
| 📌 The essentials Cavhanza (nilotinib, Cycle Pharmaceuticals/Flex Pharma) is a new orally disintegrating tablet (ODT) formulation of nilotinib, a second-generation BCR-ABL tyrosine kinase inhibitor (TKI), approved by the FDA for the treatment of adult patients with Philadelphia chromosome-positive chronic myeloid leukemia (Ph+ CML). Indications: newly diagnosed Ph+ CML in chronic phase, and Ph+ CML in chronic or accelerated phase with resistance or intolerance to prior therapy including imatinib (Gleevec). This is the same clinical indication as Tasigna (nilotinib capsules, Novartis) — the FDA approval of the ODT version was supported by the established efficacy and safety data from Tasigna’s well-controlled trials. What makes Cavhanza different: the nilotinib molecule is unchanged. The innovation is pharmaceutical delivery. The ElectroNanoSpray (ENS) proprietary technology used by Flex Pharma produces nanoparticle-sized drug particles with dramatically improved solubility and dissolution rate. The result: Cavhanza maintains bioavailability when taken with proton pump inhibitors (PPIs) or histamine H2 receptor antagonists (H2RAs) — acid reducers that substantially reduce Tasigna’s absorption and are currently contraindicated with it. No food effect: Cavhanza can be taken without regard to meals. Standard nilotinib capsules require fasting (no food 2 hours before and 1 hour after each dose) because food substantially increases absorption and can raise drug levels to toxic ranges. The clinical problem this solves: approximately 25% of Ph+ CML patients are co-prescribed PPIs or H2RAs for conditions such as GERD, peptic ulcer disease, or gastroesophageal reflux. With standard nilotinib, these patients face a choice between undertreating their leukemia (due to reduced TKI absorption) or undertreating their GI condition (by stopping the acid reducer). Cavhanza eliminates this compromise. Dosing: consistent with Tasigna: 300 mg orally twice daily for newly diagnosed CML-CP; 400 mg orally twice daily for resistant or intolerant CML-CP and CML-AP. Can be swallowed whole or allowed to dissolve in the mouth before swallowing; can be taken with or without water. Regulatory basis: 505(b)(2) NDA pathway, referencing Tasigna’s clinical efficacy data. The studies showed no difference in the rate or extent of nilotinib absorption whether the ODT was swallowed whole or dissolved in the mouth. |
|---|
Chronic myeloid leukemia is one of the most remarkable success stories in oncology’s history. Before 2001, a diagnosis of CML in chronic phase carried a median survival measured in years. The discovery that the BCR-ABL fusion oncogene drives CML, and the subsequent development of imatinib (Gleevec) as the first targeted BCR-ABL inhibitor, transformed CML from a reliably fatal malignancy into a manageable chronic condition. Today, patients on first- or second-generation TKI therapy have survival rates that approach those of the general population.
But managing a chronic leukemia requires sustained, reliable drug exposure, and for a meaningful proportion of CML patients that has been harder to achieve than the simple instruction to “take your pill twice a day” implies. Nilotinib (Tasigna), one of the most effective second-generation TKIs, has two well-documented, compliance-limiting properties: it cannot be taken with food, and it cannot be taken with the acid-reducing medications that 25% of CML patients regularly need.
Cavhanza (nilotinib ODT, Cycle Pharmaceuticals), approved in June 2026, is the pharmaceutical engineering answer to both of those problems. The nilotinib molecule is unchanged. The delivery technology is entirely new. And the clinical consequence is that a patient who needs both a TKI and a proton pump inhibitor no longer has to choose between them.
What CML Is and Why the BCR-ABL Target Changed Everything
Chronic myeloid leukemia is a clonal myeloproliferative neoplasm caused by a specific and well-characterized genetic abnormality: the Philadelphia chromosome. The Philadelphia chromosome results from a translocation between chromosomes 9 and 22, creating the fusion gene BCR-ABL1. The BCR-ABL1 protein is a constitutively active tyrosine kinase: unlike normal ABL kinase, which requires external activation signals, BCR-ABL constantly fires, driving uncontrolled myeloid cell proliferation.
