
| 📌 The essentials On April 30, 2026, the FDA approved Auvelity (dextromethorphan HBr and bupropion HCl, Axsome Therapeutics) for the treatment of agitation associated with dementia due to Alzheimer’s disease in adults. This is the first FDA-approved treatment for Alzheimer’s disease agitation that is not an antipsychotic, and only the second FDA-approved drug for this indication overall. Auvelity’s first approved indication was major depressive disorder in adults (August 2022). The mechanism: dextromethorphan is an uncompetitive NMDA receptor antagonist and sigma-1 receptor agonist; bupropion serves as a CYP2D6 inhibitor that slows dextromethorphan metabolism, substantially increasing dextromethorphan blood levels. Auvelity is a first-in-class treatment combining NMDA antagonism and sigma-1 modulation for agitation in Alzheimer’s disease. Regulatory designation: Breakthrough Therapy Designation (2020). The clinical basis: Phase 3 ADVANCE-1 trial (NCT03226522, 5-week parallel-group RCT, n=308) and Phase 3 ACCORD-2 randomized withdrawal trial (NCT04947553, 26-week randomized withdrawal among responders). ADVANCE-1 primary endpoint: statistically significant reduction in Cohen-Mansfield Agitation Inventory (CMAI) total score at week 5 versus placebo. ACCORD-2 primary endpoint: significantly longer time to relapse (HR 0.276; p=0.001) and lower relapse incidence (8.4% vs. 28.6%) in those continuing Auvelity versus switched to placebo. Important nuance: ADVANCE-2, a second 5-week parallel-group trial (n=408), missed its CMAI primary endpoint, though secondary measures showed numerical improvements. Boxed warning: increased risk of suicidal thoughts and behaviors (antidepressant class warning). Serious risks in elderly patients: seizures, elevated blood pressure, mania. Dosing: one tablet (45 mg dextromethorphan / 105 mg bupropion) twice daily. |
|---|
Agitation in Alzheimer’s disease is one of the most distressing and difficult-to-manage aspects of the condition, for patients and for caregivers alike. It is not simply behavioral inconvenience. It encompasses excessive motor activity, verbal aggression, physical aggression, emotional distress, disinhibition, and disruptive irritability. It occurs in an estimated 40 to 76% of people with Alzheimer’s disease over the course of their illness. It is among the leading drivers of nursing home placement. It contributes to caregiver burnout. And until April 30, 2026, the only FDA-approved drug for it was brexpiprazole (Rexulti), an atypical antipsychotic that carries a boxed warning for increased mortality in elderly patients with dementia-related psychosis.
That warning, applied class-wide to all antipsychotics in this population, has made prescribers appropriately cautious. Antipsychotics are associated with increased risk of death in elderly dementia patients, an association serious enough to generate the FDA’s black box in 2005 for typical antipsychotics and 2008 for atypical antipsychotics. They have nonetheless been widely used off-label for Alzheimer’s agitation because the need was so severe and the alternatives so limited.
On April 30, 2026, the FDA approved the first non-antipsychotic option. Auvelity (dextromethorphan-bupropion) targets NMDA receptors and sigma-1 receptors through a mechanism entirely distinct from dopamine receptor blockade, providing a pharmacological approach that does not carry the mortality warning applied to antipsychotics in this population.
The clinical data behind the approval requires honest presentation: it is more nuanced than the headline suggests, and families and clinicians deserve a complete picture.
What Alzheimer’s Disease Agitation Is and Why It Is So Hard to Treat
Defining agitation in the context of dementia
Agitation in Alzheimer’s disease is formally defined as behavior that includes at least one of three domains: excessive motor activity (pacing, handwringing, rocking); verbal aggression (screaming, cursing, threatening); or physical aggression (hitting, biting, scratching). To meet a clinical threshold for treatment, these behaviors must be associated with distress in the patient, represent a change from premorbid behavior, and not be solely attributable to another medical cause or psychosis.
