| 📌 The essentials On June 24, 2026, the FDA approved a new indication for Tryngolza (olezarsen, Ionis Pharmaceuticals) as an adjunct to diet to reduce triglycerides and the risk of acute pancreatitis in adults with severe hypertriglyceridemia (sHTG: fasting triglycerides at or above 500 mg/dL). This makes Tryngolza the first and only therapy approved specifically to reduce the risk of acute pancreatitis in this population. Tryngolza was originally approved in December 2024 for adults with familial chylomicronemia syndrome (FCS), a rare monogenic form of sHTG affecting roughly 3,000 to 5,000 people in the U.S. The new sHTG indication covers approximately 3 million Americans who have severe hypertriglyceridemia from multiple non-monogenic causes. Mechanism: olezarsen is a GalNAc-conjugated antisense oligonucleotide (ASO) that targets apolipoprotein C-III (apoC-III) mRNA in hepatocytes, reducing apoC-III production. ApoC-III inhibits lipoprotein lipase (LPL), the enzyme responsible for clearing triglyceride-rich lipoproteins from the bloodstream. By reducing apoC-III, olezarsen restores LPL activity and promotes clearance of triglycerides through both LPL-dependent and LPL-independent pathways. The clinical basis: Phase 3 CORE-TIMI 72a (NCT05079919, n=617) and CORE2-TIMI 72b (NCT05552326, n=446), conducted with The TIMI Study Group. Mean baseline triglycerides: 1,116 mg/dL. Placebo-adjusted triglyceride reduction at 6 months: up to 72% (80 mg dose) in CORE, sustained through 12 months. Acute pancreatitis events: 85% reduction in pooled analyses; pooled rate ratio 0.15 (95% CI 0.05 to 0.40; p less than 0.001). Patients achieving triglycerides below 500 mg/dL: 86%. Primary NEJM publication: Marston NA et al. NEJM. 2025. doi:10.1056/NEJMoa2512761. Regulatory designations: Priority Review; Breakthrough Therapy designation (November 2025). Dosing: 50 mg or 80 mg subcutaneous injection once monthly via autoinjector. Available in the U.S. July 2026. Key safety considerations: injection site reactions; liver enzyme elevations; dose-dependent hepatic fat fraction increases; more thrombocytopenia with 80 mg dosing. |
|---|
Hypertriglyceridemia is one of the most undertreated serious lipid disorders in clinical medicine. While elevated LDL cholesterol commands the vast majority of attention in cardiovascular risk management, very high triglycerides carry their own distinct and devastating clinical consequence: acute pancreatitis. When fasting triglycerides reach approximately 500 mg/dL and above, the risk of severe, recurrent, and potentially fatal pancreatitis rises substantially. At levels above 1,000 mg/dL, the risk becomes acutely dangerous.
And until June 24, 2026, no FDA-approved therapy had ever demonstrated that it could reduce the risk of acute pancreatitis in patients with severe hypertriglyceridemia. Fibrates, fish oils, and niacin lower triglycerides in this population, but none of them had generated the clinical trial evidence showing that their triglyceride reduction translated into fewer pancreatitis events.
Tryngolza (olezarsen, Ionis Pharmaceuticals) is the first. The Phase 3 CORE and CORE2 trials, involving 1,061 adults with fasting triglycerides at or above 500 mg/dL and a mean baseline level of 1,116 mg/dL, demonstrated an 85% reduction in acute pancreatitis events and up to 72% reduction in triglycerides compared to placebo — and did so with a once-monthly subcutaneous injection targeting the same molecular pathway responsible for the most severe form of this disease.
This post covers what severe hypertriglyceridemia is and why pancreatitis is its most feared consequence, how the apoC-III mechanism drives triglyceride accumulation and why targeting it with an antisense oligonucleotide represents a fundamentally different approach from existing therapies, what the CORE and CORE2 trials showed, the safety profile of olezarsen, how it relates to the original FCS indication, and what this approval means for the much larger population of Americans with severe hypertriglyceridemia.
What Severe Hypertriglyceridemia Is and Why It Causes Pancreatitis
Triglycerides are the primary form of dietary fat storage in the body. After meals, triglycerides are packaged into chylomicrons in the intestine and released into the bloodstream, where they are broken down by lipoprotein lipase (LPL). Between meals, the liver packages triglycerides into very low-density lipoprotein (VLDL) for transport and distribution. Under normal conditions, fasting triglycerides are below 150 mg/dL.