This single molecular event — a translocation creating a permanently active kinase — is the driver of CML in the chronic phase for virtually every patient with the disease. That singular, druggable target is what made CML the proving ground for precision oncology.
CML has three clinical phases, reflecting disease progression if untreated or inadequately treated:
| Phase | Definition | Clinical characteristics |
|---|---|---|
| Chronic phase (CML-CP) | Less than 10% blasts in peripheral blood or bone marrow | Most patients at diagnosis; generally manageable with oral TKI therapy; good prognosis with treatment |
| Accelerated phase (CML-AP) | 10 to 19% blasts; specific cytogenetic or hematologic criteria | Intermediate stage; higher risk of progression; still potentially responsive to TKI therapy |
| Blast phase (CML-BP) | More than 20% blasts; resembles acute leukemia | Rapid deterioration; TKI therapy less effective; often requires intensive chemotherapy |
The goal of TKI therapy in CML-CP is to achieve and maintain major molecular response (MMR), defined as BCR-ABL1 transcript levels at or below 0.1% on the International Scale (IS). Achieving MMR correlates strongly with preventing progression to accelerated or blast phase, and deep molecular responses (MR4, MR4.5) are associated with the possibility of treatment-free remission (TFR) in a proportion of patients. The monitoring of BCR-ABL1 transcript levels by PCR is standard practice, typically every 3 months during the first year of therapy and every 3 to 6 months thereafter.
Where Nilotinib Fits in the CML Treatment Landscape
CML now has five approved BCR-ABL TKIs in the United States, each targeting the same fundamental kinase but with different potency profiles, off-target activity, side effect patterns, and approved indications:
| Agent | Generation | FDA-approved indications (adults) | Notable features |
|---|---|---|---|
| Imatinib (Gleevec, generics) | First | Newly diagnosed CML-CP; imatinib-intolerant/resistant CML-CP/AP/BP | First-in-class; extensive long-term data; generic available |
| Nilotinib (Tasigna, Cavhanza) | Second | Newly diagnosed CML-CP; resistant/intolerant CML-CP and CML-AP | Higher affinity for BCR-ABL; superior MMR vs imatinib; food/acid-reducer interaction |
| Dasatinib (Sprycel) | Second | Newly diagnosed CML-CP; resistant/intolerant CML (all phases) | Src kinase activity; effective in most imatinib resistance mutations; pleural effusion risk |
| Bosutinib (Bosulif) | Second | Newly diagnosed CML-CP; resistant/intolerant CML (CP, AP, BP) | GI-dominant side effects; food increases absorption (take with meal) |
| Ponatinib (Iclusig) | Third | Resistant/intolerant CML; T315I mutation | Covers T315I “gatekeeper” mutation; arterial thromboembolism risk |
Nilotinib is classified as a second-generation TKI. It was engineered from the imatinib structure to achieve higher binding affinity and selectivity for BCR-ABL1, addressing imatinib resistance mutations and producing faster, deeper molecular responses. It is described as the most selective inhibitor of BCR-ABL among the approved TKIs, with potency approximately 30 times higher than imatinib in vitro.
The ENESTnd Trial: The Clinical Evidence Foundation
Cavhanza’s FDA approval was supported by the established clinical evidence base for nilotinib, specifically the data from the ENESTnd (Evaluating Nilotinib Efficacy and Safety in Clinical Trials-Newly Diagnosed patients) trial (NCT00471497), the pivotal Phase 3 trial that defined nilotinib’s role in frontline CML.
