damage that can range from mild and self-limiting to severe and fatal. It is a recognized complication of certain chemotherapy regimens and stem cell transplantation conditioning and can be life-threatening when severe.
The boxed warning means:
- Liver function tests must be monitored before each dose and as clinically indicated throughout treatment
- Dose modifications or discontinuation are required for significant hepatotoxicity
- Patients proceeding to stem cell transplantation after Decnupaz require careful management of VOD risk in the transplant setting
Warnings and precautions
Infusion-related reactions (IRRs): Infusion-related reactions occurred in clinical trials. Patients should be premedicated per the prescribing information before each infusion and monitored throughout administration. For severe reactions, the infusion should be stopped and not restarted.
Edema: Fluid retention and edema are documented with CD123-targeted therapies in BPDCN. Monitor for new or worsening edema, particularly in patients with baseline cardiac or renal disease.
Sulfite allergic reactions: Decnupaz contains sodium metabisulfite, which can cause allergic-type reactions including anaphylaxis and bronchospasm in susceptible individuals. The risk is higher in patients with asthma. Patients should be asked about sulfite sensitivity before initiating therapy.
Embryo-fetal toxicity: Based on the mechanism of action (DNA alkylation), Decnupaz can cause fetal harm. Females of reproductive potential should use effective contraception during treatment and for at least 6 months after the final dose. Males with female partners of reproductive potential should use effective contraception during treatment and for at least 4 months after the final dose.
Dosing and Administration
| Parameter | Details |
|---|---|
| Dose | 0.045 mg/kg intravenously once every 3 weeks (21-day cycle) |
| Infusion duration | Approximately 15 to 30 minutes |
| Dose calculation | Based on actual body weight |
| Cycles | Continue until disease progression or unacceptable toxicity |
| Formulation | Lyophilized cake for injection; requires reconstitution prior to administration |
| Premedication | Per prescribing information; required before each infusion |
What This Approval Means in Context
Decnupaz vs. tagraxofusp
Decnupaz is the second approved therapy for BPDCN. Tagraxofusp (Elzonris), approved in 2018, remains the reference treatment for newly diagnosed BPDCN and demonstrated an overall response rate of 90% in treatment-naive patients in its pivotal trial. However, tagraxofusp carries a boxed warning for capillary leak syndrome, a serious and potentially life-threatening vascular complication that limits its use in some patients.
Decnupaz offers a mechanistically distinct option across both treatment-naive and relapsed settings, with a different toxicity profile. No head-to-head comparison between tagraxofusp and Decnupaz exists; the choice between them in the treatment-naive setting will depend on institutional experience, patient-specific factors including comorbidities that affect tolerance of each product’s boxed warning risks, and the treating hematologist’s clinical judgment.
The approval of Decnupaz for relapsed or refractory disease is particularly significant because tagraxofusp’s pivotal data was primarily in the treatment-naive setting, and until now there has been no approved targeted therapy specifically for patients who have progressed after first-line treatment.
The AbbVie acquisition context
Pivekimab sunirine was originally developed by ImmunoGen, Inc., a company that pioneered ADC technology and developed multiple ADCs including mirvetuximab soravtansine (Elahere) for ovarian cancer. In early 2024, AbbVie acquired ImmunoGen for approximately $10.1 billion, a transaction that included pivekimab sunirine in the pipeline. The BLA for Decnupaz was submitted to the FDA in September 2025 and approved May 27, 2026.
For Patients and Clinicians
For patients diagnosed with BPDCN
BPDCN is rare enough that most patients will be referred to specialized hematology centers with experience in this disease shortly after diagnosis. Treatment decisions for BPDCN, including the choice between Decnupaz and tagraxofusp in treatment-naive disease, and whether to pursue stem cell transplantation, belong with a board-certified hematologic oncologist familiar with this specific diagnosis.
Decnupaz is now an FDA-authorized option for adults with BPDCN in any line of therapy. For patients who have relapsed after prior treatment, including tagraxofusp, this is the first approved targeted therapy available in that setting.
The Leukemia and Lymphoma Society (LLS) and NORD maintain current clinical information on BPDCN including specialist referral resources. For clinical trial opportunities, ClinicalTrials.gov lists currently enrolling studies for BPDCN. AbbVie’s patient support program provides access resources for Decnupaz at abbvie.com/BPDCN.
For related HED coverage of other ADC approvals and hematologic malignancy treatment advances in 2026, see our post on Inqovi plus venetoclax, the first all-oral AML regimen for treatment-ineligible patients, and our post on the Immgolis biosimilar approval and the TNF inhibitor market for autoimmune conditions.
Sources
FDA approval announcement: FDA approves pivekimab sunirine-pvzy for blastic plasmacytoid dendritic cell neoplasm, an ultra-rare hematologic malignancy. FDA.gov. May 27, 2026.
AbbVie press release: AbbVie Announces FDA Approval of Decnupaz (pivekimab sunirine-pvzy) for the Treatment of Blastic Plasmacytoid Dendritic Cell Neoplasm. abbvie.com. May 27, 2026.
Drugs.com approval news: FDA Approves Decnupaz (pivekimab sunirine-pvzy) for the Treatment of Blastic Plasmacytoid Dendritic Cell Neoplasm. drugs.com. May 27, 2026.
ASCO Post clinical summary: BPDCN: FDA Approves Pivekimab Sunirine-pvzy. ascopost.com. May 2026.
CancerNetwork detailed coverage: FDA Approves Pivekimab Sunirine in Rare Hematologic Malignancy. cancernetwork.com. May 2026.
Targeted Oncology full trial summary: FDA Approves Pivekimab Sunirine for BPDCN. targetedonc.com. May 2026.
OncLive OS data coverage: FDA Approves Pivekimab Sunirine for Blastic Plasmacytoid Dendritic Cell Neoplasm. onclive.com. May 2026.
ONS clinical summary: FDA Approves Pivekimab Sunirine-Pvzy for Blastic Plasmacytoid Dendritic Cell Neoplasm. ons.org. May 2026.
CURE magazine coverage: FDA OKs Decnupaz for Adults With Blastic Plasmacytoid Dendritic Cell Neoplasm. curetoday.com. May 2026.
Medscape coverage: FDA Approves Novel Targeted Therapy for Rare Blood Cancer. medscape.com. May 2026.
CADENZA trial registration: NCT03386513. ClinicalTrials.gov.
Tagraxofusp FDA approval (reference): FDA approves tagraxofusp-erzs for blastic plasmacytoid dendritic cell neoplasm. FDA.gov. 2018.
BPDCN disease overview: Blastic Plasmacytoid Dendritic Cell Neoplasm. StatPearls. NCBI.
BPDCN GARD overview: Blastic Plasmacytoid Dendritic Cell Neoplasm. rarediseases.info.nih.gov.
Hepatic VOD reference: Hepatic Veno-Occlusive Disease. PMC6016375.
ADC overview: Antibody-Drug Conjugate. cancer.gov.
Breakthrough Therapy Designation: Breakthrough Therapy. FDA.gov.
Orphan Drug Designation: Designating an Orphan Product. FDA.gov.
AbbVie acquisition of ImmunoGen: AbbVie Completes Acquisition of ImmunoGen. abbvie.com.
Patient resources: Leukemia and Lymphoma Society: BPDCN | NORD: BPDCN | NIH GARD: BPDCN | ClinicalTrials.gov: BPDCN
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. BPDCN is an ultra-rare malignancy requiring specialist care. Treatment decisions should be made in close consultation with a board-certified hematologic oncologist with experience in rare blood cancers. |
|---|
Leave a Reply