| 📌 The essentials On May 15, 2026, the FDA approved venetoclax tablets (Dr. Reddy’s Laboratories) in three strengths, 10 mg, 50 mg, and 100 mg, as the first generic version of Venclexta (venetoclax, AbbVie/Genentech). Venclexta has been on the market since April 2016 and at its brand list price costs thousands of dollars per month, making it inaccessible or unaffordable for many patients who need it. The generic is therapeutically equivalent to the brand-name product: the same molecule, the same doses, the same clinical indications. What venetoclax is approved for: adults with chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL), including as part of multiple combination regimens, and adults with newly diagnosed AML who are 75 years or older or have comorbidities precluding intensive chemotherapy, in combination with azacitidine, decitabine, or low-dose cytarabine. Recent additional approval: in February 2026, the FDA also approved venetoclax plus acalabrutinib as the first all-oral, fixed-duration combination for previously untreated CLL. What the generic approval means in practice: competition between generic and brand-name manufacturers typically drives price reduction over time. How quickly and how substantially prices fall depends on how many generic manufacturers enter the market and on formulary and pharmacy benefit manager decisions. For patients currently on Venclexta: your pharmacist may substitute the generic at the counter; check with your oncologist and pharmacist about what to expect at your next fill. For patients considering venetoclax therapy: the generic approval is the beginning of an access improvement story; real-world pricing at pharmacies will emerge over the coming weeks and months. |
|---|
Few drugs in the history of blood cancer treatment have had as broad and rapid an impact as venetoclax. When the FDA first approved it in April 2016, it validated a decade of research into BCL-2 (B-cell lymphoma-2) as a cancer survival target and introduced a mechanism of action, apoptosis restoration, that was entirely distinct from chemotherapy or the kinase inhibitors that preceded it in the same patient populations.
In the nearly decade since, venetoclax has accumulated FDA approvals across multiple blood cancer indications, generated pivotal trial data with some of the most compelling remission rates ever seen in chronic lymphocytic leukemia and AML, and become a cornerstone of treatment regimens ranging from CLL to multiple myeloma to myelodysplastic syndromes. It is taken by hundreds of thousands of patients. And until May 15, 2026, every one of them required a brand-name drug at brand-name pricing.
On May 15, 2026, Dr. Reddy’s Laboratories received the first FDA generic approval for venetoclax, ending the brand exclusivity that AbbVie and Genentech have held since 2016. For a drug with a monthly list price that has historically exceeded $10,000, the arrival of generic competition is a meaningful moment for patients and payers.
This post covers what venetoclax is, the science behind why it works, its complete approved indication landscape, the safety profile clinicians and patients need to understand, and what the generic approval means practically.
What BCL-2 Is and Why Blocking It Kills Cancer Cells
Understanding venetoclax requires understanding a fundamental principle of cancer biology: cancer cells have learned to cheat death.
Normal cells have a built-in self-destruction mechanism called apoptosis, programmed cell death. When a cell is damaged, mutated, or simply no longer needed, internal signaling pathways trigger a cascade that dismantles the cell from within. This mechanism is one of the body’s primary defenses against cancer: cells that accumulate oncogenic mutations are normally eliminated by apoptosis before they can proliferate into a tumor.