Severe hypertriglyceridemia is defined as fasting triglycerides at or above 500 mg/dL. At this level, the body’s triglyceride clearance machinery is overwhelmed: chylomicrons and VLDL remain in the circulation at pathologically elevated concentrations. The population affected in the United States is substantial, approximately 3 million adults, arising from combinations of genetic predisposition, metabolic conditions (type 2 diabetes, obesity, hypothyroidism), alcohol use, and medications that raise triglycerides (corticosteroids, certain antipsychotics, estrogens, beta-blockers).
Why hypertriglyceridemia causes pancreatitis
The mechanism by which very high triglycerides cause acute pancreatitis is not fully elucidated but involves the accumulation of triglyceride-rich lipoproteins (chylomicrons) in the pancreatic capillaries. Pancreatic lipase, the same enzyme that normally digests dietary fat in the intestine, hydrolyzes these accumulated triglycerides locally in the pancreatic microcirculation. The free fatty acids released from this hydrolysis are directly toxic to pancreatic acinar cells, producing the inflammatory cascade of acute pancreatitis. The pathological cycle is self-amplifying: local tissue damage increases vascular permeability, concentrating triglycerides further in the pancreatic bed.
Hypertriglyceridemia-induced acute pancreatitis differs from gallstone or alcohol-induced pancreatitis in several clinically important ways. Patients often present with more severe disease at initial diagnosis. The condition is highly recurrent: patients who have had one episode remain at high risk for subsequent attacks as long as triglycerides remain uncontrolled. Repeated episodes of acute pancreatitis cause cumulative damage including pancreatic fibrosis, exocrine insufficiency, and secondary diabetes. And the acute attacks themselves can be life-threatening, with mortality rates of 5 to 10% per episode from severe pancreatitis.
| Why the existing therapies for hypertriglyceridemia have never been sufficient for this population Fibrates (fenofibrate, gemfibrozil), omega-3 fatty acids (Vascepa, Lovaza), and niacin all lower triglycerides to varying degrees in patients with sHTG. For mild-to-moderate hypertriglyceridemia, these agents are appropriate. For severe hypertriglyceridemia (triglycerides at or above 500 mg/dL), the problem is twofold: the degree of triglyceride reduction achievable with these agents is often insufficient to bring triglycerides below the 500 mg/dL danger threshold, and — critically — none of these therapies had ever demonstrated in a randomized controlled trial that their triglyceride-lowering translated into fewer pancreatitis events. They lower triglycerides. They do not have regulatory approval for reducing pancreatitis risk. For patients with sHTG who have been told to take a fibrate and a fish oil and watch their diet, this approval addresses the most important clinical gap in their management. |
|---|
The Science: How apoC-III Drives Triglyceride Accumulation and Why Blocking It Works
Understanding olezarsen’s mechanism requires understanding the central role of apolipoprotein C-III (apoC-III) in triglyceride metabolism.
ApoC-III is a small apolipoprotein produced primarily in the liver. It acts as a major inhibitor of triglyceride clearance through two distinct mechanisms:
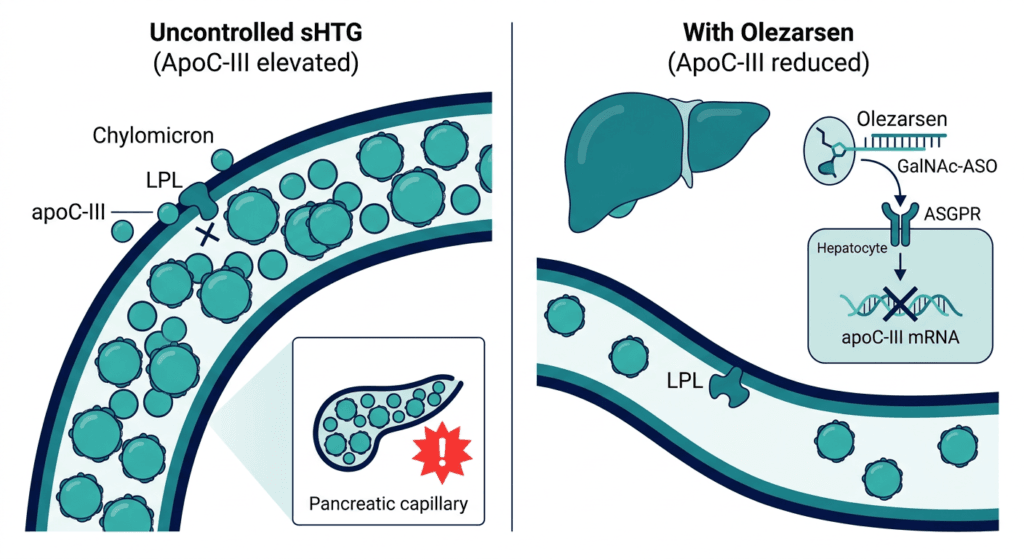
LPL inhibition: LPL is the enzyme that sits on the surface of capillary endothelial cells throughout the body and hydrolyzes the triglycerides in circulating VLDL and chylomicrons, releasing fatty acids for energy use or storage. ApoC-III, when present on the surface of these triglyceride-rich lipoproteins, directly inhibits LPL activity. When apoC-III levels are high, LPL cannot efficiently break down triglycerides, and triglyceride-rich lipoproteins accumulate in the bloodstream.
