| 📌 The essentials On June 17, 2026, the FDA approved Utebzi (tebipenem pivoxil, GSK/Spero Therapeutics) for the treatment of complicated urinary tract infections (cUTI), including pyelonephritis, caused by susceptible microorganisms in adult patients who have limited or no alternative oral treatment options. This is the first and only oral carbapenem antibiotic approved anywhere in the United States. Previously, every carbapenem available to U.S. clinicians required intravenous administration, meaning that patients with drug-resistant cUTIs requiring carbapenem-level coverage had no oral option and needed hospitalization, a peripherally inserted central catheter (PICC) line, or infusion center visits. Approved organisms: Escherichia coli, Klebsiella pneumoniae, Enterobacter cloacae species complex, Klebsiella oxytoca, and Enterococcus faecalis. The clinical basis: Phase 3 PIVOT-PO trial (NCT06059846), 1,690 hospitalized adults with cUTI or acute pyelonephritis, double-blind, randomized 1:1 oral tebipenem pivoxil versus intravenous imipenem-cilastatin. Trial stopped early for efficacy at interim analysis (May 2025). Primary endpoint: overall response (composite of clinical cure plus microbiological eradication) at test-of-cure visit. Result: 58.5% (261/446) with tebipenem pivoxil versus 60.2% (291/483) with IV imipenem-cilastatin (adjusted difference −1.3%; 95% CI −7.5% to 4.8%), meeting non-inferiority. ESBL-producing Enterobacterales subgroup: composite response 52.2% versus 56.8% with IV imipenem-cilastatin. Regulatory designations: Qualified Infectious Disease Product (QIDP), Fast Track. Regulatory history: GSK resubmitted the NDA in December 2025 after an earlier Complete Response Letter; PIVOT-PO data supported the resubmission. Dosing: 600 mg (two 300 mg tablets) orally every 6 hours for 7 to 10 days, with or without food. Important dosing limits: dose adjustment required for eGFR 15 to below 60 mL/min; use not recommended in patients with eGFR above 150 mL/min due to predicted reduced tebipenem exposure. |
|---|
For the past several decades, carbapenems have represented the antibiotic class of last resort in infectious disease medicine. When bacteria have developed resistance to penicillins, cephalosporins, and fluoroquinolones, carbapenems are frequently the agents that still work. They are critically important, routinely used in hospitalized patients with serious infections, and until June 17, 2026, every single carbapenem available in the United States required intravenous administration.
That meant something specific and consequential for patients with complicated urinary tract infections caused by multidrug-resistant organisms: no matter how well they felt, no matter how stable their condition, they needed a hospital bed, an IV line, or an outpatient infusion arrangement to receive the only effective treatment available to them. The United States has more than 3 million cUTI cases treated annually, and a substantial proportion involve organisms resistant to standard oral agents. For those patients, the arrival of an oral carbapenem is not a minor convenience. It is a clinically meaningful expansion of outpatient treatment options.
Utebzi (tebipenem pivoxil, GSK/Spero Therapeutics) was approved June 17, 2026, as the first oral carbapenem in the U.S. for cUTI in patients with limited or no alternative oral treatment options. The Phase 3 PIVOT-PO trial compared oral tebipenem pivoxil head-to-head against intravenous imipenem-cilastatin, the gold-standard IV carbapenem, and stopped early for efficacy. This post covers what complicated UTIs are, how carbapenems work and why an oral formulation required a novel prodrug approach, what PIVOT-PO data showed, what the regulatory backstory was, and what this approval means for patients and clinicians managing resistant gram-negative infections.
What Complicated Urinary Tract Infections Are and Why Drug Resistance Makes Them Harder to Treat
Complicated urinary tract infections are defined by the presence of structural or functional abnormalities in the urinary tract, or by host factors that impair the normal defenses against infection. They include pyelonephritis (kidney infection), infections associated with urinary catheters or stents, infections in patients with obstructive uropathy or neurogenic bladder, and infections in immunocompromised hosts. Unlike uncomplicated UTIs, which can typically be treated with short courses of oral antibiotics in otherwise healthy outpatient women, cUTIs require more intensive management, longer treatment courses, and often hospitalization.