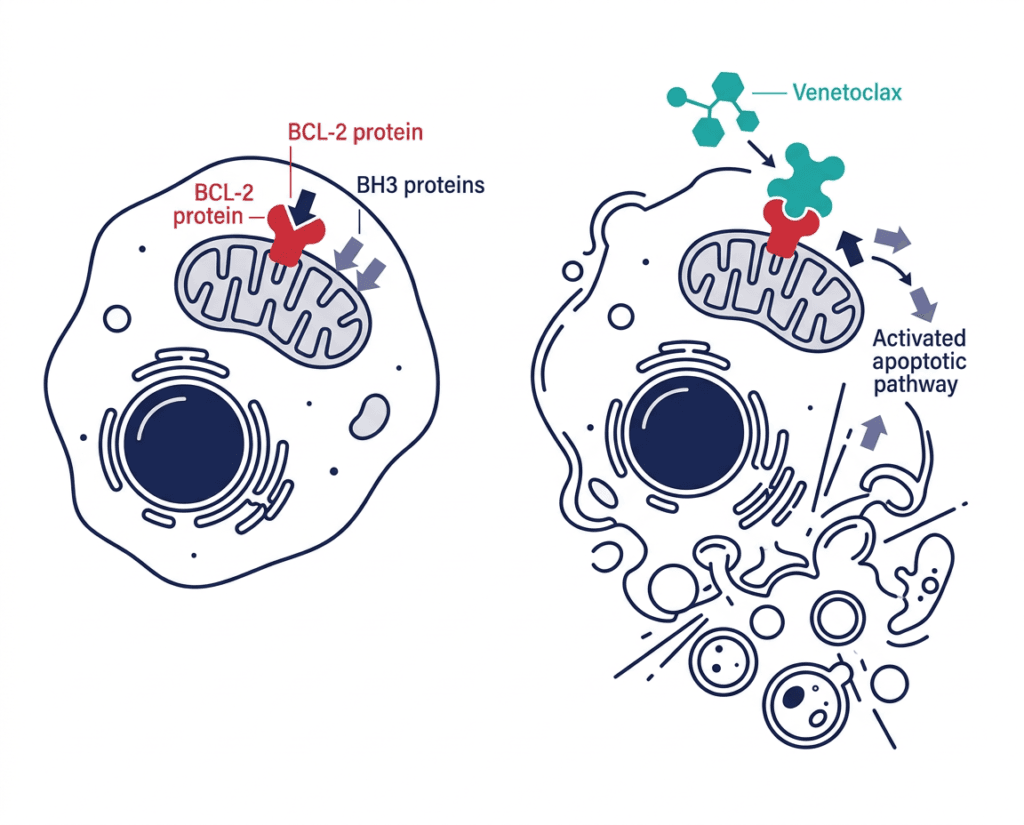
Many cancer cells, particularly blood cancers including CLL, SLL, AML, and multiple myeloma, escape this mechanism by overexpressing BCL-2, a protein that resides on the outer membrane of mitochondria and functions as a survival signal. BCL-2 works by binding and sequestering BH3-only proteins, the molecules that would normally activate the apoptotic cascade. By flooding the cell with BCL-2, cancer cells effectively disable their own self-destruct mechanism, allowing them to accumulate, resist chemotherapy, and evade the immune system.
Venetoclax is an oral, highly selective BCL-2 inhibitor. It was discovered through a collaboration between AbbVie and Genentech using fragment-based drug design, specifically engineered to mimic the BH3 domain of pro-apoptotic proteins. By binding to BCL-2 with extremely high affinity, venetoclax displaces the sequestered BH3-only proteins, freeing them to activate the mitochondrial apoptotic pathway. The result is rapid apoptotic cell death, within hours of exposure in susceptible cells, in cancer cells that have been surviving by BCL-2-mediated cheating.
| Why BCL-2 inhibition produces tumor lysis syndrome (TLS): the critical safety concept Venetoclax works so effectively, and so rapidly, in BCL-2-dependent cancer cells that its primary serious risk is a direct consequence of its efficacy. When large numbers of cancer cells die rapidly, they release their intracellular contents, including potassium, phosphate, uric acid, and other electrolytes, into the bloodstream simultaneously. This electrolyte release is called tumor lysis syndrome (TLS). Severe TLS can cause dangerous elevations in potassium (leading to fatal cardiac arrhythmias), elevated phosphate (causing calcium to drop, risking seizures and cardiac dysfunction), elevated uric acid (causing kidney damage), and acute kidney failure. This is why venetoclax requires a careful ramp-up dosing schedule rather than starting at the full therapeutic dose. The ramp-up, beginning at 20 mg daily and escalating weekly over 5 weeks to 400 mg in CLL, is specifically designed to kill cancer cells gradually enough to allow the kidneys and other organs to clear the cellular debris without being overwhelmed. Pre-treatment assessment of TLS risk is mandatory. Patients at high risk (large lymph nodes, high lymphocyte counts) require hospitalization and intravenous hydration for at least the first dose of each ramp-up step. Understanding TLS is the single most important safety concept for any clinician initiating venetoclax therapy. |
|---|
Venetoclax’s Complete FDA-Approved Indication Landscape
Over nearly a decade, venetoclax has accumulated multiple approved indications, alone and in combination, making its approved use landscape one of the most complex of any hematologic oncology drug currently available. As of May 2026, the approved indications are:
CLL and SLL indications
Indication 1: CLL or SLL monotherapy Originally approved April 2016 for adult patients with CLL or SLL with 17p deletion who had received at least one prior therapy. Expanded in 2018 to all adult patients with CLL or SLL who had received at least one prior therapy, regardless of 17p deletion status.
