| 📌 The essentials Januvia (sitagliptin, Merck) is an oral DPP-4 inhibitor approved in October 2006 for the treatment of type 2 diabetes as monotherapy and as add-on combination therapy. Nearly 8 million Januvia prescriptions were filled in the United States in 2022 alone. Combined franchise sales with Janumet and Janumet XR exceeded $2 billion annually as recently as 2023. Retail price without insurance: approximately $600 to $700 per month. Generic timeline: Merck’s core sitagliptin patent expires November 24, 2026. Settlement agreements with more than 21 generic manufacturers allow launches as early as May 2026 under certain conditions. A generic sitagliptin phosphate (Viatris/Watson Labs) was approved December 30, 2025. Additionally, Zituvio (sitagliptin free base, Zydus), a different chemical form of sitagliptin that is not substitutable for Januvia at the pharmacy counter but can be prescribed specifically, has been available at select specialty pharmacies for approximately $80 per month since its October 2023 FDA approval. Expected generic price once multiple manufacturers are in the market: 80 to 85% below brand list price, approximately $80 to $100 per month. Janumet generics expected by May 2026; Janumet XR generics by July 2026, per settlement terms. Cardiovascular safety: the TECOS trial (n=14,671) established cardiovascular non-inferiority to placebo (HR 0.98; 95% CI 0.89 to 1.08; p less than 0.001 for non-inferiority). Sitagliptin did not increase heart failure hospitalizations in TECOS, a finding that distinguishes it from saxagliptin within the DPP-4 class. Sitagliptin does not have cardiovascular or cardiorenal protective indications. |
|---|
| 📚 About this series: the 2026 Loss of Exclusivity Watch This is Post 4 of HED’s 2026 Loss of Exclusivity series, tracking the ten major drugs losing U.S. exclusivity this year. The full series covers: Xolair (omalizumab) • Pomalyst (pomalidomide) • Opsumit (macitentan) • Januvia/Janumet (sitagliptin) • Simponi (golimumab) • Mavenclad (cladribine) • Gattex (teduglutide) • Trintellix (vortioxetine) • Briviact (brivaracetam) • Xeljanz (tofacitinib). Each post follows the same format: what the drug is and how it works, what the clinical evidence shows, who uses it and why, and what the entrance of competition means for patients, prescribers, and the market. |
|---|
Type 2 diabetes is one of the most common chronic conditions in the United States. Roughly 38 million Americans have diabetes, and about 90 to 95% of those cases are type 2. Managing it requires lifelong medication for most patients, typically starting with metformin and expanding to one or more additional agents as the disease progresses. The medication decisions made at each step affect not just blood sugar numbers, but long-term risks of kidney disease, nerve damage, heart attack, stroke, and blindness.
Januvia (sitagliptin) has been a cornerstone of type 2 diabetes management since its FDA approval in October 2006. Its combination of proven efficacy, low hypoglycemia risk, weight neutrality, and once-daily oral dosing made it a clinically attractive option for many patients. Nearly 8 million Januvia prescriptions were filled in the United States in 2022 alone, and its combined franchise with Janumet and Janumet XR generated over $2 billion in annual global sales as recently as 2023.
Its major limitation has been cost. At $600 to $700 per month retail with no widely available true generic, affordability has been a significant barrier for the millions of patients who take it.
That is changing. Merck’s core sitagliptin patent expires November 24, 2026, and settlement agreements with more than 21 generic manufacturers may allow generic sitagliptin to enter the market as early as May 2026 under certain conditions. Generic sitagliptin is expected to cost 80 to 85% less than brand-name Januvia once multiple manufacturers are competing.
This post covers what sitagliptin is, how DPP-4 inhibition works at a molecular level, what the clinical evidence shows about its efficacy and cardiovascular safety (including a nuanced story about heart failure that is often misunderstood), where it fits in the 2026 diabetes treatment landscape, and what the arrival of generics means for patients who have been caught between a drug that works and a price that does not.
A Brief History: How Sitagliptin Changed Diabetes Medicine
When the FDA approved Januvia in October 2006, it introduced a genuinely new class of diabetes medication. DPP-4 inhibitors worked through a mechanism that none of the existing oral agents — metformin, sulfonylureas, thiazolidinediones — shared: they amplified the body’s own hormonal response to meals rather than directly stimulating insulin secretion or reducing insulin resistance.