Impaired hepatic remnant uptake: Beyond LPL inhibition, apoC-III also blocks the hepatic receptors responsible for removing triglyceride-rich lipoprotein remnants from the bloodstream after partial hydrolysis. This means that even the breakdown products of VLDL and chylomicron hydrolysis accumulate in circulation when apoC-III is elevated.
In patients with sHTG, both mechanisms contribute to the massive triglyceride accumulation. Some patients have genetic variants that increase apoC-III expression directly; others have metabolic conditions that drive excess apoC-III production; all share the downstream consequence of overwhelmed LPL and impaired remnant clearance.
How olezarsen targets apoC-III: the GalNAc-ASO approach
Olezarsen is an antisense oligonucleotide (ASO) — a short, synthetic strand of modified RNA designed to bind to the messenger RNA (mRNA) that encodes apoC-III in the liver. When the ASO binds to its target mRNA, it recruits RNase H, an enzyme that degrades the bound RNA strand. With the mRNA destroyed, the ribosome cannot translate it into apoC-III protein. Hepatic apoC-III production decreases substantially and persistently.
What makes olezarsen a next-generation ASO is its GalNAc (N-acetyl galactosamine) conjugation. Three GalNAc molecules are attached to the olezarsen molecule in a triantennary arrangement. GalNAc is a high-affinity ligand for the asialoglycoprotein receptor (ASGPR) expressed almost exclusively on hepatocytes. When the GalNAc-conjugated ASO enters the bloodstream, hepatocytes recognize and rapidly internalize it through receptor-mediated endocytosis. The result: the drug is delivered with exceptional precision to the liver cells where apoC-III is produced, achieving equivalent apoC-III knockdown at doses far lower than first-generation ASOs that relied on non-targeted distribution.
The practical significance of the GalNAc targeting is not only efficacy. First-generation apoC-III ASOs like volanesorsen caused significant thrombocytopenia (low platelet counts) because systemic ASO distribution led to off-target interaction with platelets and the reticuloendothelial system. The GalNAc-mediated hepatic uptake of olezarsen reduces systemic ASO exposure substantially, greatly reducing platelet-related side effects. As a result, patients treated with olezarsen do not require the same intensive platelet monitoring that volanesorsen demanded, simplifying outpatient management considerably.
The CORE and CORE2 Trials: What the Data Shows
Trial design
CORE-TIMI 72a (NCT05079919) and CORE2-TIMI 72b (NCT05552326) were two Phase 3, global, multicenter, randomized, double-blind, placebo-controlled trials conducted in collaboration with The TIMI Study Group. Together they enrolled 1,061 adults (617 in CORE; 446 in CORE2) with fasting triglycerides at or above 500 mg/dL who were already on standard-of-care therapies for elevated triglycerides.
The extremely high baseline mean triglyceride level of 1,116 mg/dL in enrolled patients reflects the severity of sHTG being targeted. At baseline, 47% of CORE participants and 37% of CORE2 participants had fasting triglycerides at or above 880 mg/dL, well into the range where pancreatitis risk is acute.