The Cohen-Mansfield Agitation Inventory (CMAI), the instrument used as the primary efficacy measure in ADVANCE-1, is a validated 29-item scale assessing the frequency of specific agitated behaviors on a scale from 1 (never) to 7 (several times per hour). Higher scores indicate more frequent agitation. The CMAI is the most widely used and well-validated agitation measure in Alzheimer’s disease research and has been accepted by the FDA as a primary endpoint in this indication.
The pathophysiology behind agitation in Alzheimer’s disease
Agitation in Alzheimer’s disease is not simply a behavioral response to cognitive decline. It reflects specific neurobiological changes in the Alzheimer’s brain: degeneration of the prefrontal cortex and its connections impairs impulse control and emotional regulation; locus coeruleus neurodegeneration disrupts norepinephrine signaling affecting arousal and stress responses; and aberrant glutamate signaling through NMDA receptors contributes to the excitotoxic and dysregulated neuronal activity associated with agitation and other behavioral symptoms.
This neurobiological basis for agitation is what makes the NMDA antagonist mechanism of dextromethorphan a rational pharmacological target, distinct from the dopamine-based mechanism of antipsychotics.
| Why off-label antipsychotics have remained standard despite the mortality risk The FDA issued boxed warnings for both typical and atypical antipsychotics in dementia patients between 2005 and 2008, following multiple trials and pharmacovigilance analyses showing a 1.6 to 1.7-fold increased risk of death versus placebo in elderly patients with dementia-related psychosis and behavioral disturbances. Despite this warning, antipsychotics (particularly quetiapine, risperidone, and haloperidol) have continued to be widely prescribed for Alzheimer’s agitation off-label, because the severity of unmanaged agitation creates a real and urgent clinical need that outweighs the mortality risk for many patients in institutional settings. The lack of an approved non-antipsychotic alternative for more than 15 years is the direct reason for this uncomfortable clinical reality. The approval of brexpiprazole in 2023 addressed the first part of the gap: an FDA-approved indication for Alzheimer agitation. But it is still an antipsychotic carrying the same mortality warning. Auvelity addresses the second part: a genuinely mechanistically distinct option without that class-level mortality warning. |
|---|
How Auvelity Works in Alzheimer’s Disease Agitation
Auvelity’s pharmacology in Alzheimer’s disease agitation reflects the same mechanism that supported its 2022 approval for major depressive disorder, applied to a different behavioral target.
Dextromethorphan: the pharmacologically active agent
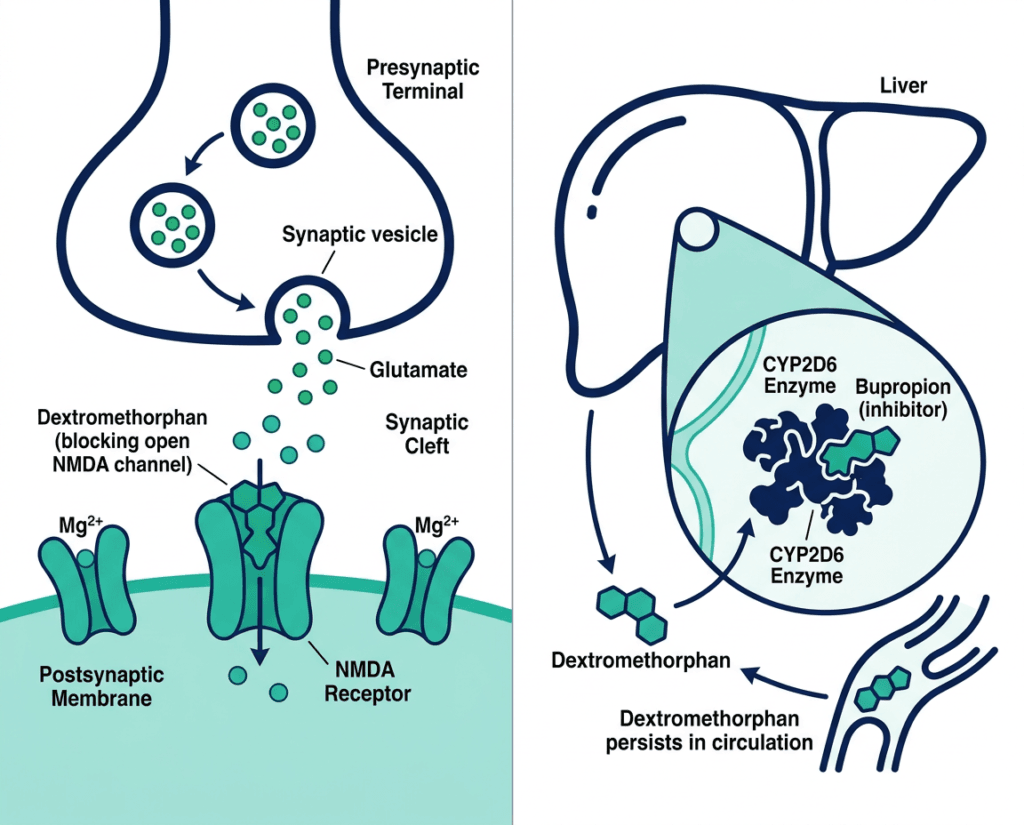
Dextromethorphan (DXM) is a synthetic morphinan compound familiar as the cough-suppressing active ingredient in many over-the-counter cold preparations. At the doses used in Auvelity, which are substantially higher than OTC cough suppressant doses, it acts as an uncompetitive NMDA receptor antagonist and a sigma-1 receptor agonist.
