
| 📌 The essentials On May 29, 2026, the FDA approved Xocova (ensitrelvir, Shionogi) for post-exposure prophylaxis (PEP) of COVID-19 in adults and adolescents aged 12 years and older who have been exposed to an individual with COVID-19. This is the first and only oral therapy approved in the United States to help prevent COVID-19 after exposure. No previously approved treatment or prophylaxis option for post-exposure prevention of COVID-19 has existed in the United States. The clinical basis: Phase 3 SCORPIO-PEP trial (NCT05897541), 2,387 participants aged 12 and older, global randomized double-blind placebo-controlled, published in the New England Journal of Medicine on May 14, 2026. Primary endpoint: 67% reduction in risk of symptomatic COVID-19 through day 10 (2.9% ensitrelvir vs. 9.0% placebo; risk ratio 0.33; 95% CI 0.22 to 0.49; p less than 0.0001). High-risk subgroup: 76% relative risk reduction (2.4% vs. 9.9%; RR 0.24). Safety: adverse event rates nearly identical between groups (15.1% vs. 15.5%); no treatment-related dysgeusia (altered taste), which affected many patients on nirmatrelvir-ritonavir (Paxlovid). Dosing: 375 mg (3 tablets) on day 1, then 125 mg (1 tablet) daily on days 2 to 5, initiated within 72 hours of symptom onset in the exposed household contact. Not approved for treatment of active COVID-19 in the U.S. Important context: the prior PEP trials of nirmatrelvir-ritonavir and molnupiravir did not meet their primary endpoints; SCORPIO-PEP is the first and only Phase 3 oral antiviral PEP trial to do so. |
|---|
COVID-19 has been a fact of life since 2020. More than five years later, it remains endemic: the CDC estimated between 3.8 million and 12.4 million new COVID-19 cases in the United States between October 2025 and May 2026, resulting in as many as 240,000 hospitalizations and 42,000 deaths. The vaccines changed the acute mortality picture. The antivirals, primarily nirmatrelvir-ritonavir (Paxlovid), changed the treatment picture for high-risk individuals once infected. What has never existed is a tool for the gap between those two interventions: an oral option that someone can take after being exposed to a household member with COVID-19, before they become infected themselves.
On May 29, 2026, that gap closed. The FDA approved ensitrelvir (Xocova) as the first oral option to help prevent COVID-19 after exposure, for adults and adolescents aged 12 years and older following contact with an individual with COVID-19. The pivotal SCORPIO-PEP trial, the only Phase 3 study of an oral antiviral to meet the primary endpoint of preventing symptomatic COVID-19 following exposure, was published in the New England Journal of Medicine two weeks before the approval.
What Post-Exposure Prophylaxis Means and Why It Is a Different Goal Than Treatment
To understand what Xocova does and does not do, it is worth being precise about the concept of post-exposure prophylaxis (PEP).
Post-exposure prophylaxis is the use of a drug or intervention after confirmed or probable exposure to a pathogen, with the goal of preventing infection or disease before symptoms develop. The classic example is HIV PEP: a combination of antiretroviral drugs taken for 28 days after a potential HIV exposure, which significantly reduces the risk of infection if started promptly. The same principle applies to rabies post-exposure vaccination and to some bacterial infections.
COVID-19 PEP is conceptually identical but pharmacologically distinct: in this case, the goal is to prevent SARS-CoV-2 from establishing productive infection in the body of someone who has just been exposed to an infected person, by suppressing viral replication in the earliest window before the viral load grows to symptomatic levels.
What this means for understanding Xocova:
Xocova is not a treatment for active COVID-19 infection in the United States. It is not taken once you have symptoms. It is taken when you have been exposed and do not yet have symptoms. The timing window is critical: it must be initiated within 72 hours of symptom onset in the index case (the household member with COVID-19), which in practice means within days of knowing that someone in your home is infected.
What Ensitrelvir Is: The 3CL Protease Mechanism
Ensitrelvir is a SARS-CoV-2 main protease (3CL protease, or Mpro) inhibitor. This is the same general class of target as nirmatrelvir (the active component of Paxlovid), but ensitrelvir is a chemically distinct molecule developed independently by Shionogi through a research collaboration with Hokkaido University.