The clinical profile that emerged from trials was distinctive. Sitagliptin lowered blood sugar meaningfully but without causing hypoglycemia on its own, because its mechanism is glucose-dependent. It was weight neutral, a meaningful advantage over insulin and many other agents. It was well tolerated. And it came in a single once-daily pill with no food restrictions.
Five DPP-4 inhibitors, including sitagliptin, vildagliptin, alogliptin, saxagliptin, and linagliptin, were approved by regulatory authorities and entered the market between 2006 and 2013. For a decade, DPP-4 inhibitors became one of the most commonly prescribed second-line diabetes medication classes in the world. Januvia, as the first and best-known entry, captured the largest share of that market.
Merck generated roughly $50 billion in cumulative global Januvia sales over nearly two decades. The company has told investors it expects sales to drop substantially following generic launches, with research suggesting a drug’s price can fall as much as 20% when the first generic enters and as much as 85% after multiple alternatives are established.
The Science: How DPP-4 Inhibition Works
Understanding what sitagliptin does requires a brief explanation of the incretin system, one of the body’s core mechanisms for managing blood sugar after meals.
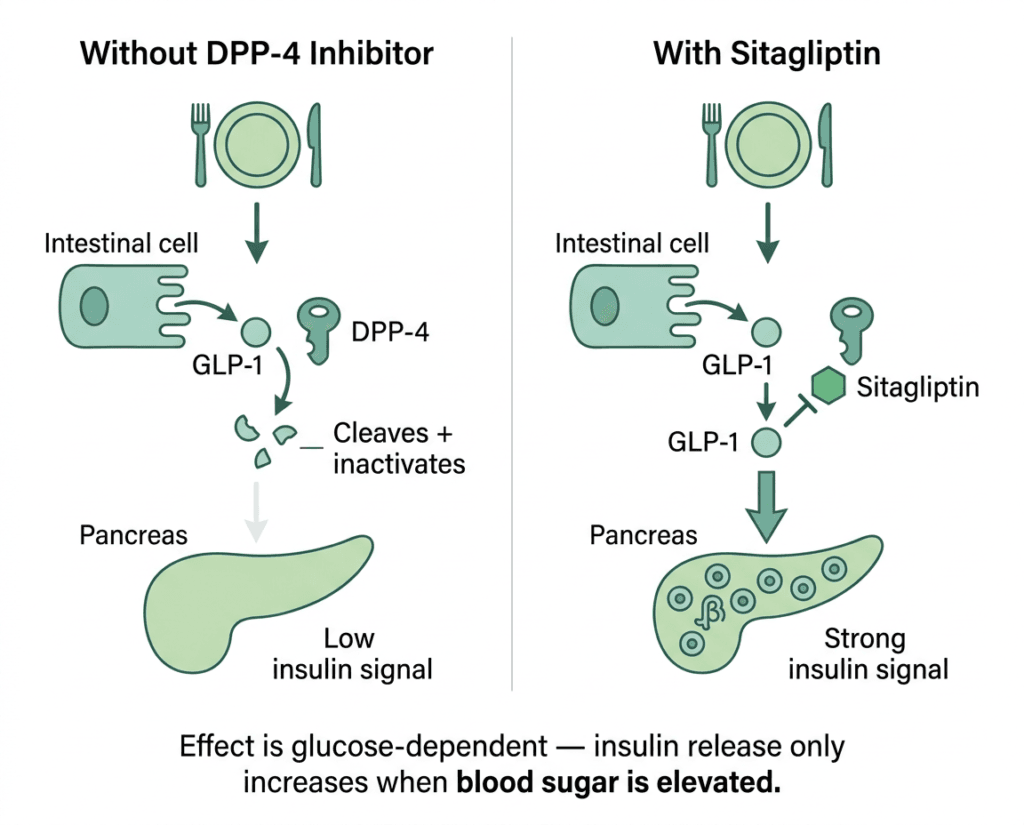
When you eat, specialized cells in the small intestine release hormones called incretins, primarily glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP). These hormones signal the pancreas to increase insulin secretion and, in the case of GLP-1, to suppress glucagon (the hormone that raises blood sugar). The incretin effect amplifies the body’s insulin response to a meal in a glucose-dependent way: it only activates significantly when blood sugar is actually elevated.