ENESTnd enrolled 846 adult patients with newly diagnosed CML-CP within 6 months of diagnosis, stratified by Sokal risk score, and randomized them 1:1:1 to nilotinib 300 mg twice daily, nilotinib 400 mg twice daily, or imatinib 400 mg once daily.
| Endpoint | Nilotinib 300 mg twice daily | Imatinib 400 mg once daily | Significance |
|---|---|---|---|
| MMR (BCR-ABL1 at or below 0.1%) at 12 months | 44% | 22% | p less than 0.0001 |
| Complete cytogenetic response (CCyR) at 12 months | 80% | 65% | p less than 0.001 |
| Progression to accelerated or blast phase | 0.7% | 4.2% | Significantly reduced |
| 5-year MMR rate | 77% | 60% | Durable superior response |
| 10-year overall survival | Greater than 87% | Comparable (non-inferior) | Long-term survival similar |
Source: Saglio G et al. Nilotinib versus Imatinib for Newly Diagnosed CML. NEJM. 2010;362(24):2251–2259. doi:10.1056/NEJMoa0912614. 10-year analysis: Hochhaus A et al. Leukemia. 2022.. NCT00471497.
The landmark finding from ENESTnd was that nilotinib produced significantly higher rates of MMR at 12 months, significantly fewer progressions to accelerated or blast phase, and significantly more patients achieving deep molecular response (MR4, MR4.5) compared to imatinib across all Sokal risk categories. These advantages translated into a durable efficacy benefit through 10 years of follow-up, with 10-year MMR rates of approximately 77% for nilotinib 300 mg twice daily versus 60% for imatinib.
The 10-year analysis also confirmed a key safety signal: cardiovascular events including ischemic heart disease, peripheral artery disease, and stroke occurred at higher rates in nilotinib-treated patients (approximately 7 to 8%) than in imatinib-treated patients (approximately 2 to 3%) over a decade. This cardiovascular risk is now a well-established element of nilotinib’s prescribing profile and is included in boxed warning language.
Cavhanza’s approval was via the 505(b)(2) NDA pathway, which allows a new drug application to reference existing published literature and data from a reference-listed drug. The ODT studies showed no difference in the rate or extent of nilotinib absorption whether the ODT was swallowed whole or dissolved in the mouth before swallowing, confirming pharmaceutical equivalence of the two administration methods.
The Core Problem Cavhanza Solves: Acid Reducers and pH-Dependent Absorption
This is the clinical story that gives Cavhanza its differentiated value. Understanding it requires a brief look at what standard nilotinib capsules need to be absorbed effectively.
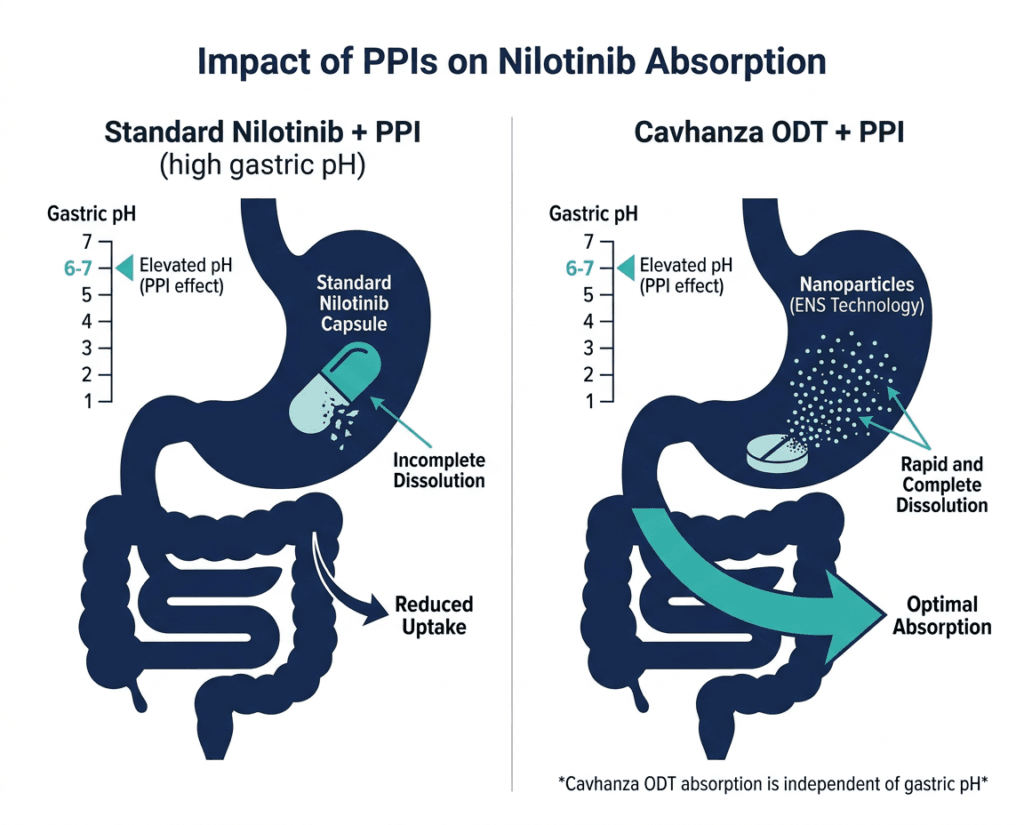
Nilotinib is a weakly basic molecule that dissolves best in acidic conditions. In the stomach’s normally acidic environment, the drug dissolves adequately before moving into the small intestine where it is absorbed. When proton pump inhibitors (PPIs) or histamine H2 receptor antagonists (H2RAs) are on board, they reduce gastric acid production, raising stomach pH substantially. In this elevated-pH environment, standard nilotinib capsules dissolve poorly, and absorption drops significantly.