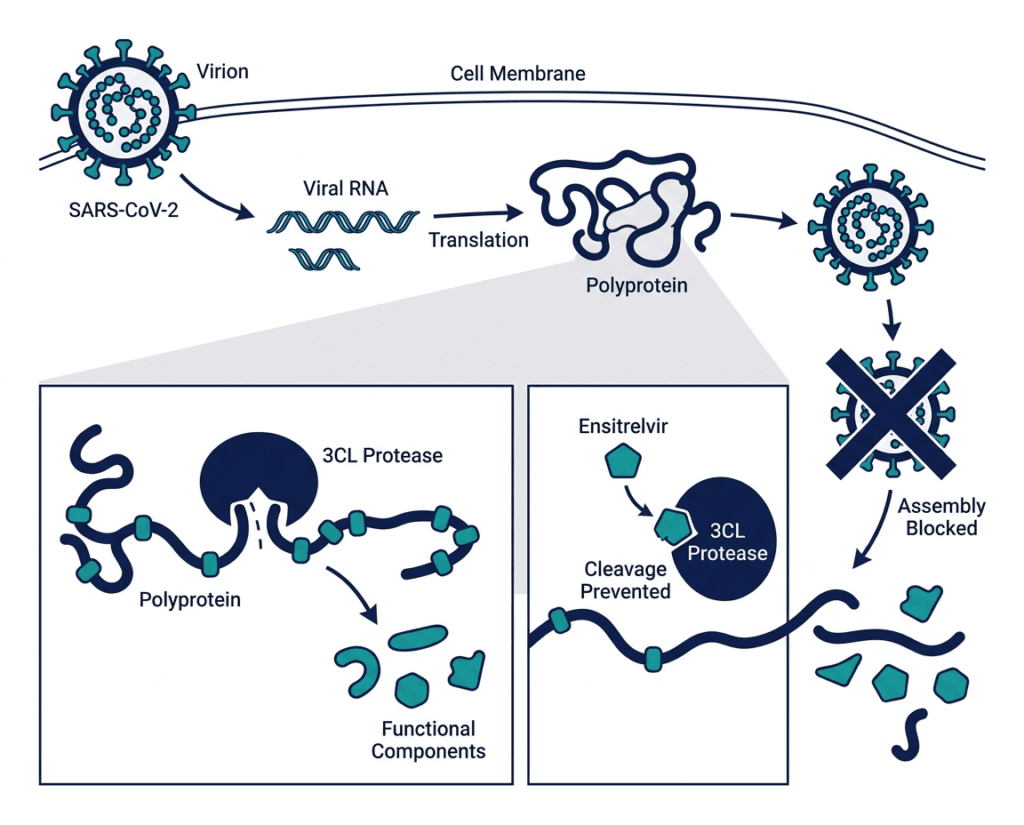
The SARS-CoV-2 3CL protease is an enzyme that is essential for viral replication. After the virus enters a cell and its RNA is translated into a large polyprotein, the 3CL protease cleaves this polyprotein into the functional viral components needed to assemble new virus particles. Without this cleavage, functional viral replication cannot proceed. By blocking the 3CL protease, ensitrelvir prevents the virus from producing the components it needs to replicate, suppressing the viral load in exposed individuals before it can rise to the level that produces symptoms and transmission.
| How ensitrelvir differs from nirmatrelvir (the active component of Paxlovid) Both ensitrelvir and nirmatrelvir target the 3CL protease, but they are structurally different molecules with different pharmacological profiles. Nirmatrelvir requires co-administration with ritonavir as a pharmacokinetic booster because it is rapidly metabolized by CYP3A4 in the liver; ritonavir inhibits CYP3A4, extending nirmatrelvir’s half-life. This ritonavir requirement creates the significant drug-drug interaction problem that limits Paxlovid use in many patients on common medications. Ensitrelvir does not require a pharmacokinetic booster. It has adequate oral bioavailability and a sufficiently long half-life on its own. This means Xocova does not carry the same extensive drug interaction liability that makes Paxlovid unusable in patients on many common medications (statins, blood thinners, immunosuppressants, anticonvulsants). Ensitrelvir is still a CYP3A4 substrate and inhibitor and has its own drug interaction considerations (discussed in the safety section), but the interaction profile is less extensive than ritonavir-boosted nirmatrelvir. |
|---|
The SCORPIO-PEP Trial: Full Results
Why this trial matters beyond just this approval
The findings differ from prior postexposure prophylaxis trials of nirmatrelvir-ritonavir and molnupiravir, which did not show statistically significant protection against COVID-19 in household contacts. Understanding why those trials failed contextualizes why SCORPIO-PEP succeeded.
