I have all the data including the nuanced primary endpoint story. This is one of the more interesting approval stories of 2026 because the full ITT analysis technically missed the noninferiority margin but the FDA approved based on the modified ITT. That distinction must be presented honestly and clearly. Here is the full compliant post.
The First Needle-Free Mealtime Insulin Option for Children Just Got FDA Approval. Here Is What the INHALE-1 Data Shows, Including the Part That Is More Complicated Than the Headlines Suggest.
By M. Rodriguez, CST/CMA/CCA | Health Evidence Digest
| 📌 The essentials On May 29, 2026, the FDA approved Afrezza (insulin human inhalation powder, MannKind Corporation) for use in children and adolescents aged 6 years and older with type 1 or type 2 diabetes. This expands Afrezza’s label beyond adults (approved June 2014) to include pediatric patients for the first time. Afrezza is the first and only inhaled mealtime insulin available to pediatric patients in the more than 100-year history of insulin therapy. The clinical basis: Phase 3 INHALE-1 trial (NCT04974528), 230 children and adolescents aged 4 to 17 years, 26-week randomized open-label comparison of Afrezza plus basal insulin versus multiple daily injections (MDI) of rapid-acting insulin analog plus basal insulin. Published in Diabetes Care, January 2026. Important nuance on the primary endpoint: the full intent-to-treat (ITT) analysis showed a between-group HbA1c difference of 0.435%, narrowly exceeding the prespecified noninferiority margin of 0.4%. This was attributed to a single non-adherent patient. A pre-specified modified ITT (mITT) analysis excluding this patient showed a difference of 0.370%, meeting noninferiority. The FDA approved based on the totality of evidence including the mITT analysis, long-term safety data, lung function data, and 20-plus years of Technosphere inhaled insulin research. Pulmonary safety: no significant difference in lung function between groups at 26 weeks. FEV1 remained within normal range throughout. No serious pulmonary adverse events. Secondary findings: significantly less weight gain and significantly higher treatment satisfaction in Afrezza-treated patients and parents versus MDI. Age minimum: 6 years and older. Price: eligible patients can access Afrezza for $35 or less per month through MannKind Cares. |
|---|
Insulin has been injected for more than 100 years. Every child diagnosed with type 1 diabetes has faced the same reality: multiple daily needle sticks, in school, at meals, at sports practice, at birthday parties, at sleepovers. For most of that century, there was no alternative.
On May 29, 2026, the FDA approved Afrezza (insulin human inhalation powder) for use in children and adolescents aged 6 and older, making it the first needle-free mealtime insulin option ever available to pediatric patients. The drug that has been available to adult patients with diabetes since 2014 can now be prescribed to the children and adolescents for whom injection anxiety, school logistics, and social friction around insulin administration are documented barriers to adherence and glycemic control.
The clinical evidence behind the approval requires honest presentation. The pivotal trial technically missed its pre-specified primary endpoint in the full analysis, approved based on a modified analysis and a totality of supporting evidence. That is a fact families and prescribers deserve to understand, not a reason to dismiss a drug that addresses one of the most durable unmet needs in pediatric diabetes care.
Why Needle Anxiety in Children With Diabetes Is a Clinical Problem, Not a Parental Preference
Needle anxiety in children with diabetes is one of the most consistently documented barriers to optimal insulin therapy in pediatric endocrinology. It is not simply a matter of children disliking injections; it is a behavioral pattern with measurable downstream consequences for glycemic control.
Fear of injections drives dose skipping, delayed mealtime insulin administration, avoidance of insulin correction doses when blood glucose runs high, and in some cases refusal to initiate or intensify insulin therapy at diagnosis. In school settings specifically, the logistics of supervised insulin administration, the social visibility of the act, and the fear of peer reactions around needles create practical barriers that affect real-world glycemic management differently from how they appear in clinical trials conducted in controlled settings.
The consequences of suboptimal mealtime insulin dosing in children compound over time. Chronic hyperglycemia accelerates the development of diabetic retinopathy, nephropathy, and neuropathy. In children who spend years with elevated post-meal glucose excursions because they skip or reduce mealtime insulin doses to avoid injections, the long-term risk burden is real and well-established.