The most common organisms causing cUTI are gram-negative Enterobacterales, principally E. coli and Klebsiella pneumoniae. These same organisms are at the center of one of the most serious antimicrobial resistance crises in contemporary medicine.
Extended-spectrum beta-lactamase (ESBL)-producing Enterobacterales have developed enzymes that inactivate most penicillins and cephalosporins. They are resistant to trimethoprim-sulfamethoxazole in many cases and frequently resistant to fluoroquinolones. In the PIVOT-PO trial, approximately 35 to 39% of Enterobacterales isolates in both arms were ESBL producers, reflecting the real-world prevalence of this resistance pattern in hospitalized patients with cUTI. For patients whose infection is caused by an ESBL-producing organism, the standard outpatient oral antibiotics (ciprofloxacin, trimethoprim-sulfamethoxazole, nitrofurantoin) are often not options. Until now, that left no oral carbapenem alternative.
Carbapenem-resistant Enterobacterales (CRE), which are resistant even to standard IV carbapenems, are designated by the CDC as an urgent threat. Utebzi’s approved indication specifically covers susceptible organisms, meaning it is not intended for CRE infections where even IV carbapenems would fail. Its value is in the ESBL-producing and fluoroquinolone-resistant Enterobacterales space, where it provides a first oral carbapenem-class option.
The Science: How Tebipenem Works and Why an Oral Carbapenem Required a Prodrug Approach
Carbapenem mechanism of action
Carbapenems belong to the beta-lactam antibiotic class, which also includes penicillins and cephalosporins. All beta-lactams share a core mechanism: they bind to penicillin-binding proteins (PBPs) in bacterial cell walls, inhibiting the transpeptidation reaction that cross-links the peptidoglycan strands that give the cell wall its structural integrity. Without proper peptidoglycan cross-linking, the bacterial cell wall cannot withstand osmotic pressure, the cell lyses, and the bacterium dies.
What distinguishes carbapenems from other beta-lactams is their stability against beta-lactamase enzymes. Most gram-negative bacteria that cause serious infections produce beta-lactamases, enzymes that hydrolyze the beta-lactam ring of penicillins and cephalosporins, rendering those antibiotics inactive. Carbapenems have a unique bicyclic structure that makes them resistant to the most common beta-lactamases, including ESBLs. This is why carbapenems remain active where penicillins and cephalosporins have failed, and it is the mechanistic basis for their clinical importance as last-resort antibiotics.
Tebipenem specifically exhibits broad-spectrum activity against gram-negative Enterobacterales by binding with high affinity to PBP2 and PBP3, the penicillin-binding proteins primarily responsible for cell wall elongation and septation during bacterial cell division. Its activity is bactericidal and is optimized against the organisms most commonly implicated in cUTI.