The problem in type 2 diabetes is that this incretin response is blunted: both GLP-1 levels and the pancreatic response to incretins are diminished. And even what GLP-1 is released gets destroyed quickly. The enzyme dipeptidyl peptidase-4 (DPP-4) inactivates GLP-1 within minutes of its secretion. This was discovered in the 1990s, and it became the pharmacological rationale for DPP-4 inhibitors: block the enzyme that destroys GLP-1, and more of it survives long enough to do its job.
Sitagliptin is a selective, competitive inhibitor of DPP-4. In patients with type 2 diabetes, a single dose produces DPP-4 inhibition for a full 24-hour period. After a meal or oral glucose load, this inhibition results in a two- to three-fold increase in circulating active GLP-1 and GIP, decreased glucagon concentrations, and increased responsiveness of insulin release to glucose.
The glucose-dependence of this mechanism is the key to why sitagliptin rarely causes hypoglycemia on its own. Because GLP-1 and GIP only stimulate insulin when glucose is actually elevated, DPP-4 inhibition does not push insulin secretion when blood sugar is already in a normal or low range. The risk of hypoglycemia primarily arises when sitagliptin is combined with insulin or a sulfonylurea, agents that cause insulin release independent of glucose levels.
What the Clinical Evidence Shows
Glycemic efficacy
Across clinical trials, sitagliptin as monotherapy or add-on therapy produces HbA1c reductions of approximately 0.5 to 0.8% from baseline. That is a moderate but clinically meaningful reduction, comparable to other agents in the DPP-4 class and positioned below the reductions achieved by GLP-1 receptor agonists, which typically deliver 1.0 to 1.5% or more at higher doses. An 18-week head-to-head trial of 800 patients with inadequately controlled type 2 diabetes on metformin found saxagliptin and sitagliptin produced similar HbA1c reductions, confirming that DPP-4 agents within the class are broadly equivalent on this endpoint.
| Clinical setting | Typical HbA1c reduction | Notes |
|---|---|---|
| Monotherapy | approximately 0.6 to 0.8% | Similar to other DPP-4 inhibitors |
| Add-on to metformin | approximately 0.5 to 0.7% | Most common clinical use |
| Add-on to insulin | approximately 0.4 to 0.6% | Allows insulin dose reduction in some patients |
| Add-on to sulfonylurea | approximately 0.4 to 0.6% | Increases hypoglycemia risk from the sulfonylurea; requires caution |
| Triple therapy (metformin plus sulfonylurea) | approximately 0.6 to 0.7% | Established combination in guidelines |
The FDA approved Januvia for all of these uses. Janumet (sitagliptin 50 mg plus metformin) and Janumet XR were subsequently approved as fixed-dose combinations, simplifying the regimen for patients who need both agents. Generic Janumet is expected by May 2026 and generic Janumet XR by July 2026 per settlement terms, under certain conditions.
Cardiovascular safety: the TECOS trial and what it established
The TECOS trial (NCT00790205) was the FDA-required cardiovascular outcomes trial for sitagliptin. It enrolled 14,671 patients with type 2 diabetes and established cardiovascular disease, randomizing them to sitagliptin or placebo added to existing therapy. The primary outcome, a composite of cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for unstable angina, occurred in 11.4% of sitagliptin patients versus 11.6% of placebo patients (HR 0.98; 95% CI 0.89 to 1.08; p less than 0.001 for non-inferiority). Sitagliptin was cardiovascularly safe: it neither increased nor decreased the risk of major adverse cardiovascular events.
Equally important was the heart failure finding. Sitagliptin did not increase the rate of hospitalization for heart failure. This distinguishes it within the DPP-4 class: saxagliptin in the SAVOR-TIMI 53 study showed a significant 27% increase in heart failure hospitalizations, which prompted the FDA to add a class-level heart failure warning to all DPP-4 inhibitors. That warning is on Januvia’s label, but the sitagliptin-specific TECOS data is reassuring. A re-adjudication of TECOS performed at the FDA’s request confirmed 224 heart failure hospitalization events in the sitagliptin arm and 239 in the placebo arm, numerically favoring sitagliptin. The class warning remains; the drug-specific evidence does not support the concern.