This is the clinical backdrop against which the Afrezza pediatric approval should be understood. Whether inhaled insulin achieves slightly different HbA1c values than injections in a controlled trial is relevant; whether it enables children who currently under-dose or skip mealtime insulin to take it more consistently is equally relevant, and arguably more important for the majority of real-world pediatric patients.
What Afrezza Is and How the Technosphere Delivery System Works
Afrezza is an inhaled formulation of recombinant human insulin that uses MannKind’s proprietary Technosphere drug delivery platform to achieve rapid pulmonary absorption. The drug is provided as a dry powder in a foil blister cartridge and is inhaled through a small, pocket-sized inhaler at the start of each meal.
The Technosphere platform consists of fumaryl diketopiperazine (FDKP) particles, which are engineered to form microparticles that carry insulin into the deep lung. When these particles reach the alveolar surface, they dissolve rapidly in the aqueous lung lining, releasing insulin that is then absorbed into the pulmonary capillary bloodstream. This pulmonary absorption pathway bypasses the subcutaneous tissue depot that slows absorption with injected insulin.
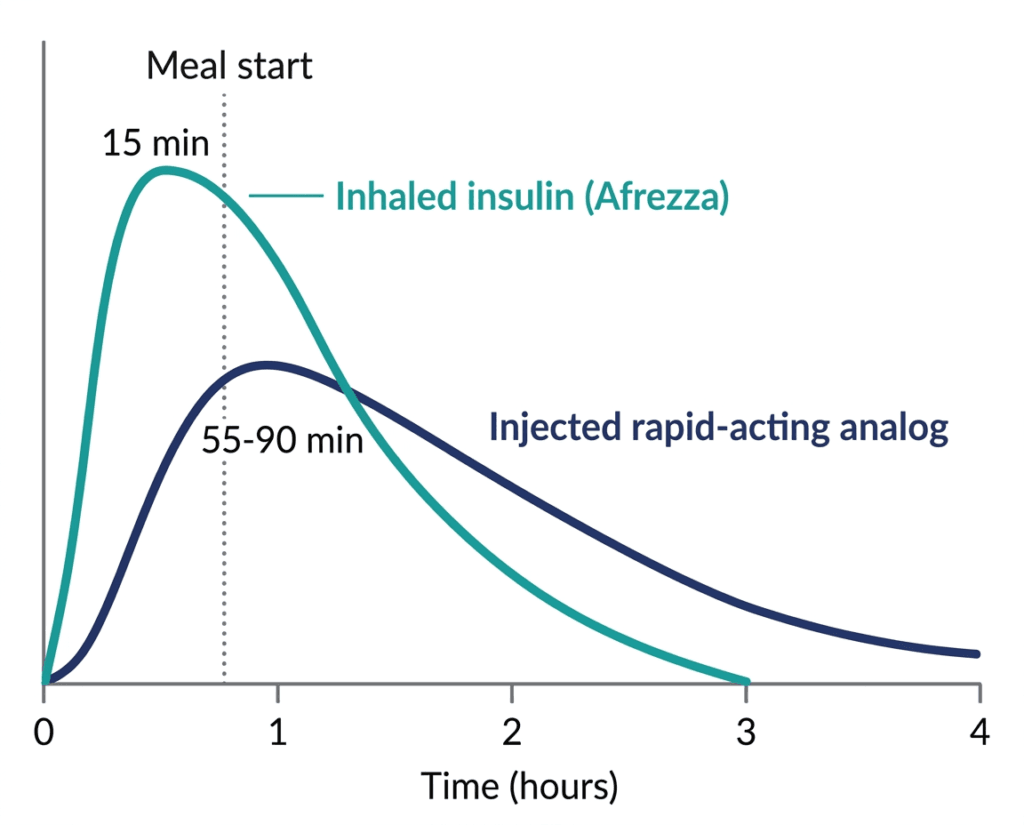
The pharmacokinetic result is what makes Afrezza clinically distinctive: it is the fastest-acting insulin available. In adults, Afrezza reaches peak insulin concentration within approximately 12 to 15 minutes of inhalation, compared to 55 to 90 minutes for rapid-acting injectable analogs like aspart, lispro, or glulisine. The duration of action is correspondingly shorter, approximately 3 hours, compared to 3 to 5 hours for injectable rapid-acting analogs.