The standard Tasigna prescribing information reflects this directly: PPIs should not be co-administered with nilotinib, and H2RAs must be separated by specific timing restrictions (H2RAs can be administered approximately 10 hours before or approximately 2 hours after nilotinib). For a patient taking a PPI for chronic GERD, that effectively means stopping the PPI. For a patient taking an H2RA, it means carefully coordinating two twice-daily medications around each other’s timing windows.
The scale of this problem: approximately 25% of Ph+ CML patients are co-prescribed acid-reducing agents. These are largely older adults managing both their leukemia and common age-related comorbidities including reflux, peptic ulcer disease, and gastroprotective use alongside other medications like aspirin or anticoagulants. Telling these patients to stop their acid reducer, or to comply with precise timing restrictions every day for years, is not a trivial ask. Non-adherence to TKI therapy in CML is directly associated with loss of molecular response.
The food effect compounds this further. Standard nilotinib capsules must be taken without food: eating within 2 hours before or 1 hour after a nilotinib dose significantly increases drug absorption and can raise plasma levels to potentially toxic ranges. This means four distinct daily time windows around which the patient must plan: fast before dose 1, fast after dose 1, fast before dose 2, fast after dose 2. For patients managing a full daily life including meals and medications, this is a substantial behavioral burden.
How Cavhanza addresses both problems
Cavhanza uses Flex Pharma’s proprietary ElectroNanoSpray (ENS) technology to produce a nanoparticle-scale formulation of nilotinib with dramatically improved solubility and dissolution characteristics. By engineering the drug particles to be far smaller, the formulation increases the surface area available for dissolution and reduces the drug’s dependence on low gastric pH to dissolve adequately before reaching the small intestine. The result:
- PPI co-administration: allowed with Cavhanza — no contraindication, no timing restriction
- H2RA co-administration: allowed with Cavhanza — no timing restriction
- Food effect: eliminated — Cavhanza can be taken with or without food
The orally disintegrating tablet format adds a further convenience dimension: the tablet can dissolve in the mouth before swallowing or can be swallowed whole. It can be taken with or without water. For patients who have difficulty swallowing capsules, or for patients in clinical settings where oral medication access is limited, these properties matter.
Safety: What Prescribers and Patients Need to Know
Cavhanza carries the same safety profile as nilotinib across all formulations, because the active molecule is identical. The safety program that governs Tasigna governs Cavhanza.
Boxed warnings:
QT prolongation and sudden death: Nilotinib prolongs the QT interval and has been associated with sudden death. Hypokalemia or hypomagnesemia must be corrected before initiating nilotinib and monitored during therapy. Avoid drugs that prolong the QT interval, including many anti-arrhythmic medications, certain antifungals, and fluoroquinolone antibiotics. An ECG is required at baseline, 7 days after initiation, and periodically thereafter. Do not use in patients with hypokalemia, hypomagnesemia, or long QT syndrome.