Why carbapenems were IV-only until now: the oral bioavailability problem
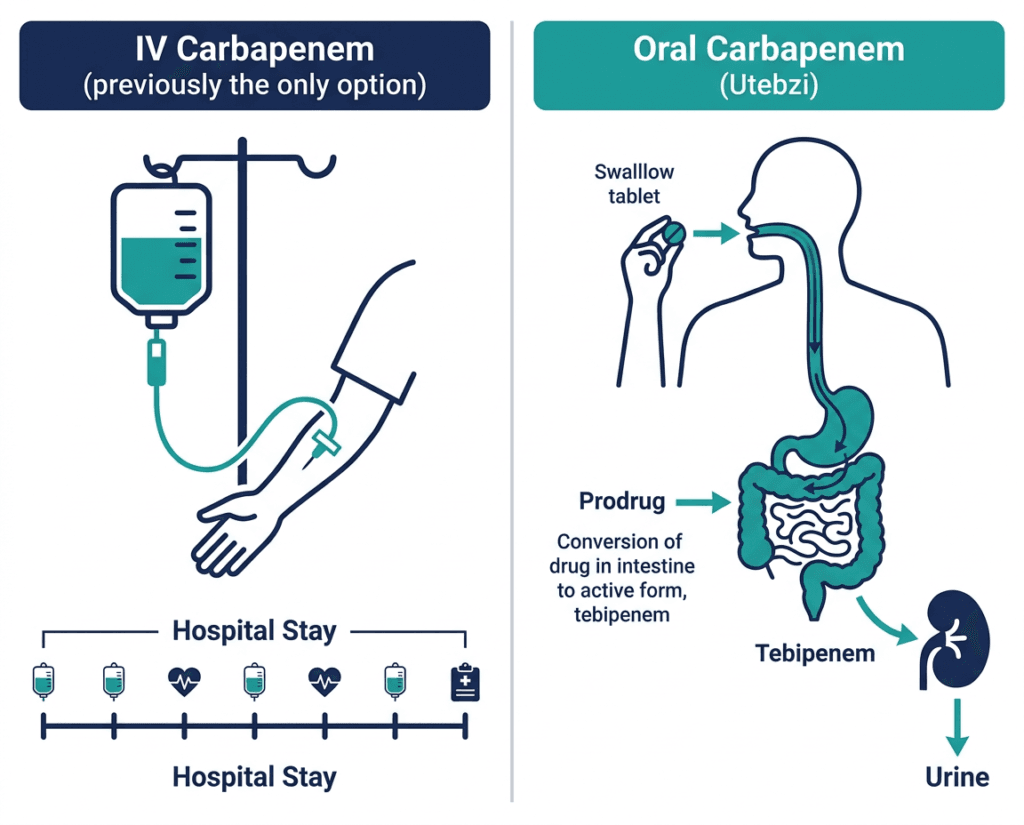
The reason all previously approved carbapenems required intravenous administration is oral bioavailability. Carbapenem molecules are hydrophilic (water-loving) and polar, characteristics that make them excellent at distributing through aqueous tissues but also make it difficult for them to cross the lipid-rich intestinal epithelium and reach the bloodstream when swallowed. Most carbapenem molecules taken orally would simply pass through the gut without being absorbed.
Tebipenem pivoxil solves this through a prodrug strategy. “Tebipenem pivoxil” is the prodrug form: the active carbapenem molecule tebipenem is chemically modified with a pivoxil ester group that makes the compound more lipophilic (fat-soluble) and significantly improves oral absorption across the intestinal epithelium. After absorption, intestinal esterases rapidly cleave the pivoxil ester, releasing the active tebipenem molecule into systemic circulation. The active tebipenem then distributes into renal tissue and urine, where it achieves the concentrations needed to kill the causative organisms.
This prodrug approach is the same chemical strategy used in several other orally administered antibiotics, most notably the cephalosporin prodrugs cefuroxime axetil and cefpodoxime proxetil, where ester modification similarly improves gut absorption of molecules that would otherwise be poorly bioavailable. For carbapenems, engineering this chemistry without compromising the stability of the beta-lactam ring and without producing a molecule with unfavorable pharmacokinetics was a substantial pharmaceutical development challenge.