| Why ultra-rapid onset matters for post-meal glucose control Mealtime insulin is meant to blunt the glucose spike that follows carbohydrate absorption. For injected rapid-acting insulin analogs, there is a well-documented mismatch: the insulin starts working 15 to 30 minutes after injection but glucose starts rising almost immediately upon eating. Patients are instructed to inject 15 to 20 minutes before eating, but adherence to pre-meal injection timing is low in practice, particularly in children and adolescents in real-world settings. Afrezza’s rapid onset means it can be inhaled at the start of the meal rather than before and still reach peak effect while glucose is rising from that meal. This timing advantage is pharmacologically meaningful and practically significant in school-age children who cannot predict meal timing, must eat quickly, or cannot leave class early to administer insulin before lunch. |
|---|
The INHALE-1 Trial: What the Data Shows, Including the Nuance
Design
INHALE-1 (NCT04974528) was a 26-week, open-label, randomized, multicenter Phase 3 clinical trial with a 26-week safety extension, enrolling children and adolescents aged 4 to 17 years with type 1 or type 2 diabetes. The open-label design was necessary because blinding inhaled versus injected insulin in children is not practically feasible.
Enrollment (n=230): Randomized 1:1 to:
- Afrezza inhalation powder plus basal insulin (n approximately 115)
- Multiple daily injections (MDI) of rapid-acting insulin analog plus basal insulin (n approximately 115)
Primary endpoint: Non-inferiority in change in HbA1c from baseline at 26 weeks, with a prespecified non-inferiority margin of 0.4%.
Lung safety monitoring: FEV1 (forced expiratory volume in 1 second) and FVC measured at baseline, 12 weeks, and 26 weeks. Serious pulmonary adverse events tracked throughout.
Key secondary endpoints: Weight change, treatment satisfaction (patients and parents), time in range (blood glucose 70 to 180 mg/dL), hypoglycemia frequency.
The primary endpoint: what happened and why it matters
This is the most clinically important and least straightforwardly reported aspect of the INHALE-1 data, and it deserves transparent presentation.
| HbA1c analysis | Between-group difference (Afrezza minus MDI) | vs. 0.4% margin |
|---|---|---|
| Full intent-to-treat (ITT) analysis (n=230) | +0.435% | Exceeds margin — non-inferiority NOT met |
| Modified ITT (mITT) analysis (n=229, excluding 1 non-adherent patient) | +0.370% | Below margin — non-inferiority met |
Source: INHALE-1, NCT04974528. Published Diabetes Care. January 2026. Cardiology Advisor pre-approval coverage. April 2026.
In the full ITT population, the mean HbA1c change was marginally worse in the Afrezza arm, with a between-group difference of 0.435%. This narrowly exceeded the prespecified non-inferiority margin of 0.4%, meaning the full analysis technically did not meet the primary endpoint as specified.
According to MannKind and the investigating team, this outcome was driven by a single patient who did not adhere to the study protocol. Excluding this patient in the pre-specified mITT analysis produced a between-group difference of 0.370%, which falls within the 0.4% margin, meeting non-inferiority.
The FDA approved Afrezza for pediatric use based on the totality of evidence, including the mITT analysis, 26-plus weeks of lung function data showing no meaningful pulmonary effects, 52-week safety extension data, and more than 20 years of Technosphere inhaled insulin research across thousands of patients including prior adult programs.
It is worth being direct about what this means: the FDA reviewed the evidence and concluded the benefit-risk profile supports approval. The influence of a single non-adherent patient on the ITT analysis, the pre-specified nature of the mITT sensitivity analysis, and the favorable safety, satisfaction, and weight data collectively informed that conclusion. Patients and prescribers should be aware of this nuance; it does not invalidate the approval but it is relevant context for how to weigh the glycemic control evidence.
Lung function: the key safety endpoint
| Lung function parameter | Afrezza arm | MDI arm |
|---|---|---|
| Mean FEV1 at baseline | 2.901 L (99.6% predicted) | 2.948 L (102.3% predicted) |
| Mean FEV1 at week 26 | 2.934 L (96.6% predicted) | 2.957 L (98.0% predicted) |
| Between-group difference in FEV1 change | Not statistically significant | Reference |
| Serious pulmonary adverse events | None reported | None reported |
| Normal FEV1 range maintained throughout | Yes, both groups | Yes |
The lung function data is the most reassuring finding from INHALE-1 for families with legitimate concerns about what happens to a child’s lungs when they inhale insulin particles for months or years. In INHALE-1, both groups showed small declines in FEV1 percentage of predicted at 26 weeks, with no statistically significant difference between groups and both remaining solidly within normal range throughout.
