| 📌 The essentials On June 12, 2026, the FDA approved Ambelvist (gadoquatrane, Bayer) for use with MRI to detect and visualize lesions with abnormal vascularity in the central nervous system (brain, spine, and associated tissues) and the body (head and neck, thorax, abdomen, pelvis, and musculoskeletal system) in adult and pediatric patients, including term neonates. What makes it distinctive: gadoquatrane is a next-generation macrocyclic gadolinium-based contrast agent (mGBCA) with a novel tetrameric structure that achieves high image quality at substantially reduced gadolinium doses. With this approval, Ambelvist becomes the lowest-dose macrocyclic GBCA approved in the United States. Recommended dose: 0.01 mmol/kg actual body weight, which delivers 0.04 mmol Gd/kg body weight. This represents 60% less gadolinium than the standard macrocyclic GBCAs dosed at 0.1 mmol Gd/kg body weight, and 20% less gadolinium than gadopiclenol (Vueway), which delivers 0.05 mmol Gd/kg. The clinical basis: Phase 3 QUANTI program (three studies: QUANTI CNS, QUANTI OBR, and QUANTI Pediatric), 808 patients including 93 children, across 15 countries. QUANTI CNS and QUANTI OBR were randomized, double-blind, active-comparator crossover trials. Key results: gadoquatrane met the primary endpoint of non-inferiority to comparator mGBCAs (gadobutrol, gadoterate, gadoteridol) in visualization parameters and lesion detection using 60% less gadolinium. Post-contrast MRI with gadoquatrane was superior to unenhanced MRI alone. In descriptive analyses, visualization scores and lesion counts per blinded independent reader were comparable to comparator mGBCAs dosed at 0.1 mmol Gd/kg. No new safety signals. Boxed warnings: intrathecal administration risk; nephrogenic systemic fibrosis (NSF). Contraindicated in patients with a history of severe hypersensitivity reactions to gadoquatrane. |
|---|
Every year, more than 40 million MRI examinations with contrast are performed in the United States. The contrast agents used in the majority of those scans are gadolinium-based, and they are among the most important diagnostic tools in modern medicine. They light up tumors, strokes, vascular malformations, inflammatory lesions, and infections in brain tissue, spinal cord, joints, liver, and virtually every region of the body, making otherwise invisible pathology visible and informing clinical decisions that affect surgical planning, treatment selection, and disease monitoring.
Gadolinium-based contrast agents are also, as the FDA has required to be prominently stated in prescribing information since 2017, associated with gadolinium retention: gadolinium is retained for months or years in several organs, including the brain, even in patients with normal kidney function. The clinical significance of that retention in patients without renal impairment has not been definitively established, but the concern is real enough that the FDA, the American College of Radiology, and radiological societies worldwide have consistently encouraged the use of the lowest gadolinium dose that provides the necessary diagnostic information.
Ambelvist (gadoquatrane, Bayer), approved June 12, 2026, is the first MRI contrast agent to reach that lowest-dose standard among the macrocyclic class in the United States. Its novel tetrameric molecular structure achieves high image quality at 60% less gadolinium than standard macrocyclic agents, and clinical trial data demonstrated equivalent diagnostic performance to comparator agents dosed at 2.5 times the gadolinium content.
This post covers what gadolinium-based contrast agents do and why gadolinium retention matters, how gadoquatrane’s tetrameric structure produces high-quality imaging at lower gadolinium doses, what the QUANTI Phase 3 program showed, what the safety profile means in practice, and where Ambelvist fits in the current MRI contrast landscape.
What Gadolinium-Based Contrast Agents Do and Why Gadolinium Retention Is a Clinical Concern
How contrast-enhanced MRI works
MRI produces images by detecting the radiofrequency signals emitted by hydrogen nuclei (protons) in water and fat molecules as they return to equilibrium after being excited by a magnetic field and radiofrequency pulses. The speed of that return, characterized by relaxation times called T1 and T2, varies across different tissue types and creates the intrinsic contrast that makes MRI valuable even without exogenous contrast agents.