The nirmatrelvir-ritonavir PEP trial (EPIC-PEP) did not meet its primary endpoint. The molnupiravir PEP trial similarly did not demonstrate statistically significant protection. These failures were attributed in part to late initiation windows (up to 5 days post-exposure rather than 72 hours post-symptom onset), less strict illness definitions, and different patient populations. The SCORPIO-PEP researchers suggested that earlier treatment initiation, within 72 hours following symptom onset in the index patient, along with a stricter illness definition, may have contributed to the observed efficacy.
Design
SCORPIO-PEP (NCT05897541) was a global, randomized, double-blind, placebo-controlled Phase 3 trial enrolling participants at sites in the United States, Europe, Asia, and Latin America. The trial enrolled 2,387 participants aged 12 years and older who tested negative for SARS-CoV-2 and had no symptoms at enrollment despite exposure to a household member with symptomatic COVID-19.
Key eligibility requirements:
- Age 12 years or older
- Negative SARS-CoV-2 test at baseline (RT-PCR confirmed at central laboratory)
- No COVID-19 symptoms at enrollment
- Household exposure to a member with symptomatic COVID-19
- Treatment initiated within 72 hours of symptom onset in the index household case
Primary endpoint definition: Laboratory-confirmed (central PCR) SARS-CoV-2 infection plus at least one of 14 prespecified COVID-19 symptoms lasting at least 48 hours, through day 10.
Randomization: 1:1 to ensitrelvir or placebo. Participants were randomly assigned to receive ensitrelvir (375 mg on day 1 and 125 mg on days 2 to 5) or placebo, once daily, and began treatment within 72 hours of when the household member with COVID-19 began showing symptoms.
Primary analysis population: 2,041 participants with laboratory-confirmed negative baseline tests (excluding 346 who tested positive at baseline and were therefore already infected at enrollment).
Primary endpoint results
| Outcome through Day 10 | Ensitrelvir (n=1,030) | Placebo (n=1,011) | Comparison |
|---|---|---|---|
| Symptomatic COVID-19 | 2.9% (30 patients) | 9.0% (91 patients) | — |
| Risk ratio | 0.33 | Reference | 95% CI 0.22 to 0.49 |
| Relative risk reduction | 67% | — | p less than 0.0001 |
Source: Hayden FG, Ohmagari N, et al. Ensitrelvir COVID-19 Post-exposure Prophylaxis in Household Contacts. New England Journal of Medicine. Published May 14, 2026. doi:10.1056/NEJMoa2506186. SCORPIO-PEP NCT05897541.
A 67% relative risk reduction means participants in the ensitrelvir arm were approximately three times less likely to develop symptomatic COVID-19 after household exposure. The absolute risk reduction is 6.1 percentage points (9.0% minus 2.9%), implying that approximately 16 to 17 people would need to receive Xocova to prevent one case of symptomatic COVID-19 from a household exposure.
High-risk subgroup: the most clinically relevant finding
The prespecified high-risk subgroup showed a 76% relative risk reduction (2.4% vs. 9.9%; RR 0.24), strengthening the rationale for post-exposure prevention beyond vaccination alone. This subgroup included participants with risk factors for severe COVID-19, the population for whom preventing infection carries the most meaningful clinical consequence. Among participants with risk factors for severe illness, COVID-19 developed in 9 of 382 participants assigned to ensitrelvir and 37 of 374 assigned to placebo.
The higher relative risk reduction in the high-risk subgroup (76% versus 67% overall) suggests that the drug’s preventive benefit is at least as strong in the people who need it most. This is the group that matters most clinically: older adults, immunocompromised individuals, people with cardiovascular disease or diabetes, and others for whom even a mild COVID-19 infection can trigger worsening of underlying conditions or long COVID.
Secondary and exploratory findings
In post-hoc analyses, viral loads and symptom scores appeared lower among ensitrelvir recipients who had infection at baseline or developed infection during the study, suggesting antiviral activity even in those who became infected. This is consistent with the drug’s mechanism, as protease inhibition reduces viral replication regardless of the infection stage.
Safety
Xocova was generally well tolerated, with similar rates of adverse events across groups (15.1% in the Xocova group and 15.5% in the placebo group). The most common adverse events (regardless of causality) occurring in greater than or equal to 1% of the Xocova group and at a greater frequency compared to placebo were headache, diarrhea, and cough. There were no reports of altered taste (dysgeusia) attributed to Xocova in the trial.
The absence of dysgeusia is clinically notable. Altered taste is one of the most commonly reported adverse effects of nirmatrelvir-ritonavir (Paxlovid), affecting a significant proportion of patients and sometimes leading to premature discontinuation. The clean tolerability profile of Xocova in the PEP trial, with adverse events statistically indistinguishable from placebo, supports its suitability for use in asymptomatic or presymptomatic individuals who may have no particular reason to tolerate medication side effects.