No serious pulmonary complications were reported in either group over 26 weeks or through the 52-week safety extension.
Secondary endpoints: weight and satisfaction
| Secondary endpoint | Finding |
|---|---|
| Weight gain at 26 weeks | Significantly less with Afrezza than MDI |
| Treatment satisfaction (patient-reported) | Significantly higher with Afrezza |
| Parent treatment satisfaction | Significantly higher for parents of Afrezza-treated patients |
| Hypoglycemia frequency at 26 weeks | No significant difference between groups |
The weight finding is clinically meaningful. Weight gain is a documented side effect of intensified insulin therapy in children and adolescents, and excess weight gain in a pediatric diabetes population has both metabolic and psychological implications. Less weight gain with equivalent glycemic control is a genuine secondary benefit.
The treatment satisfaction finding matters for exactly the reason discussed above: a mealtime insulin option that children and parents prefer is more likely to be used consistently, particularly for the dose corrections and meal-related doses that are most commonly skipped.
The Lung Cancer Warning: What It Means and Does Not Mean for Children
Adults using Afrezza carry a warning about a potential lung cancer signal observed in adult clinical trials. This is a labeled warning that appears in the prescribing information and requires honest discussion.
The signal emerged from long-term adult trials and post-market pharmacovigilance in adults with significant histories of smoking. A causal relationship between inhaled insulin use and lung cancer has not been established. The FDA’s assessment for the adult label concluded the benefit-risk profile remained favorable for indicated adult patients while warranting the warning and ongoing monitoring.
For pediatric patients, several important contextual points apply:
- The lung cancer signal, to the extent it exists, was observed in adults with long smoking histories
- INHALE-1 enrolled children specifically excluding prior clinically significant pulmonary disease and requiring baseline normal lung function
- No oncologic safety signals were observed in INHALE-1 or its extension
- Afrezza is labeled for pediatric use starting at age 6, and the FDA reviewed pediatric-specific lung function data before granting the approval
The warning is present in the pediatric label. Parents and prescribers should be aware of it, discuss it in the context of the full benefit-risk picture for an individual child, and continue routine follow-up monitoring of pulmonary function as clinically indicated.
Safety: The Full Prescribing Information Picture
Boxed warning (applies to adult label; relevant context for pediatric prescribers):
- Acute bronchospasm in patients with chronic lung disease (asthma, COPD)
- Contraindicated in patients with chronic lung disease
- Lung cancer signal in adults (see above)
Contraindications:
- Patients with chronic lung disease including asthma and COPD (increased risk of acute bronchospasm)
- During episodes of hypoglycemia
- Hypersensitivity to any component of the formulation
Warnings and precautions:
- Acute bronchospasm: patients should have a short-acting bronchodilator available; spirometry is recommended before initiating treatment in patients with mild or moderate lung disease
- Hypoglycemia: as with all insulins, the risk of hypoglycemia requires monitoring
- Hypokalemia: insulin drives potassium into cells; monitor in patients at risk
- Fluid retention and heart failure (applies to combination with thiazolidinediones, not standard pediatric use)
Lung function monitoring: Perform FEV1 assessment before initiating Afrezza, every 6 months during treatment, and as clinically indicated.
Who Should and Should Not Use Afrezza
Appropriate candidates for Afrezza in the pediatric setting
- Children and adolescents aged 6 and older with type 1 or type 2 diabetes who require mealtime insulin
- Patients with significant needle anxiety affecting mealtime insulin adherence
- Patients who frequently skip or reduce mealtime doses due to injection reluctance
- Patients and families who prefer the flexibility and convenience of inhaled administration for school, social, and athletic contexts
- Patients with normal baseline lung function per spirometry
Contraindicated or not appropriate
- Any patient with asthma, COPD, or other chronic pulmonary disease (absolute contraindication)
- Patients with FEV1 below 70% predicted (exclude from eligibility per trial criteria)
- Patients with recent respiratory tract infections (hold until resolved)
- Patients under 6 years of age
- Afrezza is not a replacement for basal insulin and cannot be used as a basal insulin; it is a mealtime (prandial) insulin only
Practical note for younger patients (ages 6 to 7)
Afrezza administration requires the ability to use the inhaler device correctly and to exhale fully before inhalation. Children aged 6 to 7 may require more practice and caregiver supervision to ensure consistent technique. Pediatric endocrinologists and diabetes educators should assess inhaler technique specifically in younger patients before transitioning to Afrezza independently.