Indication 2: CLL/SLL with obinutuzumab (first-line) Venetoclax plus obinutuzumab (Gazyva) for previously untreated adults with CLL or SLL, approved May 2019. Based on the CLL14 trial showing superior PFS with the combination versus chlorambucil plus obinutuzumab (HR 0.31; p less than 0.0001).
Indication 3: CLL/SLL with rituximab (relapsed or refractory) Venetoclax plus rituximab for adults with CLL or SLL who have received at least one prior therapy, approved June 2018. Based on the MURANO trial.
Indication 4: CLL/SLL with acalabrutinib (first-line) — February 2026 Venetoclax plus acalabrutinib (Calquence) for previously untreated adult patients with CLL without 17p deletion or TP53 mutation, approved February 20, 2026. The first all-oral, fixed-duration combination regimen for first-line CLL. Based on the Phase 3 AMPLIFY trial showing 3-year PFS of 76.5% with the doublet versus 66.5% with chemoimmunotherapy (HR 0.65; p=0.004). Treatment duration is fixed at 14 cycles, offering the potential for time off treatment.
AML indications
Indication 5: AML combination therapy (older or comorbid adults) Venetoclax in combination with azacitidine, decitabine, or low-dose cytarabine for newly diagnosed AML in adults aged 75 or older or with comorbidities precluding intensive induction chemotherapy, initially approved November 2018 under accelerated approval and confirmed with full approval based on the VIALE-A trial (azacitidine combination, OS 14.7 months versus 9.6 months with placebo; HR 0.66; p less than 0.001).
Indication 6: AML with Inqovi (decitabine/cedazuridine) — May 2026 As covered in our recent post on the Inqovi plus venetoclax approval, this May 13, 2026 approval created the first all-oral HMA/BCL-2 combination, providing an alternative to the intravenous azacitidine plus venetoclax regimen.
Other indications (off-label uses with evidence)
Beyond its FDA-approved indications, venetoclax has substantial evidence and is widely used in clinical practice for:
- Relapsed or refractory multiple myeloma in patients with t(11;14) translocation
- Mantle cell lymphoma in combination with BTK inhibitors
- Various MDS regimens as covered in our Inqovi post
The CLL Disease Landscape: Who Uses Venetoclax and Why
Chronic lymphocytic leukemia is the most common leukemia in adults in Western countries, affecting approximately 200,000 Americans and resulting in 18,000 new diagnoses each year in the United States. It is a cancer of mature B lymphocytes that accumulates in the blood, bone marrow, and lymph nodes. Unlike many cancers, CLL often has an indolent course, with many patients living years without requiring treatment, but once treatment is needed, the disease is incurable without allogeneic stem cell transplantation.
For years, the standard for fit CLL patients was chemoimmunotherapy (FCR, fludarabine-cyclophosphamide-rituximab), and for unfit patients, chlorambucil-based combinations. The BCL-2 inhibitor and BTK inhibitor eras, beginning with ibrutinib in 2013 and venetoclax in 2016, fundamentally transformed the landscape. These targeted oral therapies achieved response rates and progression-free survival outcomes that surpassed decades of chemotherapy development, without the myelosuppression and infectious complications of chemotherapy regimens.
The February 2026 AMPLIFY-based approval of venetoclax plus acalabrutinib represents the current apex of this evolution: an all-oral, time-limited regimen that eliminates the need for intravenous infusions and offers fixed-duration treatment followed by a treatment-free interval, the first time that has been achievable in the first-line CLL setting without any IV component.
The AML Disease Landscape: The Population That Needed Venetoclax Most Urgently
The story of venetoclax in AML is inseparable from the demographics of the disease. Acute myeloid leukemia has a median diagnosis age of approximately 68 years, and for older adults with significant comorbidities, the only prior option was supportive care or low-intensity chemotherapy with response rates below 20% and median survival under 6 months.