What TECOS did not show is cardiovascular benefit. Sitagliptin does not reduce cardiovascular events the way SGLT2 inhibitors and GLP-1 receptor agonists have been proven to. For patients with established cardiovascular disease, heart failure, or chronic kidney disease, the proven cardiorenal protection of those drug classes is a clinically meaningful advantage that sitagliptin does not share.
Where Sitagliptin Fits in the 2026 Type 2 Diabetes Landscape
This is the most important clinical context for understanding the Januvia LOE story in 2026. Sitagliptin is losing exclusivity at a moment when the treatment paradigm around it has shifted significantly.
The 2020s have been defined by two drug classes achieving benefits well beyond glycemic control. SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin) reduce cardiovascular mortality, hospitalizations for heart failure, and progression of chronic kidney disease, benefits established in landmark outcomes trials across large high-risk populations. GLP-1 receptor agonists (semaglutide, liraglutide, tirzepatide) reduce cardiovascular events, cause substantial weight loss, and in the case of semaglutide, have received FDA approval for both cardiovascular risk reduction and obesity management. The first oral non-peptide GLP-1 receptor agonist, Foundayo (orforglipron), received FDA approval in April 2026, adding a truly unrestricted oral GLP-1 option.
In that landscape, where does a weight-neutral, cardiovascularly neutral oral agent fit?
The answer is: a meaningful clinical niche that still covers millions of patients.
| Drug class | CV benefit proven | Weight effect | Hypoglycemia risk (mono) | Kidney dosing | Oral option |
|---|---|---|---|---|---|
| Metformin | No (but safe) | Modest loss | Low | Reduce in CKD | Yes |
| DPP-4 inhibitors (sitagliptin) | No, cardiovascularly neutral | Neutral | Low | Dose reduction needed (except linagliptin) | Yes |
| SGLT2 inhibitors | Yes: CV, HF, kidney | Modest loss | Low | Reduced efficacy in advanced CKD | Yes |
| GLP-1 receptor agonists (injectable) | Yes (CV outcomes trials) | Significant loss | Low | Generally safe in CKD | No (most) |
| GLP-1 receptor agonists (oral) | CV trial ongoing for some | Significant loss | Low | Generally safe | Yes (semaglutide with restrictions; orforglipron without) |
| Sulfonylureas | No | Weight gain | Significant | Dose reduction needed | Yes |
| Insulin | No | Weight gain | Significant | Flexible | No |
Sitagliptin’s clinical home in 2026 is patients who need a second-line oral agent that is well tolerated, has no hypoglycemia risk as monotherapy, and does not require the complexity of a GLP-1 or the cardiorenal eligibility profile that SGLT2 inhibitors require. That covers a large portion of the type 2 diabetes population, particularly older patients with multiple comorbidities where weight loss is not a primary goal, patients who cannot tolerate GLP-1 gastrointestinal side effects, and patients managed primarily in primary care settings where combination injectable regimens may not be the first choice.
The ADA Standards of Medical Care in Diabetes 2026 continues to recommend DPP-4 inhibitors as a reasonable option for patients who need additional glucose lowering with low hypoglycemia risk and no compelling indication for cardiorenal benefit.