Who Xocova Is and Is Not For
The approved population
Xocova is approved for adults and adolescents aged 12 years and older who have been exposed to a person in their household with COVID-19. There is no age cutoff at the upper end, meaning the approval covers older adults, who are among those most likely to benefit from prevention.
The label says “household contact” specifically. The SCORPIO-PEP trial enrolled household contacts, meaning people living in the same home as an infected person. This reflects the highest-risk exposure scenario (prolonged close contact, shared indoor air space), and this is where the evidence was generated.
Critical timing requirement
Xocova must be initiated within 72 hours of the symptom onset of the infected household contact. This is not a treatment taken when you start feeling sick; it is a prevention taken when you learn that someone in your home is sick. The logistics of this matter practically: you will need to have a prescription in advance or be able to obtain one quickly, because the 72-hour window can close rapidly.
Who should discuss Xocova with their prescriber first
Several groups have specific considerations before using Xocova:
Drug interactions: Ensitrelvir is a CYP3A4 substrate and inhibitor. While it does not require ritonavir boosting, it can affect the levels of other CYP3A4-metabolized medications and can have its own levels affected by strong CYP3A4 inducers or inhibitors. Review the full prescribing information or consult a pharmacist before initiating in patients on chronic medications.
Immunocompromised patients: While this group is among those most likely to benefit, they may also have complex drug regimens that require interaction screening before initiating Xocova.
Pregnancy and breastfeeding: Safety data in pregnancy is limited. The decision to use Xocova during pregnancy should involve a discussion with a clinician familiar with the patient’s overall situation.
Patients who have already been vaccinated and boosted: The trial enrolled participants with diverse vaccination backgrounds. Whether current vaccination status meaningfully modifies the incremental benefit of Xocova PEP is not yet established by the trial data. For high-risk patients, particularly those who are immunocompromised and may have blunted vaccine responses, Xocova may provide meaningful additional protection on top of vaccination.
Who Xocova is not for in the U.S.
Xocova is not approved in the United States for the treatment of active COVID-19 infection. If you have COVID-19 symptoms, Xocova is not the appropriate option; nirmatrelvir-ritonavir (Paxlovid) or remdesivir (Veklury) are the relevant approved treatments for symptomatic disease. Xocova is specifically for prevention in people who have been exposed but are not yet symptomatic.
Dosing
| Day | Dose | Number of tablets |
|---|---|---|
| Day 1 (loading dose) | 375 mg | 3 tablets (125 mg each) |
| Days 2 to 5 | 125 mg once daily | 1 tablet per day |
| Total treatment duration | 5 days | — |
| Timing requirement | Begin within 72 hours of symptom onset in the exposed household contact | — |
| Administration | Oral, with or without food | — |
The Regulatory Context: Japan, Global Status, and the Path to the U.S.
Ensitrelvir’s regulatory history is global and worth understanding:
Xocova received emergency regulatory approval in Japan in November 2022 and full approval in March 2024 for the treatment of COVID-19 based on results from SCORPIO-SR, a Phase 3 study conducted in Asia during the Omicron-dominant phase of the pandemic. Ensitrelvir is also approved in Japan and Singapore for post-exposure prophylaxis.
The approval occurred ahead of the Prescription Drug User Fee Act (PDUFA) action date of June 16, 2026, meaning the FDA completed its review approximately 2.5 weeks before the scheduled deadline. The U.S. approval is specifically and only for post-exposure prophylaxis; treatment of active infection is not approved in the United States. Wockhardt has submitted a Marketing Authorization Application to the European Medicines Agency; regulatory reviews are also ongoing in other jurisdictions.
This is a meaningful distinction: ensitrelvir has been approved and used in Asia for treatment and prevention; the FDA’s U.S. approval is limited to the PEP indication where the Phase 3 evidence base is strongest and the clinical need is most clearly defined.
What This Means for COVID-19 Prevention Going Forward
The approval of Xocova represents a genuine expansion of the COVID-19 prevention toolkit. The current landscape before this approval offered vaccines for prophylaxis and antivirals for treatment, but no pharmacological bridge for the household exposure scenario, which is one of the highest-risk settings for transmission.
The SCORPIO-PEP data suggests several populations that may benefit most:
Older adults in congregate settings: COVID-19 disproportionately affects older adults with greater risk for severe illness and death in close-community settings, such as long-term care facilities. When a COVID-19 case is identified in a long-term care facility, Xocova PEP for exposed residents aged 12 and older is now a pharmacologically supported prevention strategy.