Gadolinium-based contrast agents (GBCAs) enhance this further. Gadolinium (Gd) is a paramagnetic metal ion that shortens the T1 relaxation time of nearby water protons, causing tissues that take up the contrast agent to appear brighter on T1-weighted MRI sequences. The enhancement is selective: gadolinium distributes into tissues with abnormal vascularity or disrupted blood-brain barrier, which is precisely the characteristic of tumors, inflammatory lesions, abscesses, demyelinating plaques, and vascular malformations. Normal brain parenchyma is protected by an intact blood-brain barrier and does not enhance.
This is why contrast-enhanced MRI is so diagnostically powerful: the gadolinium signal provides a spatial map of pathological vascular abnormality superimposed on the exquisite anatomical detail of the unenhanced MRI sequence.
Why gadolinium retention matters
Since the first GBCA was introduced in 1988, these agents have generally been considered safe for patients with normal renal function. That perception began to evolve in 2006 when nephrogenic systemic fibrosis (NSF), a serious and potentially fatal fibrosing condition, was firmly linked to GBCA administration in patients with severely impaired renal function. NSF is now largely eliminated through screening practices and the preferential use of more stable macrocyclic GBCAs over less stable linear agents.
A separate and distinct concern emerged around 2014 when researchers identified gadolinium deposition in brain tissue in patients with normal renal function who had received multiple GBCA-enhanced MRI scans. Signal changes in the dentate nucleus and globus pallidus on T1-weighted MRI were found to correlate with cumulative gadolinium exposure. This deposition occurs with all GBCAs but is substantially greater with linear agents than with macrocyclic agents. At equivalent doses, macrocyclic GBCAs show the lowest and most similar retention profiles among all GBCA classes, because their cyclic molecular cage structure holds gadolinium more tightly and releases it less readily than the open-chain structure of linear agents.
The clinical consequences of gadolinium deposition in the brain of patients with normal renal function have not been definitively established, but the regulatory response has been clear: minimize gadolinium dose while preserving diagnostic quality. The ACR Manual on Contrast Media recommends using the lowest gadolinium dose necessary to provide adequate diagnostic information.
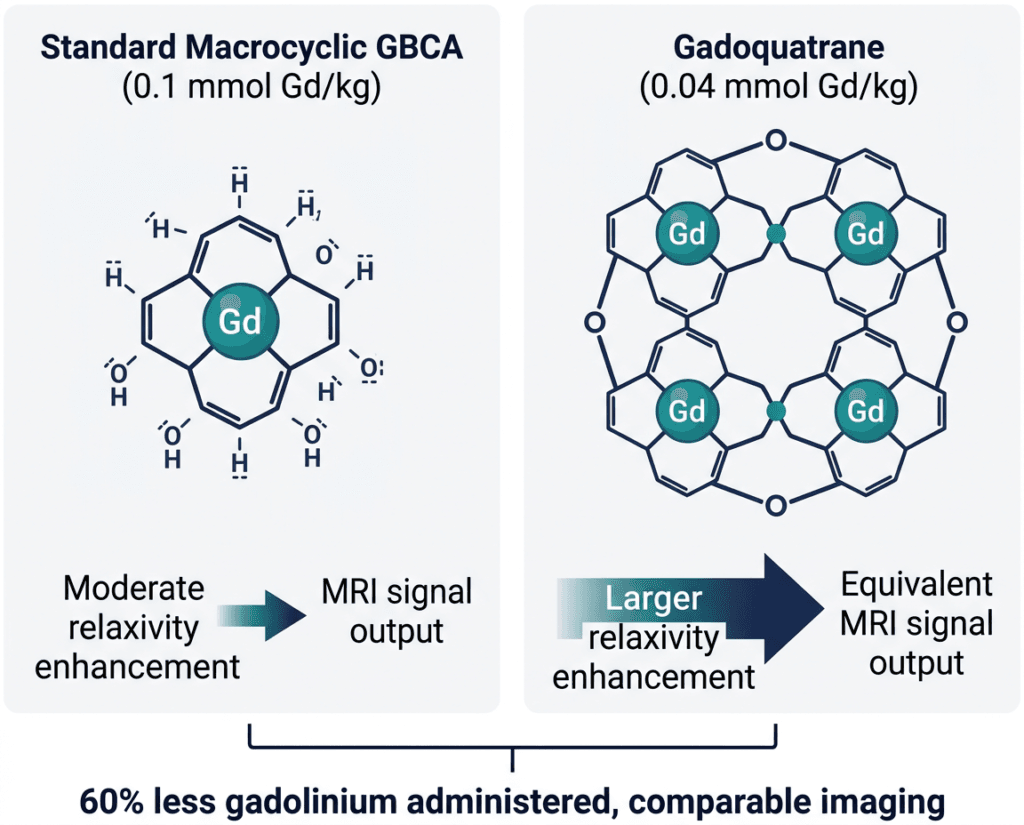
| The gadolinium problem in plain terms Every dose of gadolinium-based contrast agent leaves some gadolinium behind in the body, including in the brain. The macrocyclic cage structure of agents like gadobutrol, gadoterate, and gadoteridol holds gadolinium more tightly, reducing this retention compared to linear agents. But even macrocyclic agents deposit some gadolinium at standard doses. The logical next step, which gadoquatrane’s development pursued, was to engineer a macrocyclic agent that achieves equivalent image quality using substantially less gadolinium. Less gadolinium administered means less gadolinium available for retention, regardless of the agent’s stability profile. The tetrameric structure of gadoquatrane was designed specifically to achieve this: four times the relaxivity enhancement per gadolinium atom, enabling a 60% dose reduction while maintaining comparable imaging performance. |