Patients were randomized to olezarsen 50 mg once monthly, olezarsen 80 mg once monthly, or placebo via subcutaneous injection, for 12 months. The primary endpoint was placebo-adjusted percent change in fasting triglycerides from baseline to month 6. The results were published in the New England Journal of Medicine in November 2025.
Primary endpoint: triglyceride reduction
| Trial | Dose | Placebo-adjusted TG reduction at 6 months | p-value | Sustained at 12 months |
|---|---|---|---|---|
| CORE | 50 mg | 63% | p less than 0.001 | Yes |
| CORE | 80 mg | 72% | p less than 0.001 | Yes |
| CORE2 | 50 mg | 49% | p less than 0.001 | Yes |
| CORE2 | 80 mg | 55% | p less than 0.001 | Yes |
These are substantial reductions in a patient population starting from a mean triglyceride of 1,116 mg/dL. A 72% reduction from 1,116 mg/dL would bring the mean to approximately 312 mg/dL, below the 500 mg/dL acute pancreatitis risk threshold.
Secondary endpoint: acute pancreatitis events
The acute pancreatitis endpoint is the most clinically significant finding in the CORE and CORE2 program. At 12 months, in the pooled population across both trials:
| Outcome | Pooled olezarsen | Pooled placebo |
|---|---|---|
| Acute pancreatitis events | 7 events in 5 patients | 22 events in 17 patients |
| Rate ratio (pooled) | 0.15 (95% CI 0.05 to 0.40) | Reference |
| Reduction in acute pancreatitis events | 85% | — |
| p-value | p less than 0.001 | — |
| Patients achieving TG below 500 mg/dL | 86% | — |
Dr. Nicholas Marston, MD, MPH, cardiologist at Brigham and Women’s Hospital and Harvard Medical School, and principal investigator for the CORE program, noted that these were the first studies to show a significant reduction in acute pancreatitis events in sHTG, and that with most patients on olezarsen achieving triglyceride levels below the risk threshold for those potentially life-threatening episodes, the results represent a major advance for patients with recurrent pancreatitis.
Secondary lipid endpoints
Beyond triglycerides, olezarsen produced favorable changes across the broader lipid panel in CORE and CORE2:
- Substantial reductions in apoC-III itself (the direct molecular target)
- Reductions in remnant cholesterol
- Reductions in non-HDL cholesterol
- Reductions in VLDL cholesterol
- Increases in HDL cholesterol (the protective lipoprotein)
- Reductions in apolipoprotein B-containing lipoproteins
These secondary lipid findings are relevant to the question of whether olezarsen’s benefits extend beyond pancreatitis prevention to cardiovascular risk reduction, a question that the ongoing ESSENCE trial in moderate hypertriglyceridemia with established cardiovascular disease is designed to address.
Tryngolza’s Complete Indication Picture After June 2026
| Indication | Population | Approval date |
|---|---|---|
| Reduce triglycerides in adults with familial chylomicronemia syndrome (FCS) | Adults with confirmed genetic FCS | December 19, 2024 |
| Reduce triglycerides and the risk of acute pancreatitis in adults with severe hypertriglyceridemia (sHTG) | Adults with fasting TG at or above 500 mg/dL | June 24, 2026 |
FCS is a rare monogenic disorder affecting 3,000 to 5,000 people in the United States, caused by biallelic loss-of-function mutations in genes encoding LPL or its essential cofactors, resulting in complete or near-complete absence of LPL activity. The sHTG population, now the larger approved indication, includes patients with polygenic triglyceride elevation, secondary causes, or a combination of genetic susceptibility plus metabolic or lifestyle factors.
The mechanistic basis for olezarsen’s efficacy across both conditions is the same: in both FCS and sHTG, apoC-III elevation contributes to insufficient triglyceride clearance. In FCS, LPL is absent or dysfunctional and apoC-III’s LPL-independent effects on remnant clearance are particularly relevant. In sHTG from other causes, restoring LPL activity by reducing apoC-III is the primary mechanism.
Dosing and Administration
Tryngolza is available in two doses: 50 mg and 80 mg, both self-administered once monthly via subcutaneous autoinjector. The injection can be administered in the abdomen, thigh, or upper arm.
The 80 mg dose produced somewhat greater triglyceride reduction in the CORE trials (72% vs. 63%) but is associated with more adverse effects including dose-dependent hepatic fat fraction increases and higher rates of thrombocytopenia. The appropriate dose for a given patient is a clinical decision based on baseline triglyceride level, risk stratification, and tolerability.