Dosing
Afrezza doses are based on the patient’s usual rapid-acting insulin analog dose, converted according to the prescribing information dose conversion table. The drug is available in single-use cartridges of 4 units, 8 units, and 12 units of inhaled insulin. Key dose conversion guidance (from the January 2026 label update providing starting dose guidance for patients switching from insulin pumps or MDI) is available in the full prescribing information.
Timing: inhale at the beginning of each meal. Do not use during or after a meal. Do not use for correction doses if the patient is already hypoglycemic.
Access and Cost
MannKind has announced that eligible patients can access Afrezza for $35 or less per month through its MannKind Cares patient support program. For a condition requiring daily medication for life, this cost point is a meaningful access consideration and compares favorably with list pricing for injectable rapid-acting insulin analogs prior to the insulin price cap legislation and assistance programs currently in effect.
For related HED coverage on insulin access and recent approvals, see our post on Awiqli, the first once-weekly basal insulin for type 2 diabetes, our post on Langlara and what interchangeable insulin biosimilars mean for affordability, and our post on Linzess expanding to children as young as 2 as another pediatric label expansion approval from the same week.
Sources
FDA approval announcement and MannKind press release: MannKind Announces FDA Approval of Afrezza, the First and Only Inhaled Mealtime Insulin for Use in Children and Adolescents Aged 6 and Older Living with Diabetes. GlobeNewswire. May 29, 2026.
Drugs.com approval news: MannKind Announces FDA Approval of Afrezza for Children and Adolescents Aged 6 and Older. drugs.com. May 29, 2026.
AJMC clinical summary: FDA Approves Inhaled Insulin for Children, Adolescents With Diabetes. ajmc.com. May 2026.
Pharmacy Times approval coverage: FDA Approves Afrezza Insulin Inhalation Powder for Children, Adolescents With Type 1 and Type 2 Diabetes. pharmacytimes.com. May 2026.
HCPLive approval coverage: FDA Approves Inhaled Insulin Afrezza for Pediatric Patients With Diabetes. hcplive.com. May 2026.
Patient Care Online: FDA Approves First Inhaled Mealtime Insulin for Children and Adolescents With Diabetes. patientcareonline.com. May 2026.
TechTimes decision day coverage (with primary endpoint nuance): Inhaled Insulin for Children: FDA Reaches Decision Deadline for Afrezza. techtimes.com. May 29, 2026.
INHALE-1 primary publication: INHALE-1 Phase 3 results. Diabetes Care. January 2026.
INHALE-1 ADA 2025 presentation: Phase 3 INHALE-1 results presented at 85th ADA Scientific Sessions. Chicago, June 2025.
INHALE-1 trial registration: NCT04974528. ClinicalTrials.gov.
sBLA acceptance (October 2025): MannKind Announces US FDA Accepts for Review its Supplemental Biologics License Application (sBLA) for Inhaled Insulin (Afrezza) in Children and Adolescents Aged 4-17 Years. GlobeNewswire. October 13, 2025.
Cardiology Advisor pre-approval detailed data summary: FDA Drug Approval Decisions Expected in May 2026. thecardiologyadvisor.com. April 2026.
Afrezza original adult FDA approval (June 2014): FDA approves Afrezza to treat diabetes. FDA.gov. June 2014.
Afrezza prescribing information: Afrezza (insulin human) Inhalation Powder Prescribing Information. MannKind. 2026.
Needle anxiety and pediatric diabetes: Fear of Needles and Its Impact on Diabetes Management. PMC8261965.
Diabetic complications prevention: Preventing Diabetes Problems. NIDDK.
Patient resources: JDRF (type 1 diabetes) | American Diabetes Association: Mealtime Insulin | MannKind Cares patient support | Afrezza patient website
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Afrezza is contraindicated in patients with chronic lung disease including asthma and COPD. All decisions about mealtime insulin therapy for children and adolescents with diabetes should be made in close consultation with a pediatric endocrinologist or diabetes care team familiar with the child’s complete health history, current diabetes management, and pulmonary function status. |
|---|
Leave a Reply