|---|
How Gadoquatrane Works: The Tetrameric Structure and High Relaxivity
The key to understanding why gadoquatrane can deliver equivalent diagnostic performance at 60% less gadolinium than standard macrocyclic agents lies in its molecular architecture.
Conventional GBCAs, including the macrocyclic agents gadobutrol (Gadavist), gadoterate (Dotarem), and gadoteridol (ProHance), are monomeric molecules: one gadolinium ion chelated by one organic ligand. The magnetic effect of a single gadolinium ion on surrounding water protons, measured as relaxivity, is determined by how efficiently the paramagnetic gadolinium shortens the T1 relaxation time of nearby water molecules in a given concentration and magnetic field strength.
Gadoquatrane has a tetrameric structure: four gadolinium-chelate units are covalently linked in a single molecular framework. This arrangement substantially increases the molecule’s relaxivity. Each gadoquatrane molecule carries four gadolinium ions, and the molecular size and tumbling rate created by this tetrameric architecture are optimized for more efficient interaction with surrounding water protons. The result is that each molecule of gadoquatrane produces greater T1 enhancement per unit of gadolinium than conventional monomeric GBCAs.
This higher relaxivity per gadolinium atom is what allows gadoquatrane to produce comparable image quality at a substantially reduced gadolinium dose. The principle is analogous to a more efficient engine producing the same power output from less fuel: the tetrameric architecture extracts more MRI signal enhancement per gadolinium ion administered.
Gadoquatrane retains the macrocyclic cage structure of the established macrocyclic agents, with each of the four gadolinium ions held within a macrocyclic ligand unit. This means gadoquatrane’s thermodynamic and kinetic stability properties, the characteristics that minimize gadolinium release and retention, are consistent with the macrocyclic class. The same structural feature that produces low gadolinium retention in gadobutrol and gadoterate is present in each of gadoquatrane’s four chelate units.
The QUANTI Clinical Program: Three Trials, 808 Patients, 15 Countries
Gadoquatrane’s FDA approval is based on the QUANTI clinical development program, which consisted of three trials designed to evaluate efficacy and safety across the full body scope of the approved indication.
Program design
QUANTI CNS (NCT05915702): A multinational, randomized, prospective, double-blind, active-comparator crossover Phase 3 trial in adult patients with known or suspected CNS pathologies (brain, spine, associated tissues) undergoing contrast-enhanced MRI. Patients received gadoquatrane at 0.01 mmol/kg body weight (delivering 0.04 mmol Gd/kg) in one crossover period and one of three comparator macrocyclic GBCAs (gadobutrol, gadoterate, or gadoteridol) at 0.1 mmol Gd/kg in the other period. The crossover design meant each patient served as their own control, strengthening the comparison.
QUANTI OBR (NCT05915728): The same design applied to non-CNS body regions (head and neck, thorax, abdomen, pelvis, musculoskeletal system) in adult patients.
QUANTI Pediatric: A separate study evaluating the pharmacokinetics and safety of gadoquatrane in pediatric patients from birth to below 18 years of age across all body regions. This study supported the pediatric indication, including term neonates.