The once-monthly dosing schedule is a meaningful practical advantage. Standard-of-care fibrate therapy requires once-daily oral dosing (or twice daily for some formulations), and omega-3 fatty acids require 4 capsules daily. A single monthly injection removes the daily medication burden for the most critical component of triglyceride management in this population.
Tryngolza will be available in U.S. pharmacies beginning July 2026.
Safety: What the Prescribing Information and Trial Data Cover
The safety profile of olezarsen in CORE and CORE2 was generally favorable, with most adverse events mild in severity. Notably, serious adverse events were less frequent in olezarsen-treated patients than in the placebo group, likely reflecting the reduction in pancreatitis hospitalizations.
| Safety item | Details | Clinical guidance |
|---|---|---|
| Injection site reactions | Most common adverse event; generally mild (redness, bruising, pain); consistent with the subcutaneous injection class | Rotate injection sites. Mild reactions typically resolve without intervention. |
| Liver enzyme elevations | ALT and AST increases observed; greater with 80 mg dosing | Baseline liver function testing; monitor as clinically indicated. |
| Hepatic fat fraction increase | Dose-dependent; greater with 80 mg; clinical significance of hepatic fat accumulation under long-term treatment requires monitoring | Discuss with patients who have pre-existing hepatic steatosis; liver function monitoring recommended. |
| Thrombocytopenia | More common with 80 mg than 50 mg; less severe than observed with volanesorsen (first-generation apoC-III ASO); clinically significant platelet declines were infrequent and reversible | Baseline platelet count; periodic monitoring during therapy, more vigilant with 80 mg dosing. |
| Hypersensitivity reactions | Serious hypersensitivity reactions requiring medical treatment have occurred | Contraindicated in patients with a history of serious hypersensitivity to olezarsen or any excipient. |
| Embryo-fetal toxicity | Animal studies showed adverse developmental effects; potential fetal harm | Females of reproductive potential: use effective contraception during treatment. |
Contraindication:
Tryngolza is contraindicated in patients with a history of serious hypersensitivity reactions to olezarsen or any of the product excipients.
The GalNAc-conjugated design of olezarsen is clinically relevant to the thrombocytopenia profile. Volanesorsen, the first-generation apoC-III ASO approved in Europe for FCS, caused severe, sometimes immune-mediated thrombocytopenia that required intensive platelet monitoring and led to treatment discontinuation in a meaningful proportion of patients. Olezarsen’s hepatocyte-targeted delivery dramatically reduces systemic ASO exposure, and the lower platelet toxicity signal observed in CORE and CORE2 reflects this. Patients treated with olezarsen require monitoring but not the intensive surveillance that volanesorsen demanded.
What This Means for Patients and Clinicians
For the approximately 3 million Americans with severe hypertriglyceridemia
This approval provides the first therapy specifically shown in randomized controlled trials to reduce acute pancreatitis events. For patients who have experienced one or more episodes of hypertriglyceridemia-induced pancreatitis — a population that knows intimately what the hospitalization, pain, and recovery looks like — the 85% reduction in pancreatitis events in CORE and CORE2 is the most important number in this approval.
For patients currently on fibrates and fish oils with triglycerides still above 500 mg/dL: the addition of olezarsen as an adjunct to diet and existing therapy is now an evidence-supported option. The trials enrolled patients already on standard-of-care therapies, meaning the CORE and CORE2 data reflects real-world patients who had not achieved adequate control on existing agents.
For clinicians managing lipid disorders
The approval creates a new treatment algorithm decision point: patients with confirmed fasting triglycerides at or above 500 mg/dL, particularly those with a history of pancreatitis, should now be evaluated for Tryngolza as an add-on to current triglyceride-lowering therapy. The once-monthly subcutaneous autoinjector, the absence of significant drug-drug interactions with common triglyceride-lowering agents, and the favorable tolerability profile in CORE and CORE2 make this a manageable addition to complex lipid management regimens.
The liver function and platelet monitoring requirements are straightforward and consistent with standard care for patients on lipid-active therapies. The hepatic fat fraction consideration is worth discussing with patients who have pre-existing metabolic-associated fatty liver disease, a common comorbidity in the sHTG population.