Hepatotoxicity: Nilotinib may cause severe hepatotoxicity and liver failure, including fatal cases. Monitor liver function tests before initiating and monthly during the first year, then periodically.
Cardiovascular events: Nilotinib is associated with an increased incidence of ischemic heart disease, peripheral artery disease, and ischemic cerebrovascular events. The 10-year ENESTnd data showed cardiovascular event rates of approximately 7 to 8% over a decade. Patients with cardiovascular risk factors should be assessed carefully before initiating nilotinib, with optimization of modifiable risk factors. Monitor for signs of cardiovascular disease during treatment.
Key warnings and precautions:
| Safety item | Details | Clinical guidance |
|---|---|---|
| QT prolongation (boxed warning) | Prolongs QTcF; sudden death reported | ECG at baseline, day 7, and periodically. Correct electrolytes. Avoid QT-prolonging drugs. Hold and restart at reduced dose if QTcF greater than 480 ms. |
| Hepatotoxicity (boxed warning) | Severe liver injury and fatal liver failure reported | LFTs at baseline, monthly for first year, periodically thereafter. |
| Cardiovascular events | Ischemic heart disease, PAD, and stroke at higher rates than imatinib in long-term follow-up | Assess and manage CV risk factors before initiating. Monitor for signs of CV disease. |
| Myelosuppression | Neutropenia, thrombocytopenia, and anemia; dose modification or interruption may be required | CBC at baseline, every 2 weeks for first 2 months, then monthly. |
| Pancreatitis | Lipase and amylase elevations; symptomatic pancreatitis reported | Monitor lipase and amylase monthly or as clinically indicated. |
| Hepatitis B reactivation | Reactivation in chronic HBV carriers including fulminant hepatitis and fatal outcomes | Screen for HBV before initiating. Monitor carriers closely; consider antiviral prophylaxis. |
| CYP3A4 interactions | Strong CYP3A4 inhibitors increase nilotinib exposure; strong inducers reduce it | Avoid strong CYP3A4 inhibitors (ketoconazole, ritonavir, clarithromycin); avoid strong inducers (rifampin). If unavoidable, dose reduction recommended. |
| Embryo-fetal toxicity | Nilotinib can cause fetal harm | Women of reproductive potential: effective contraception during treatment. Advise of reproductive risks before starting therapy. |
| Lactation | Not recommended during treatment and for 14 days after last dose | Discuss with patients before initiating. |
| Pediatric use | Cavhanza not approved for pediatric patients | The approved indication is adults only. |
Common adverse reactions (occurring in 10% or more of patients in clinical trials): rash, nausea, headache, fatigue, pruritus, vomiting, alopecia, myalgia, and constipation.
What This Means for CML Patients and Prescribers
The practical change
For an established CML patient currently on Tasigna (nilotinib capsules) who also takes a PPI or H2RA: Cavhanza is now a clinically appropriate alternative that eliminates the drug interaction concern without changing the active compound, the dose, or the established molecular monitoring expectations. The transition from Tasigna to Cavhanza is a formulary and tolerability decision, not a clinical efficacy change.
For newly diagnosed CML-CP patients who also have GERD, peptic ulcer disease, or any clinical need for an acid reducer: the nilotinib-PPI interaction no longer needs to govern the treatment decision. Cavhanza can be initiated at the standard 300 mg twice-daily dose without worrying about acid-reducer timing or co-prescription contraindications.
For CML-CP and CML-AP patients with resistance or intolerance to prior therapy including imatinib: Cavhanza at 400 mg twice daily is now an option with the same added prescribing flexibility.
For oncology pharmacists and hematologists reviewing CML patients on complex polypharmacy regimens: Cavhanza’s elimination of the food restriction and the acid-reducer interaction removes two of the most practically difficult elements of long-term nilotinib adherence. Non-adherence to TKI therapy is directly associated with loss of molecular response and the risk of disease progression in CML. Any formulation innovation that reduces adherence barriers has the potential to translate into better molecular outcomes for this patient population.