In total, 808 patients including 93 children participated across 15 countries. All three trials investigated gadoquatrane at the same 0.04 mmol Gd/kg dose, which represents a 60% reduction compared to the 0.1 mmol Gd/kg dose used by standard macrocyclic GBCAs.
Primary and secondary endpoint results
The primary endpoints of QUANTI CNS and QUANTI OBR assessed visualization parameters (border delineation, internal morphology, and contrast enhancement) as rated by blinded independent readers comparing gadoquatrane-enhanced MRI to comparator-enhanced MRI.
| Outcome | Result |
|---|---|
| Primary endpoint: non-inferiority of gadoquatrane versus comparator mGBCAs in visualization parameters (CNS and body) | Met in both QUANTI CNS and QUANTI OBR |
| Key secondary endpoint: superiority of post-contrast MRI with gadoquatrane versus unenhanced MRI alone | Met: increased lesion visualization confirmed |
| Descriptive comparison: visualization scores and lesion counts per blinded independent reader | Gadoquatrane comparable to comparator mGBCAs dosed at 0.1 mmol Gd/kg |
| Secondary endpoints: sensitivity and specificity for lesion detection | Non-inferiority to comparator mGBCAs demonstrated |
| Pediatric pharmacokinetics | Pharmacokinetic behavior in children consistent with adult data; efficacy from adult data applicable to pediatric population |
| Overall safety profile (all ages) | Consistent with prior gadoquatrane data and macrocyclic GBCAs class; no new safety signals |
Source: Bayer press release, June 15, 2026. QUANTI CNS NCT05915702. QUANTI OBR NCT05915728. QUANTI CNS ECR 2025 presentation.
The crossover design is worth emphasizing for its evidentiary strength. Because each patient received both gadoquatrane and a comparator macrocyclic agent in separate MRI sessions (with blinded independent reading of all images), the comparison is unusually rigorous: the same patient’s pathology is being imaged with different agents, eliminating the patient-level variability that can confound parallel-group designs in imaging trials.
The pediatric finding that pharmacokinetic behavior of gadoquatrane in children is similar to that in adults allowed the FDA to establish pediatric efficacy through pharmacokinetic/pharmacodynamic bridging, a standard approach for contrast agents where it is not ethical or practical to run fully powered efficacy trials in all pediatric subpopulations.
Where Ambelvist Fits in the GBCA Landscape
The U.S. MRI contrast agent market in 2026 includes multiple approved GBCAs across the linear and macrocyclic classes, with recent additions specifically at lower doses:
| Agent | Class | Dose | Gd content | FDA approval |
|---|---|---|---|---|
| Gadobutrol (Gadavist, Bayer) | Macrocyclic | 0.1 mmol/kg | 0.1 mmol Gd/kg | 2011 |
| Gadoterate meglumine (Dotarem, Guerbet) | Macrocyclic | 0.1 mmol/kg | 0.1 mmol Gd/kg | 2013 |
| Gadoteridol (ProHance, Bracco) | Macrocyclic | 0.1 mmol/kg | 0.1 mmol Gd/kg | 1992 |
| Gadapentetate dimeglumine (Magnevist) | Linear | 0.1 mmol/kg | 0.1 mmol Gd/kg | 1988 |
| Gadopiclenol (Vueway, Bracco) | Macrocyclic | 0.05 mmol/kg | 0.05 mmol Gd/kg | 2022 |
| Gadoquatrane (Ambelvist, Bayer) | Macrocyclic | 0.01 mmol/kg | 0.04 mmol Gd/kg | June 2026 |
Gadopiclenol (Vueway), approved in 2022, was the first high-relaxivity macrocyclic GBCA to achieve reduced-dose approval in the U.S., delivering 0.05 mmol Gd/kg versus the standard 0.1 mmol Gd/kg used by earlier macrocyclic agents. Gadoquatrane extends this further, delivering 0.04 mmol Gd/kg, 20% less gadolinium than gadopiclenol and 60% less than standard macrocyclic agents.
The competitive distinction between Ambelvist and Vueway will be evaluated by radiologists based on imaging performance data, institutional formulary decisions, practical acquisition considerations, and any head-to-head data that emerges in the coming years. Neither drug has been compared directly to the other in a randomized trial; both have been compared to the same standard-dose macrocyclic agents.