The FCS distinction
Patients with confirmed familial chylomicronemia syndrome remain a distinct population. FCS, defined by biallelic loss-of-function mutations in LPL or essential cofactors with complete or near-complete absence of LPL activity, carries a more severe clinical course and is the population for which Tryngolza’s original December 2024 approval was granted. FCS patients may have different dose considerations and monitoring needs from the broader sHTG population; management in these patients should involve a lipidologist or endocrinologist with experience in genetic lipid disorders.
For the broader sHTG population without confirmed monogenic disease: Tryngolza is now available in both primary care and specialist settings where appropriate patient selection, baseline testing, and monitoring can be provided.
For related HED coverage on lipid management and cardiometabolic health, see our post on Foundayo (orforglipron), the first oral GLP-1 receptor agonist with no food or water restrictions, approved for obesity management in 2026, and our post on Januvia (sitagliptin) losing exclusivity and what generic sitagliptin means for the type 2 diabetes treatment landscape.
Sources
Ionis FDA approval press release: TRYNGOLZA (olezarsen) approved by the FDA as the first and only treatment to reduce triglycerides and the risk of acute pancreatitis in patients with severe hypertriglyceridemia. Ionis Pharmaceuticals. BusinessWire. June 24, 2026.
Drugs.com approval news: Tryngolza (olezarsen) Approved to Reduce Triglycerides and the Risk of Acute Pancreatitis. drugs.com. June 24, 2026.
HCPLive clinical coverage: FDA Approves Olezarsen (Tryngolza) for Severe Hypertriglyceridemia. hcplive.com. June 2026.
Endocrinology Advisor clinical summary: Tryngolza Approved to Reduce Triglycerides and Pancreatitis Risk in sHTG. endocrinologyadvisor.com. June 2026.
Pharmacy Times clinical review: Olezarsen Receives FDA Approval to Reduce Triglycerides, Risk of Acute Pancreatitis in Severe Hypertriglyceridemia. pharmacytimes.com. June 2026.
AHA gastroenterology news: FDA approves olezarsen to reduce acute pancreatitis risk in severe hypertriglyceridemia. news.gastro.org. June 2026.
CORE/CORE2 primary NEJM publication: Marston NA et al. Olezarsen for managing severe hypertriglyceridemia and pancreatitis risk. New England Journal of Medicine. 2025. doi:10.1056/NEJMoa2512761.
CORE trial registration: NCT05079919. ClinicalTrials.gov.
CORE2 trial registration: NCT05552326. ClinicalTrials.gov.
CORE/CORE2 trial design and rationale: Bergmark BA et al. Design and rationale of the CORE-TIMI 72a and CORE2-TIMI 72b trials of olezarsen. American Heart Journal. 2025;286:116–124.
ESSENCE trial (moderate HTG, CV outcomes): Olezarsen in Moderate Hypertriglyceridemia. NEJM. 2025. doi:10.1056/NEJMoa2507227.
Olezarsen mechanism and GalNAc-ASO review: Olezarsen: A Next-Generation Antisense Therapy. Cureus. PMC12700839.
Olezarsen and FCS original approval review: Olezarsen: FDA approval and clinical impact in FCS. PMC12577896.
ApoC-III mechanism and TRL metabolism: JACC Focus Seminar on apoC-III and TRL-lowering therapies. JACC. 2021;78(18):1817–1830.
Triglycerides and metabolic syndrome overview: Blood Triglycerides. NHLBI.
Acute pancreatitis overview: Acute Pancreatitis. StatPearls. NCBI.
Thrombocytopenia: Thrombocytopenia. StatPearls. NCBI.
Tryngolza prescribing information: TRYNGOLZA (olezarsen) Prescribing Information. Ionis Pharmaceuticals. 2026.
Tryngolza approval history: Tryngolza FDA Approval History. drugs.com.
Patient resources: National Lipid Association (lipid.org) | American Heart Association: Triglycerides | FCS patient community: AMAG FCS Foundation | Ionis Tryngolza patient resources
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice. Decisions about initiating Tryngolza for severe hypertriglyceridemia or familial chylomicronemia syndrome should be made in consultation with a qualified clinician, such as a lipidologist, cardiologist, or endocrinologist, who can evaluate baseline triglyceride levels, liver function, platelet counts, and the full clinical context including history of pancreatitis and concurrent medications. |
|---|
Leave a Reply