| Why the pivoxil ester matters beyond oral bioavailability The pivoxil moiety that enables tebipenem’s oral absorption is the same group used in pivampicillin and pivmecillinam, and its hydrolysis releases pivalic acid as a byproduct. Pivalate can conjugate with carnitine and impair carnitine metabolism, particularly with long-term or repeated use. This class effect of pivoxil-containing antibiotics is relevant for patients receiving concurrent carnitine supplementation and for patients with carnitine metabolism disorders. The short course of Utebzi (7 to 10 days) limits this concern in most clinical settings, but it is worth noting as a mechanistic consideration of the prodrug chemistry. |
|---|
The PIVOT-PO Trial: Design and Full Results
Design
PIVOT-PO (NCT06059846) was a global, randomized, double-blind, non-inferiority Phase 3 trial enrolling 1,690 hospitalized adult patients with cUTI or acute pyelonephritis. The double-blind design was maintained using a double-dummy approach: patients in each arm received both an active oral tablet and a matching IV placebo, or an active IV infusion and a matching oral placebo tablet, maintaining blinding while comparing true oral versus true IV administration.
Randomization: 1:1 to:
- Tebipenem pivoxil 600 mg orally (two 300 mg tablets) every 6 hours for 7 to 10 days
- Imipenem-cilastatin 500 mg intravenously every 6 hours for 7 to 10 days (standard of care comparator)
Imipenem-cilastatin (Primaxin) was chosen as the comparator because it is a well-established IV carbapenem with robust efficacy data in cUTI, appropriate as the active reference standard for a non-inferiority comparison against an oral carbapenem.
Primary endpoint: Overall response at the test-of-cure (TOC) visit, defined as a composite of clinical cure plus microbiological eradication in the intent-to-treat (ITT) efficacy cohort.
The trial was stopped early for efficacy at a planned interim analysis in May 2025, indicating that the pre-specified criteria for early stopping based on demonstrated non-inferiority were met ahead of the planned full enrollment.
Primary endpoint results
| Outcome | Tebipenem pivoxil (oral) | Imipenem-cilastatin (IV) | Comparison |
|---|---|---|---|
| Overall response (clinical cure plus microbiological eradication) at TOC | 58.5% (261/446) | 60.2% (291/483) | Adjusted difference −1.3% (95% CI −7.5% to 4.8%) |
| Non-inferiority demonstrated | Yes | Reference | Lower CI bound within pre-specified margin |
Source: Spero Therapeutics/GSK press release. GlobeNewswire. June 17, 2026. PIVOT-PO NCT06059846. Presented at IDWeek 2025.
The adjusted difference of −1.3 percentage points, with a 95% confidence interval ranging from −7.5% to +4.8%, demonstrates that oral tebipenem pivoxil was non-inferior to intravenous imipenem-cilastatin in achieving the composite endpoint of clinical cure plus microbiological eradication. The upper bound of the confidence interval is positive (favoring oral tebipenem in the best-case scenario) and the lower bound remains within whatever non-inferiority margin was pre-specified. This is the evidentiary standard the FDA required to demonstrate that oral tebipenem delivers comparable efficacy to the IV comparator.
ESBL-producing pathogen subgroup
In the PIVOT-PO trial, 35.1% of Enterobacterales isolates in the tebipenem arm and 38.9% in the imipenem arm were ESBL producers, reflecting the real-world prevalence of ESBL-producing cUTI in hospitalized patients. Among patients infected with ESBL-producing organisms, the composite response rates at TOC were 52.2% with tebipenem pivoxil and 56.8% with IV imipenem-cilastatin. Comparable response rates were also observed among patients infected with fluoroquinolone-not-susceptible and trimethoprim-sulfamethoxazole-resistant Enterobacterales.
This subgroup data is clinically important because the ESBL-producing patient population represents precisely the group for whom no oral treatment was previously available. That composite response rates in this resistance-characterized subgroup were broadly consistent with the overall ITT population supports the use of tebipenem pivoxil specifically in these patients.
Safety in PIVOT-PO
The safety profile of tebipenem pivoxil was consistent with the carbapenem class. The most common adverse events were diarrhea and headache. Additional adverse events reported included mild to moderate nausea, abdominal pain, transaminase elevations, and Clostridioides difficile-associated diarrhea (CDAD), which is a class effect associated with broad-spectrum antibiotics. No new or unexpected safety signals were identified.