NMDA receptor antagonism: NMDA receptors are glutamate receptors involved in synaptic plasticity, learning, and memory but also in excitotoxic signaling when overactivated. In Alzheimer’s disease, aberrant NMDA receptor activity is implicated in both neurodegeneration and behavioral dysregulation. Blocking these receptors, as memantine (Namenda) does (memantine is an FDA-approved NMDA antagonist for moderate to severe Alzheimer’s cognitive symptoms), may reduce the neurochemical substrate for agitation. DXM’s NMDA antagonism is uncompetitive, meaning it binds the receptor channel in its open state, providing a rapid blocking effect that differs pharmacodynamically from memantine’s competitive inhibition.
Sigma-1 receptor agonism: The sigma-1 receptor is a chaperone protein in the endoplasmic reticulum of neurons involved in neuroplasticity, neuroprotection, and neurotransmitter regulation. Sigma-1 agonism may have independent anxiolytic and neuroprotective effects relevant to Alzheimer’s disease behavioral symptoms.
Bupropion: the pharmacokinetic enabler
Bupropion is an aminoketone antidepressant that inhibits CYP2D6, the hepatic enzyme responsible for metabolizing dextromethorphan. When taken alone, DXM is rapidly metabolized by CYP2D6 and does not achieve sustained therapeutic blood levels for neuropsychiatric indications. Bupropion’s CYP2D6 inhibition blocks this metabolism, dramatically increasing DXM blood levels and duration of action, achieving therapeutic NMDA and sigma-1 receptor engagement that OTC doses of DXM cannot.
This pharmacokinetic partnership is the core mechanism behind Auvelity’s design: bupropion is not chosen for its antidepressant properties in this combination (the bupropion-alone arm in ADVANCE-1 was terminated for futility, confirming bupropion alone has no meaningful effect on Alzheimer’s agitation) but because it makes DXM pharmacologically effective at lower doses with better tolerability.
The Clinical Evidence: Two Trials, a Complete Picture
The FDA’s approval is based on two Phase 3 trials: ADVANCE-1 (positive) and ACCORD-2 (positive). A third trial, ADVANCE-2, also informed the totality of evidence but missed its primary endpoint and deserves honest presentation.
ADVANCE-1 (NCT03226522): the 5-week parallel-group primary efficacy trial
ADVANCE-1 was a randomized, double-blind, 5-week, parallel-group, placebo-controlled Phase 3 trial in adults with Alzheimer’s disease and moderate to severe agitation. The trial enrolled 308 patients across three arms: Auvelity (n=152), placebo (n=156), and bupropion alone (n, terminated early for futility).
Primary endpoint: Change in CMAI total score from baseline at week 5.
Auvelity versus placebo (CMAI change): Auvelity was statistically significantly superior to placebo in reducing CMAI total score at week 5. The improvement was consistent with clinically meaningful agitation reduction.