The Safety Profile
| Safety item | Details | Clinical guidance |
|---|---|---|
| Pancreatitis | Postmarketing reports of acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing cases. Causal relationship not definitively established. | Discontinue immediately if pancreatitis is suspected. Do not restart. Not recommended in patients with a history of pancreatitis. |
| Heart failure (class warning) | FDA class-level warning based on saxagliptin data. Sitagliptin-specific TECOS data showed no increased heart failure risk. | The class warning remains on the label but the sitagliptin-specific evidence is reassuring. Discuss with prescriber in patients with known heart failure risk factors. |
| Severe joint pain | Postmarketing cases of severe and disabling arthralgia reported with DPP-4 inhibitors, including sitagliptin. Onset can occur months to years after initiation. | Consider DPP-4 inhibitor as a possible cause of new-onset severe joint pain. Discontinue and reassess. |
| Hypoglycemia | Low risk as monotherapy. Higher risk when combined with insulin or sulfonylurea. | If combined with insulin or a sulfonylurea, lower the dose of the partnering agent to reduce hypoglycemia risk when starting sitagliptin. |
| Renal dosing | Sitagliptin is primarily renally excreted. Dose adjustment required for eGFR below 45 mL/min/1.73m². | Standard dose 100 mg once daily; reduce to 50 mg for eGFR 30 to 45; reduce to 25 mg for eGFR below 30. Check kidney function at baseline and periodically. |
| Hypersensitivity | Serious hypersensitivity reactions including anaphylaxis and angioedema reported postmarketing. | Discontinue immediately; do not restart if a hypersensitivity reaction occurred. |
| Bullous pemphigoid | Postmarketing reports of bullous pemphigoid (a serious skin blistering condition) with DPP-4 inhibitors. | Discontinue if bullous pemphigoid develops. |
The Generic Landscape: What to Expect in 2026 and 2027
The sitagliptin generics story has two distinct threads.
Zituvio (sitagliptin free base, Zydus): FDA-approved in October 2023. Zituvio contains sitagliptin in a different chemical form (free base rather than the phosphate salt used in Januvia). It is not bioequivalent to Januvia and cannot be automatically substituted by a pharmacist, but a prescriber can write a new prescription for it specifically. At select specialty pharmacies including Marley Drug, sitagliptin in this form has been available for approximately $80 per month. This is already an accessible option for patients who know to ask about it.
True generic Januvia (sitagliptin phosphate): A generic version of Januvia was approved by Watson Labs (now Viatris) on December 30, 2025, as sitagliptin phosphate. Settlement agreements between Merck and at least 21 generic manufacturers allow launch as early as May 2026. The core Januvia patent expires November 24, 2026. When multiple generics are in the market, prices are expected to fall 80 to 85%, potentially to $50 to $100 per month.
The scale of this LOE is significant. In Q1 2026, Merck’s Januvia/Janumet franchise generated $574 million, down 28% from $796 million in Q1 2025, with the decline attributed primarily to lower pricing in the U.S. and generic competition in international markets. The U.S. decline, when it arrives fully after the November patent expiration, will be steeper.
For the broader healthcare system, the price reduction from Januvia’s LOE is among the most consequential access stories of 2026. Nearly 8 million Januvia prescriptions were filled in 2022. When per-prescription costs fall by 80 to 85%, the system-wide savings are in the billions of dollars annually, and millions of patients who have been cost-sharing or going without will have a path to affordable access.
The Janumet and Janumet XR situation
The Janumet fixed-dose combination has a slightly different patent picture. Merck’s patent covering the sitagliptin-metformin co-formulation expires in November 2026, but a separate patent on the co-formulation was defended successfully in litigation against Viatris, potentially giving Janumet XR additional protection. Settlement agreements nonetheless allow Janumet generics by May 2026 and Janumet XR generics by July 2026 under certain conditions.
For patients on Janumet, the combination’s value is primarily simplicity: one pill instead of two. When both sitagliptin and metformin are available as inexpensive generics separately, the question of whether the combination tablet justifies any remaining price premium becomes less pressing.
What This Means for Patients
If you are currently taking Januvia and your blood sugar is well controlled, nothing about your clinical situation requires you to change anything immediately. Generic sitagliptin phosphate with FDA approval is therapeutically equivalent to Januvia.
What to watch for: formulary notifications from your insurer, and conversations with your pharmacist about when generic sitagliptin becomes available on your plan’s formulary. Going from $600 a month to $80 to $100 a month for the same drug is not a minor convenience. For patients who have been managing this cost for years, it is a significant change in financial burden.
If cost has already been an issue and you have been managing with partial doses, delayed refills, or skipping months: ask your prescriber or pharmacist right now about Zituvio or authorized generic sitagliptin at pharmacies that already offer it in the $80-per-month range. You do not need to wait for the November patent expiration to access a substantially lower-cost version of this drug.