The Regulatory Backstory: A Prior CRL and the Path to Approval
The path to Utebzi’s June 2026 approval was not linear. GSK and Spero had submitted an earlier NDA for tebipenem pivoxil for cUTI, supported by a prior Phase 3 trial. That application received a Complete Response Letter from the FDA, which identified deficiencies that needed to be addressed before approval could be granted. The PIVOT-PO trial, which compared oral tebipenem directly against intravenous imipenem-cilastatin (a more demanding head-to-head non-inferiority design than the prior trial), was specifically designed and conducted to address the FDA’s concerns and generate the evidence package required for resubmission.
GSK filed the NDA resubmission in December 2025, supported by the PIVOT-PO data that had been presented at IDWeek 2025 weeks prior. The PDUFA date was set for June 18, 2026, and the FDA approved one day ahead of the deadline on June 17, 2026.
The tebipenem pivoxil program has received QIDP (Qualified Infectious Disease Product) designation and Fast Track designation from the FDA, both reflecting the agency’s recognition of the serious unmet need in drug-resistant cUTI.
Approved Organisms, Dosing, and Critical Prescribing Guidance
Approved organisms
Utebzi is approved for cUTI caused by the following susceptible organisms:
- Escherichia coli
- Klebsiella pneumoniae
- Enterobacter cloacae species complex
- Klebsiella oxytoca
- Enterococcus faecalis
Culture and susceptibility testing are essential before prescribing. Utebzi is indicated for organisms confirmed or strongly suspected to be susceptible. It is not effective against CRE (carbapenem-resistant Enterobacterales), and empiric use without culture data should be guided by institutional stewardship protocols and local epidemiology.
Dosing
| Parameter | Details |
|---|---|
| Standard dose | 600 mg (two 300 mg tablets) orally every 6 hours |
| Duration | 7 to 10 days |
| Administration | With or without food |
| Renal adjustment | Required for eGFR 15 to below 60 mL/min; consult full prescribing information for specific dose |
| eGFR above 150 mL/min | Use not recommended (predicted reduced tebipenem exposure may reduce efficacy; if necessary, monitor clinical response closely) |
| Not recommended | eGFR below 15 mL/min (end-stage renal disease without dialysis); data insufficient |
The eGFR above 150 mL/min restriction is an unusual and clinically notable prescribing caution. Patients with hyperfiltration (augmented renal clearance), which can occur in younger patients, pregnant patients, and critically ill patients with preserved kidney function, may clear tebipenem faster than typical patients, potentially reducing urinary drug concentrations below the threshold needed for bactericidal activity. This pharmacokinetic consideration is specific to a renally-excreted antibiotic being used for a urinary tract indication and should be considered when prescribing in patients whose renal function is known to be substantially above normal.
Antibiotic stewardship
Consistent with antimicrobial stewardship principles, Utebzi should be used only to treat infections proven or strongly suspected to be caused by susceptible bacteria. The approved labeling specifically addresses this: use should follow culture and susceptibility data whenever possible, and empiric use should be reserved for patients with strong clinical suspicion of a resistant organism based on prior culture history, risk factors, or local epidemiology.
What This Approval Means in Clinical Practice
Before June 17, 2026, a hospitalized patient with pyelonephritis caused by an ESBL-producing E. coli, who was otherwise stable and could be managed as an outpatient, had essentially no oral option. Every carbapenem required IV access. Sending such a patient home required either arranging home IV infusion (expensive, logistically complex, and uncomfortable for the patient) or keeping them in the hospital longer than their clinical condition strictly required (expensive and exposing them to hospital-acquired infection risk).
As Dr. Debra L. Fromer, MD, of Hackensack Meridian Health, explained: the advent of an oral carbapenem reduces the strain on the healthcare system by enabling earlier discharge and allowing outpatient treatment of patients who previously required hospitalization or PICC line placement. A pill taken at home every 6 hours is not identical in convenience to a once-daily oral antibiotic, but compared to an IV infusion it is transformative for appropriate patients.