Key secondary endpoint: A statistically significantly greater proportion of Auvelity-treated patients were rated by clinicians as “minimally improved” or better on the modified Alzheimer’s Disease Cooperative Study Clinical Global Impression of Change (mADCS-CGIC) at week 5.
Bupropion-alone arm: Terminated for futility at a planned interim analysis, confirming that bupropion alone has no clinically meaningful effect on Alzheimer’s agitation. This is an important finding: it confirms that the efficacy of Auvelity is attributable to the pharmacological effect of enhanced DXM rather than to bupropion’s antidepressant or dopaminergic properties.
ACCORD-2 (NCT04947553): the 26-week randomized withdrawal durability trial
ACCORD-2 used a different trial design: an open-label lead-in phase in which all patients received Auvelity, followed by randomization (only among responders who achieved sustained response) to continue Auvelity or switch to placebo for up to 26 weeks. This enriched randomized withdrawal design is appropriate for evaluating whether response is maintained over longer treatment periods.
Open-label lead-in findings: Patients showed rapid CMAI improvement during the lead-in phase, with a mean reduction of 20.4 points at week 6 (46% reduction from baseline). Approximately 69% achieved at least a 30% response, qualifying them for the randomized withdrawal phase.
Randomized withdrawal phase primary endpoint: Time to relapse of agitation symptoms.
| Outcome | Continue Auvelity | Switch to placebo |
|---|---|---|
| Hazard ratio for relapse | 0.276 | Reference |
| p-value | 0.001 | — |
| Relapse incidence | 8.4% | 28.6% |
Patients continuing Auvelity experienced significantly longer time to relapse and substantially lower relapse incidence than those switched to placebo. The approximately 72% reduction in relative relapse risk over 26 weeks confirms durable maintenance of the anti-agitation response.
The important design caveat: Because ACCORD-2 enrolled only patients who had responded to Auvelity before randomization, its relapse findings should be interpreted in the context of an enriched responder population. It confirms that Auvelity works in those who respond; it cannot speak to what proportion of all Alzheimer’s agitation patients will respond.
ADVANCE-2: the missed primary endpoint, presented honestly
ADVANCE-2 was a second 5-week parallel-group trial in 408 participants with Alzheimer’s agitation. Unlike ADVANCE-1, it missed its primary endpoint: the between-group difference in CMAI change at week 5 was −13.8 in the Auvelity arm versus −12.6 in the placebo arm, not reaching statistical significance. Secondary measures showed numerical improvements but these were not formally significant given the failed primary endpoint.
The FDA’s approval despite ADVANCE-2’s failure reflects the totality of evidence approach: ADVANCE-1 met its primary endpoint, ACCORD-2 met its primary endpoint with a compelling relapse reduction effect, the bupropion-futility finding provides mechanistic clarity, and the long-term safety data is favorable. The difference between ADVANCE-1 and ADVANCE-2 results in the same endpoint is not fully explained and represents genuine clinical uncertainty about the magnitude of benefit in all patients.
This is important information for families and clinicians: Auvelity works meaningfully for many patients, but the clinical evidence includes one failed parallel-group trial, and not every patient should be expected to respond.
Auvelity’s Second Indication: How This Differs From the MDD Approval
Auvelity was first approved in August 2022 for major depressive disorder in adults, based on the GEMINI and ASCEND trials demonstrating rapid antidepressant effects. The Alzheimer’s agitation indication uses the same drug at the same dose but for a neurobiologically and clinically distinct target.