Dr. Kevan Herold’s statement about treating a different disease earlier applies here in spirit: much of the value of precision oncology in CML comes from the consistency and completeness of BCR-ABL suppression. Inconsistent drug levels from missed doses, from food effect violations, or from acid-reducer-mediated reduced absorption, erode that suppression and create the selective pressure that drives resistance mutations.
The monitoring requirements remain
Regardless of formulation, patients on nilotinib require: baseline and periodic ECGs; CBC monitoring every 2 weeks for the first 2 months and monthly thereafter; LFTs monthly for the first year; electrolyte monitoring; and BCR-ABL1 PCR monitoring every 3 months during the first year and every 3 to 6 months thereafter. These monitoring requirements are unchanged by the ODT formulation.
For related HED coverage on CML and hematologic oncology, see our post on Pomalyst (pomalidomide) losing exclusivity and what generic pomalidomide means for multiple myeloma patients from the 2026 Loss of Exclusivity series.
Sources
Cycle Pharmaceuticals press release (approval): CAVHANZA (nilotinib) Orally Disintegrating Tablets: A New, FDA-approved Treatment Offering PPI and H2RA Flexibility for Ph+ CML Patients. BusinessWire. June 2, 2026.
BioSpace coverage: CAVHANZA (nilotinib) Orally Disintegrating Tablets: A New, FDA-approved Treatment. biospace.com. June 2026.
Targeted Oncology clinical summary: FDA OKs Oral Nilotinib Tablets for Ph+ CML With Acid-Reducer Flexibility. targetedonc.com. June 2026.
Cancer Therapy Advisor: FDA Approves Cavhanza, an ODT Formulation of Nilotinib for Ph+ CML. cancertherapyadvisor.com. June 2026.
Oncology Nursing News: FDA Approves Oral Nilotinib Tablets for Ph+ CML. oncnursingnews.com. June 2026.
WebMD approval summary: Cavhanza (Nilotinib) FDA Approval. webmd.com. June 2026.
ENESTnd primary publication: Saglio G et al. Nilotinib versus Imatinib for Newly Diagnosed CML in Chronic Phase. NEJM. 2010;362(24):2251–2259. doi:10.1056/NEJMoa0912614.
ENESTnd 10-year analysis: Hochhaus A et al. Long-term outcomes with frontline nilotinib versus imatinib in newly diagnosed CML-CP: ENESTnd 10-year analysis. Leukemia. 2022.
ENESTnd trial registration: NCT00471497. ClinicalTrials.gov.
BCR-ABL mutations and nilotinib selectivity: Nilotinib and BCR-ABL mutations. PMC4915803.
Philadelphia chromosome and CML mechanism: Chronic Myelogenous Leukemia. StatPearls. NCBI.
Philadelphia chromosome molecular biology: BCR-ABL1 in CML. PMC7955155.
PPIs overview: Proton Pump Inhibitors. StatPearls. NCBI.
H2RAs overview: Histamine H2 Receptor Antagonists. StatPearls. NCBI.
QT prolongation: QT Prolongation. StatPearls. NCBI.
505(b)(2) NDA pathway: 505(b)(2) Applications. FDA.gov.
FDA nilotinib original approval: FDA approves nilotinib for chronic myeloid leukemia. FDA.gov.
Cavhanza prescribing information: CAVHANZA (nilotinib) Prescribing Information. Flex Pharma/Cycle Pharmaceuticals. 2026.
American Cancer Society CML overview: Chronic Myeloid Leukemia. cancer.org.
Patient resources: Leukemia and Lymphoma Society (LLS) | CML Advocates Network | Cycle Pharmaceuticals Cavhanza support | [Breakthrough T1D is not applicable here] | Novartis Tasigna patient support
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice. Nilotinib (Cavhanza) carries boxed warnings for QT prolongation with sudden death risk, hepatotoxicity, and cardiovascular events. CML management requires individualized care by a board-certified hematologist or oncologist with expertise in TKI therapy. Patients considering a transition from Tasigna to Cavhanza should discuss this with their treating hematologist-oncologist. |
|---|
Leave a Reply