One practical note on renal dosing: generics will be available in all three strengths, 25 mg, 50 mg, and 100 mg, corresponding to the Januvia label. Patients with reduced kidney function who currently take a lower dose of Januvia should confirm that their generic prescription specifies the same strength. Dose substitution errors are a real dispensing risk when a drug transitions from brand to generic, and this is worth verifying at pickup.
For related HED coverage on diabetes treatment advances in 2026, see our post on Awiqli, the first once-weekly basal insulin for type 2 diabetes, our post on Foundayo (orforglipron), the first oral GLP-1 receptor agonist with no food or water restrictions, and our post on Langlara, the third interchangeable insulin glargine biosimilar, and what it means for insulin access.
Sources
Generic sitagliptin timeline and pricing: Januvia (Sitagliptin) 2026 Availability, Prices and Tips to Find. Medfinder. April 2026.
Merck patent settlements: Merck defends blockbuster Januvia franchise from patent challenge. Pharmaphorum. September 2022. | Merck prevails in high-stakes patent lawsuit against Viatris. Fierce Pharma. September 2022.
Merck Q1 2026 financial results: Merck Form 8-K: Januvia/Janumet Q1 2026 revenues $574 million, down 28%. SEC.gov.
Patent cliff overview: Blockbuster drugs face a massive patent cliff in 2026. Drug Discovery News. February 2026.
DPP-4 mechanism (incretin system): Ahrén B. DPP-4 Inhibition and the Path to Clinical Proof. Frontiers in Endocrinology. 2019. PMC6593050.
DPP-4 inhibitor class review: Role of DPP-4 Inhibitors in the Treatment Algorithm of T2DM. PMC6696077.
DPP-4 inhibitors (StatPearls): Dipeptidyl Peptidase IV (DPP-4) Inhibitors. StatPearls. NCBI.
GLP-1 biology: Glucagon-Like Peptide 1. StatPearls. NCBI.
TECOS trial primary publication: Green JB et al. Effect of Sitagliptin on Cardiovascular Outcomes in Type 2 Diabetes. NEJM. 2015;373:232–242. doi:10.1056/NEJMoa1501352.
TECOS trial registration: NCT00790205. ClinicalTrials.gov.
TECOS heart failure re-adjudication: Scirica BM et al. Re-adjudication of TECOS with study-level meta-analysis of hospitalization for heart failure from CV outcomes trials with DPP-4 inhibitors. Clinical Cardiology. 2022. PMC9286326.
Januvia FDA approval: FDA approves sitagliptin for type 2 diabetes. FDA.gov.
Janumet FDA approval: FDA approves sitagliptin/metformin combination tablet. FDA.gov.
Januvia prescribing information: JANUVIA (sitagliptin) Prescribing Information. Merck.
Zituvio generic availability: Generic Zituvio Availability. drugs.com.
ADA Standards 2026: Standards of Medical Care in Diabetes 2026. Diabetes Care. American Diabetes Association.
SGLT2 inhibitors overview: SGLT2 Inhibitors. StatPearls. NCBI.
Metformin: Metformin. StatPearls. NCBI.
Sulfonylureas: Sulfonylureas. StatPearls. NCBI.
Insulin: Insulin. StatPearls. NCBI.
Pancreatitis: Acute Pancreatitis. StatPearls. NCBI.
Hypoglycemia: Hypoglycemia. StatPearls. NCBI.
Diabetic kidney disease: Diabetic Kidney Disease. NIDDK.
CDC diabetes statistics: National Diabetes Statistics Report. CDC.
Empagliflozin CV benefit: FDA approves empagliflozin to reduce risk of cardiovascular death. FDA.gov.
HED internal references: Foundayo (orforglipron) FDA approval post | Awiqli once-weekly insulin post | Langlara interchangeable biosimilar insulin post
Patient resources: American Diabetes Association | Merck Patient Assistance Program | NeedyMeds | Marley Drug (low-cost generics)
| Disclaimer: Health Evidence Digest provides general information about FDA approvals, loss of exclusivity events, and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Decisions about diabetes medications, including switching from brand-name to generic sitagliptin, should be made in consultation with your prescribing clinician, who can account for your full medical history, current kidney function, and other medications. Drug pricing information reflects figures at time of publication and is subject to change. |
|---|
Leave a Reply