This creates some complexity for prescribers:
- The boxed warning for suicidal thoughts in adolescents and young adults is a class effect from the antidepressant pharmacology of bupropion; while the approved Alzheimer’s agitation indication covers elderly adults (who are at lower background risk of this complication), the warning is still on the label
- In Alzheimer’s disease patients specifically, separating depression from agitation is clinically important: depression is very common in Alzheimer’s disease, and Auvelity’s dual indication means it may be considered for patients who have both conditions, though the trials studied these separately
- Drug interactions relevant to bupropion’s CYP2D6 inhibition are the same across indications
Auvelity’s Place in Alzheimer’s Disease Agitation Treatment
With this approval, two drugs now have FDA approval for Alzheimer’s disease agitation:
| Drug | Company | Mechanism | Approval date | Boxed warning |
|---|---|---|---|---|
| Brexpiprazole (Rexulti) | Otsuka/Lundbeck | Atypical antipsychotic (partial D2 agonist) | May 2023 | Increased mortality in elderly patients with dementia-related psychosis |
| Auvelity (dextromethorphan-bupropion) | Axsome Therapeutics | NMDA antagonist/sigma-1 agonist | April 30, 2026 | Suicidal thoughts (antidepressant class); no dementia mortality warning |
The absence of a dementia-specific mortality warning on Auvelity does not mean it is risk-free in this population. It means its mechanism (NMDA antagonism rather than dopamine receptor blockade) does not carry the class-level mortality association established for antipsychotics. Individual patient risk-benefit assessment by a qualified clinician familiar with the patient’s full medical picture remains essential.
For patients who are not appropriate candidates for antipsychotic therapy, including those with Parkinson’s disease or Lewy body dementia where antipsychotics carry heightened risk, Auvelity may be a particularly relevant option.
Safety: What the Prescribing Information Covers
Boxed warning
Increased risk of suicidal thoughts and behaviors: All antidepressants, including bupropion (a component of Auvelity), carry a class-level boxed warning for increased risk of suicidal thoughts and behaviors in children, adolescents, and young adults. The Alzheimer’s agitation indication is in elderly adults, where this risk is substantially lower, but the warning is present on the label. Monitor for clinical worsening and emergence of suicidal thoughts in all patients.
Warnings specific to elderly Alzheimer’s patients
Seizure risk: Bupropion is associated with dose-dependent seizure risk. This risk is relevant in elderly Alzheimer’s patients who may have underlying cerebrovascular disease, which independently increases seizure risk. The seizure warning in the prescribing information is particularly relevant in patients with prior seizures, CNS tumors, or concurrent medications that lower the seizure threshold.
Elevated blood pressure and hypertension: Bupropion inhibits norepinephrine reuptake, which can elevate blood pressure. Monitor blood pressure before starting and periodically during treatment. In elderly patients with cardiovascular disease, this is a clinically important consideration.
Activation of mania or hypomania: Relevant primarily for patients with undiagnosed or undertreated bipolar disorder.
Common adverse events (occurring in at least 5% and more than twice placebo in ADVANCE-1)
Dizziness, nausea, headache, diarrhea, somnolence, dry mouth, hyperhidrosis.
Drug interactions
Because bupropion is a CYP2D6 inhibitor, Auvelity will increase the plasma concentration of other CYP2D6-metabolized drugs (including many antidepressants, antipsychotics, beta-blockers, and opioids). Review the full prescribing information for the complete interaction table. This is particularly relevant in elderly patients on multiple medications.
Dosing
One extended-release tablet (dextromethorphan 45 mg / bupropion 105 mg) taken twice daily, morning and evening. Do not crush, cut, or chew the extended-release tablet. The tablet can be taken with or without food.
For Patients, Families, and Caregivers
What Auvelity is and is not
Auvelity is a treatment for agitation in Alzheimer’s disease. It is not a cognitive enhancer, does not slow disease progression, and is not a substitute for existing Alzheimer’s disease treatments such as donepezil, memantine, or lecanemab. It specifically targets one of the most disabling behavioral symptoms of Alzheimer’s disease.
What to expect if starting treatment
If Auvelity is prescribed, the ACCORD-2 open-label data showed that meaningful agitation improvement became apparent within the first several weeks of treatment, with about 69% of patients achieving at least a 30% improvement by week 6. Not all patients will respond. If no meaningful improvement is seen after an adequate trial, this should prompt discussion with the prescribing clinician about alternative management strategies.
Caregiver considerations
Alzheimer’s disease agitation is one of the most significant drivers of caregiver distress and burnout. The availability of a non-antipsychotic FDA-approved option may facilitate earlier treatment consideration in patients where clinicians or families have been reluctant to start antipsychotic therapy.