For radiology departments and institutions with established ACR or local protocols encouraging minimum gadolinium dose, Ambelvist provides an additional option in the macrocyclic class with the lowest Gd dose approved in the U.S. For patients who undergo contrast-enhanced MRI repeatedly over years of disease monitoring, such as patients with multiple sclerosis, brain metastases, or chronic inflammatory conditions requiring serial imaging, the cumulative gadolinium dose reduction across many scans is the practical benefit.
Safety: What the Prescribing Information Covers
Ambelvist’s safety profile is consistent with the macrocyclic GBCA class, with the same class-level concerns that apply to all gadolinium-based contrast agents.
Boxed warnings:
Intrathecal administration: Gadolinium-based contrast agents are not approved for intrathecal injection, and accidental intrathecal administration has resulted in serious adverse reactions including seizures, cardiorespiratory arrest, and death. This is a class-wide warning for all GBCAs. Ambelvist must be administered intravenously only.
Nephrogenic systemic fibrosis (NSF): Ambelvist, like all approved GBCAs, carries a boxed warning for NSF, a serious, debilitating, and potentially fatal fibrosing disorder of the skin and other tissues that has been observed in patients with impaired elimination of GBCAs, primarily those with chronic, severe kidney disease. As a macrocyclic agent, gadoquatrane is classified in the lower-NSF-risk group (ACR Group II/III), but the class warning remains on the label. Screen patients for acute kidney injury or other conditions that may reduce renal clearance before administering any GBCA.
Contraindication:
Ambelvist is contraindicated in patients with a history of severe hypersensitivity reactions to gadoquatrane.
Warnings and precautions:
Hypersensitivity reactions: As with all GBCAs, acute allergic-type reactions ranging from mild (urticaria, pruritus) to severe (anaphylaxis, bronchospasm, cardiovascular collapse) can occur. These are uncommon but can be immediate or delayed. Assess patient allergy history before administration. Maintain resuscitation capability during administration.
Gadolinium retention: As described above, gadolinium is retained for months or years in the brain and other organs following GBCA administration. Linear GBCAs cause greater retention than macrocyclic GBCAs. At equivalent doses, retention is lowest and most similar among macrocyclic agents. The lower administered dose of gadoquatrane means less total gadolinium is available for potential retention compared to standard-dose macrocyclic agents. The clinical consequences of gadolinium retention in the brain of patients with normal renal function have not been established.
Acute kidney injury: GBCAs may increase the risk of acute kidney injury. Screen patients for reduced renal function before administration. In patients with chronic kidney disease, use the lowest dose necessary and avoid repeat dosing unless the diagnostic benefit clearly outweighs the risk.
Interference with lesion visualization: Certain lesion types may not enhance reliably with Ambelvist. Some lesions visible with other GBCA types may not be detectable with gadoquatrane at the approved dose. Blinded reading of MRI examinations should consider the dose and agent used.
Dosing:
Administered as an intravenous injection of 0.01 mmol/kg actual body weight (which delivers 0.04 mmol Gd/kg body weight). Ambelvist is supplied as a 0.1 mmol/mL solution in single-dose vials, single-dose prefilled syringes, imaging bulk packages, and pharmacy bulk packages.
What This Means for Patients Who Receive Contrast-Enhanced MRI
Most patients receiving contrast-enhanced MRI will not choose their contrast agent: the radiology department or ordering institution determines which agent to use based on formulary, protocol, and clinical judgment. What patients can do is understand why the conversation about gadolinium matters and ask informed questions about contrast use.
For patients who undergo contrast-enhanced MRI repeatedly, such as those with multiple sclerosis being monitored for disease activity, patients with brain metastases under treatment, and patients with chronic inflammatory conditions like Crohn’s disease requiring serial cross-sectional imaging, cumulative gadolinium exposure from repeated scans is the most relevant concern. Lower-dose agents at equivalent diagnostic performance represent a genuine clinical benefit for these populations over a lifetime of imaging.
For patients with chronic kidney disease, the NSF boxed warning is the priority concern. Any patient with significantly impaired renal function should discuss with their ordering physician whether contrast enhancement is necessary for their specific clinical question, and if so, which agent and dose minimize the NSF risk while providing the needed diagnostic information.