The key phrase in the approved indication is “limited or no alternative oral treatment options.” Utebzi is not positioned as a first-line or empiric therapy for all cUTIs. It is a targeted option for the resistance gap: patients with culture-confirmed or highly suspected resistant organisms where standard oral agents have failed or are expected to fail. The approved patient population is specific, the culture requirement is clinical standard, and the antibiotic stewardship framing is appropriately conservative.
For patients with cUTI or recurrent UTI who are managing resistant infections: Utebzi is a prescription medication that requires a clinician experienced in managing complicated UTIs. The starting point for access is a discussion with a urologist, urogynecologist, or infectious disease specialist who can review culture results and determine whether tebipenem pivoxil is appropriate for the specific organism and clinical situation.
For related HED coverage on other resistant-organism antibiotic approvals in 2026, see our post on Zaynich (cefepime-zidebactam), the first antibiotic combination in which the beta-lactamase inhibitor also independently targets PBP2, approved for drug-resistant cUTI just weeks earlier.
Sources
FDA approval / GSK press release: Utebzi (tebipenem pivoxil) approved in the US for adults with complicated urinary tract infections. GSK. June 17, 2026.
Spero Therapeutics press release: Utebzi (tebipenem pivoxil) approved in the US for adults with complicated urinary tract infections. Spero Therapeutics/GlobeNewswire. June 17, 2026.
Drugs.com approval news: FDA Approves Utebzi (tebipenem pivoxil) for Adults with Complicated Urinary Tract Infections. drugs.com. June 17, 2026.
Utebzi approval history: Utebzi FDA Approval History. drugs.com.
Urology Times clinical coverage (with Dr. Fromer quote): FDA approves tebipenem pivoxil for complicated urinary tract infections. urologytimes.com. June 2026.
AJMC detailed trial coverage: FDA Approves First Oral Carbapenem Antibiotic for Complicated UTIs. ajmc.com. June 2026.
Renal and Urology News clinical summary: Utebzi Approved as First Oral Carbapenem Antibiotic for cUTIs. renalandurologynews.com. June 2026.
Contagion Live detailed coverage: FDA Approves Tebipenem Pivoxil as First Oral Carbapenem For Complicated Urinary Tract Infections. contagionlive.com. June 2026.
Contemporary OB/GYN clinical coverage: FDA approves tebipenem pivoxil as first oral carbapenem antibiotic for complicated urinary tract infections. contemporaryobgyn.net. June 2026.
PIVOT-PO trial registration: NCT06059846. ClinicalTrials.gov.
Complicated UTI overview: Complicated Urinary Tract Infections. StatPearls. NCBI.
Beta-lactam antibiotics and PBPs: Beta-Lactam Antibiotics. StatPearls. NCBI.
ESBL and beta-lactamases: Beta-Lactamase Inhibitors. PMC7279573.
Enterobacterales infections: Gram-Negative Bacterial Infections. StatPearls. NCBI.
C. diff associated diarrhea: Clostridioides Difficile. StatPearls. NCBI.
CRE threat designation: Antibiotic Resistance Threats in the United States. CDC.
Antibiotic stewardship core elements: Core Elements of Antibiotic Stewardship. CDC.
QIDP and GAIN Act: GAIN Act FAQ. FDA.gov.
Fast Track designation: Fast Track. FDA.gov.
CRL overview: FDA Drug Review Process. FDA.gov.
Utebzi prescribing information: UTEBZI (tebipenem pivoxil) Prescribing Information. GSK. 2026.
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Utebzi is a prescription antibiotic indicated specifically for adult patients with complicated urinary tract infections caused by susceptible organisms who have limited or no alternative oral treatment options. Antibiotic selection should be guided by culture and susceptibility data and made in consultation with a qualified healthcare provider. |
|---|
Leave a Reply