Immunocompromised individuals: Those with impaired vaccine responses, including transplant recipients, patients on immunosuppressive therapy, and patients with hematologic malignancies, have limited protection from vaccination alone. PEP with Xocova provides an additional layer of prevention after household exposure.
Caregivers of high-risk individuals: A caregiver who lives with and provides daily assistance to an older adult with multiple comorbidities has both personal and protective reasons to prevent becoming a COVID-19 vector. If a household member develops COVID-19, PEP for the caregiver reduces the risk of transmission to the high-risk person they serve.
Long COVID prevention: People diagnosed with COVID-19 had increased rates of both new and worsening neurologic, cardiovascular, respiratory, and renal conditions during the year following infection. Preventing acute infection prevents the downstream risk of these post-COVID complications for individuals who successfully avoid infection with Xocova.
For related HED coverage of COVID-19 treatment and prevention developments, see our coverage of nirmatrelvir-ritonavir (Paxlovid) and its drug interaction challenges and our post on Foundayo (orforglipron) and the post-marketing safety requirements for newer antivirals and metabolic drugs for context on how the FDA approaches post-marketing surveillance for novel mechanisms in new populations.
Sources
FDA approval / Shionogi press release: Shionogi Announces FDA Approval of XOCOVA (ensitrelvir), the First and Only Oral Option to Help Prevent COVID-19 Following Exposure. businesswire.com. May 31, 2026.
Drugs.com approval news: FDA Approves Xocova (ensitrelvir), the First and Only Oral Option to Help Prevent COVID-19 Following Exposure. drugs.com. June 1, 2026.
SCORPIO-PEP primary NEJM publication: Hayden FG, Ohmagari N, et al. Ensitrelvir COVID-19 Post-exposure Prophylaxis in Household Contacts. New England Journal of Medicine. Published May 14, 2026. doi:10.1056/NEJMoa2506186.
SCORPIO-PEP trial registration: NCT05897541. ClinicalTrials.gov.
Shionogi NEJM publication announcement: New England Journal of Medicine Publishes Shionogi Study Demonstrating Ensitrelvir Prevents COVID-19 Following Exposure. shionogi.com. May 14, 2026.
Contagion Live approval coverage: FDA Approves Ensitrelvir as First Oral Post-Exposure Prevention Option for COVID-19. contagionlive.com. May 2026.
Patient Care Online: FDA Approves Xocova as First Oral COVID-19 Postexposure Prophylaxis Option. patientcareonline.com. June 2026.
PharmExec coverage: FDA Approves Xocova as First Oral Post-Exposure Covid-19 Prevention Therapy. pharmexec.com. June 2026.
Pharmacy Times SCORPIO-PEP results: Ensitrelvir Demonstrates Significant COVID-19 Post-Exposure Prophylaxis Efficacy in Phase 3 Trial. pharmacytimes.com. 2026.
Conexiant clinical summary: Ensitrelvir Reduced COVID After Household Exposure. conexiant.com. June 2026.
Cardiology Advisor pre-approval coverage: Ensitrelvir Under Review for COVID-19 Postexposure Prophylaxis. thecardiologyadvisor.com. September 2025.
Xocova prescribing information: XOCOVA (ensitrelvir) Prescribing Information. Shionogi. 2026.
Paxlovid FDA approval: FDA approves nirmatrelvir-ritonavir (Paxlovid) for treatment of COVID-19. FDA.gov.
Ensitrelvir mechanism: Ensitrelvir as a SARS-CoV-2 Protease Inhibitor. PMC9941555.
3CL protease and SARS-CoV-2 replication: SARS-CoV-2 Main Protease Structure. PMC9941555.
Post-exposure prophylaxis concept: Post-Exposure Prophylaxis. StatPearls. NCBI.
HIV PEP reference: HIV Post-Exposure Prophylaxis. CDC.
CYP3A4 drug interactions: CYP3A4. StatPearls. NCBI.
Patient resources: CDC COVID-19 information | Xocova patient information | CDC COVID-19 treatments and prevention
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Xocova is a prescription medication approved only for post-exposure prophylaxis (PEP) of COVID-19 and is not approved for the treatment of active COVID-19 infection in the United States. Patients with COVID-19 symptoms should contact their healthcare provider. The 72-hour initiation window after symptom onset in the exposed household contact is a firm requirement. |
|---|
Leave a Reply