For patients undergoing a single diagnostic MRI as part of an acute clinical evaluation, such as evaluation for stroke, initial workup of a brain mass, or staging of a newly diagnosed cancer, the cumulative dose concern is less relevant. The diagnostic adequacy of the scan is the priority.
For clinicians and radiologists: the ACR Manual on Contrast Media, updated in 2026, provides the current framework for GBCA selection and dose minimization. Ambelvist’s addition to the macrocyclic formulary options gives departments a lowest-dose macrocyclic choice for protocols where gadolinium minimization is a priority alongside diagnostic adequacy.
For related HED coverage on neurological conditions commonly evaluated with contrast-enhanced MRI, see our post on Ocrevus (ocrelizumab) approved for pediatric relapsing-remitting MS and our post on the FDA’s acceleration of psychedelic drug programs for treatment-resistant depression and PTSD, the latter of which covers conditions where neuroimaging plays a growing role in clinical research.
Sources
Bayer FDA approval press release: Bayer’s AMBELVIST (gadoquatrane) Receives FDA Approval for Contrast-Enhanced MRI. BusinessWire. June 15, 2026.
Bayer Ambelvist page: AMBELVIST (gadoquatrane) FDA approval. bayer.com.
BioSpace approval coverage: Bayer’s Ambelvist Receives FDA Approval for Contrast-Enhanced MRI. biospace.com. June 15, 2026.
CancerNetwork clinical summary: FDA Approves Gadoquatrane to Detect CNS and Non-CNS Body Region Lesions. cancernetwork.com. June 2026.
Renal and Urology News coverage: FDA Approves Lower-Dose Gadolinium Contrast Agent Ambelvist. renalandurologynews.com. June 2026.
Neurology Advisor coverage: FDA Approves Lower-Dose Gadolinium Contrast Agent Ambelvist. neurologyadvisor.com. June 2026.
Axis Imaging News coverage: FDA Approves Bayer’s Low-Dose MRI Contrast Agent. axisimagingnews.com. June 2026.
QUANTI CNS Phase 3 topline results (Bayer/ECR 2025): Positive results from Phase III study for Bayer’s investigational contrast agent gadoquatrane. Bayer/BusinessWire. February 26, 2025.
QUANTI program pivotal topline results (all studies): Bayer’s investigational MRI contrast agent gadoquatrane meets primary and main secondary endpoints. BusinessWire. January 10, 2025.
QUANTI Pediatric (RSNA 2025): RSNA25: Pediatric Study for Bayer’s Investigational MRI Contrast Agent Gadoquatrane Meets Primary and Secondary Endpoints. biospace.com. December 2025.
QUANTI CNS trial registration: NCT05915702. ClinicalTrials.gov.
QUANTI OBR trial registration: NCT05915728. ClinicalTrials.gov.
Ambelvist prescribing information: AMBELVIST (gadoquatrane) Prescribing Information. Bayer. labeling.bayerhealthcare.com.
GBCA safety update (AJR): Update on Gadolinium-Based Contrast Agent Safety. AJR. doi:10.2214/AJR.23.30036.
Gadolinium retention brain review: MRI contrast agents and retention in the brain: review. PMC11282029.
Linear versus macrocyclic gadolinium CNS gene expression: Long-term effects of linear versus macrocyclic GBCAs on gene expression in CNS of mice. PMC11723877.
Gadolinium toxicity mechanisms review: Gadolinium toxicity: mechanisms, clinical manifestations, and nanoparticle role. PMC12454587.
NSF overview: Nephrogenic Systemic Fibrosis. StatPearls. NCBI.
ACR Manual on Contrast Media (2026): ACR Manual on Contrast Media. acr.org.
MRI overview: Magnetic Resonance Imaging. NIBIB.
Vueway (gadopiclenol) prescribing information (comparator reference): Vueway (gadopiclenol) package insert. Bracco.
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice. Ambelvist (gadoquatrane) carries a boxed warning for risks associated with intrathecal administration and nephrogenic systemic fibrosis. Decisions about contrast agent selection for MRI examinations are made by qualified radiologists and ordering clinicians based on the clinical question, patient characteristics, and institutional protocols. Patients with renal impairment should discuss the use of gadolinium-based contrast agents with their physician before undergoing contrast-enhanced MRI. |
|---|
Leave a Reply