The Alzheimer’s Association maintains current resources on managing behavioral symptoms in Alzheimer’s disease, including agitation, with clinical guidance for families navigating these decisions. The Family Caregiver Alliance provides practical support resources specifically for dementia caregivers. The National Institute on Aging maintains current information on all FDA-approved Alzheimer’s treatments.
For related HED coverage on Alzheimer’s disease treatment advances and FDA approvals, see our post on AVLAYAH, the first gene therapy crossing the blood-brain barrier to reach neurons in Hunter syndrome for context on how the BBB problem in neurological disease is being approached across conditions, and our post on Ocrevus expanding to pediatric multiple sclerosis as another example of 2026 approvals expanding the treatment toolkit for neurological conditions.
Sources
FDA press announcement: FDA Approves First Non-Antipsychotic Drug to Treat Agitation Associated with Dementia. FDA.gov. April 30, 2026.
Axsome Therapeutics press release: Axsome Therapeutics Announces FDA Approval of Auvelity (dextromethorphan HBr and bupropion HCl) for the Treatment of Agitation Associated with Dementia due to Alzheimer’s Disease. GlobeNewswire. April 30, 2026.
Drugs.com approval news: Axsome Therapeutics Announces FDA Approval of Auvelity for Agitation Associated with Dementia. drugs.com. April 30, 2026.
Psychiatric Times detailed clinical summary: FDA Approves Auvelity for Treatment of Agitation in Alzheimer Disease. psychiatrictimes.com. May 2026.
NeurologyLive detailed coverage: FDA Approves AXS-05 as New Treatment for Alzheimer Disease Agitation. neurologylive.com. May 2026.
Neurology Advisor: Auvelity Gains Approval for Agitation in Alzheimer Disease. neurologyadvisor.com. April 2026.
Conexiant clinical summary: FDA Approves Auvelity for Agitation in Alzheimer’s Disease. conexiant.com. April 2026.
AJMC: FDA Approves Dextromethorphan-Bupropion for Agitation Due to Alzheimer Disease. ajmc.com. May 2026.
Pharmacy Times: FDA Approves First Non-Antipsychotic Treatment for Agitation Associated with Alzheimer Disease. pharmacytimes.com. 2026.
Consultant360: FDA Approves Auvelity for Agitation in Alzheimer Disease Dementia. consultant360.com. May 2026.
ADVANCE-1 trial registration: NCT03226522. ClinicalTrials.gov.
ACCORD-2 trial registration: NCT04947553. ClinicalTrials.gov.
Brexpiprazole Alzheimer agitation FDA approval: FDA approves brexpiprazole for agitation associated with Alzheimer’s disease dementia. FDA.gov. May 2023.
Auvelity prescribing information: Auvelity (dextromethorphan HBr and bupropion HCl) Prescribing Information. Axsome Therapeutics. 2026.
Alzheimer’s disease agitation overview: Neuropsychiatric Symptoms in Alzheimer’s Disease. PMC8461428.
CMAI instrument: Cohen-Mansfield Agitation Inventory. PMC5880688.
NMDA receptor antagonism in AD: NMDA Receptor Antagonists in Alzheimer’s Disease. PMC5542145.
Sigma-1 receptor: Sigma-1 Receptor in Neurological Disorders. PMC6370317.
Dextromethorphan pharmacology: Dextromethorphan. StatPearls. NCBI.
Bupropion: Bupropion. StatPearls. NCBI.
CYP2D6: CYP2D6. StatPearls. NCBI.
Memantine FDA approval: FDA approves memantine for moderate to severe Alzheimer’s disease. FDA.gov.
Agitation StatPearls: Agitation and Delirium in Elderly. StatPearls. NCBI.
Patient resources: Alzheimer’s Association: Behavioral Symptoms | Family Caregiver Alliance | National Institute on Aging: Alzheimer’s Treatments
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Auvelity carries a boxed warning for suicidal thoughts and behaviors associated with antidepressant medications. Decisions about treatment for Alzheimer’s disease agitation, including whether Auvelity is appropriate for a specific patient, should be made in close consultation with a qualified neurologist, geriatric psychiatrist, or geriatrician familiar with the patient’s complete medical history, current medications, and clinical circumstances. |
|---|
Leave a Reply