The standard curative-intent treatment for AML, the “7+3” induction regimen of cytarabine and anthracycline, requires weeks of inpatient hospitalization and produces early mortality rates of 10 to 15% in older patients. For a 78-year-old with heart failure, the treatment could kill before the leukemia did.
The VIALE-A trial (venetoclax plus azacitidine versus azacitidine alone in elderly or comorbid AML) showed median overall survival of 14.7 months in the combination arm versus 9.6 months in the azacitidine-alone arm, with a composite complete remission rate of 66.4% versus 28.3%. For a population with no prior options offering anything close to these numbers, venetoclax-based therapy was transformative.
Safety: What Every Patient and Clinician Must Know
Boxed warning: Tumor lysis syndrome
The most serious risk with venetoclax is TLS, described in detail in the callout box above. Every patient initiating venetoclax must be assessed for TLS risk before starting, and the ramp-up dosing schedule must be followed precisely. Clinicians unfamiliar with venetoclax initiation should review the full prescribing information carefully before the first prescription.
TLS prophylaxis requirements:
- Hydration: begin 1 to 2 days before each ramp-up dose; continue at least 24 hours after each ramp-up dose
- Anti-hyperuricemic agent: allopurinol should be initiated 2 to 3 days before the first dose
- Electrolyte and renal function monitoring: before each ramp-up dose and at specific intervals after
Additional boxed warning: serious infections
Venetoclax can cause severe and fatal infections. Neutropenia is common, particularly with combination regimens. Grade 3 or 4 neutropenia occurs in approximately 50 to 60% of patients on venetoclax-based combinations. Monitor complete blood counts before each cycle and as clinically indicated.
Common serious adverse reactions
Neutropenia: Most common grade 3 or 4 toxicity. Granulocyte colony-stimulating factor (G-CSF) may be required. Dose interruption or reduction per prescribing information guidance.
Thrombocytopenia: Platelet count monitoring required before each cycle.
Anemia: Common across all indications and combination regimens.
Serious infections: Pneumonia, sepsis, and other serious infections have been reported. Monitor closely for febrile episodes.
Nausea and diarrhea: Most common non-hematologic adverse events; typically manageable with dose modification and supportive care.
Pregnancy
Venetoclax can cause fetal harm based on its mechanism of action. Females of reproductive potential should use effective contraception during treatment and for at least 30 days after the last dose.
The Generic Approval: What the Hatch-Waxman Pathway Means
The Dr. Reddy’s generic approval came through the Abbreviated New Drug Application (ANDA) pathway, the regulatory mechanism created by the Drug Price Competition and Patent Term Restoration Act of 1984 (Hatch-Waxman Act). Under this pathway, a generic applicant must demonstrate that its product is bioequivalent to the brand-name drug, meaning it produces the same drug concentration in the bloodstream over time, without repeating the extensive safety and efficacy clinical trials that established the drug’s value.
Dr. Reddy’s filed ANDA 214733 and challenged Venclexta’s patents with a Paragraph IV certification, asserting that the patents were invalid or not infringed. AbbVie and Genentech sued in the U.S. District Court for the District of Delaware in 2020 to block the generic, triggering the standard 30-month litigation stay. The litigation resolved, the last Venclexta regulatory exclusivity expired in 2026, and the FDA approved the generic on May 15, 2026.
This is the standard pathway through which generic competition enters the U.S. drug market for virtually every major small-molecule medication after patent and exclusivity expiration.
| What generic entry means for pricing: expectations and reality The pattern of price competition following first-generic entry for high-cost oncology drugs is well-established but often slower and less complete than patients hope for. For a drug like Venclexta with a monthly list price historically exceeding $10,000, the first-generic price typically enters at 15 to 30% below the brand list price. Meaningful price competition, 50% or more below brand list price, typically requires multiple generic manufacturers entering the market. For any given patient, the actual out-of-pocket cost depends not on the list price but on their specific insurance coverage, their pharmacy benefit manager’s formulary decisions, whether the generic or brand-name is preferred on their plan, and what assistance programs are available. AbbVie’s existing patient assistance programs for Venclexta and the generic manufacturer’s own pricing strategies will both affect real-world access. Patients currently on Venclexta with inadequate coverage should discuss the generic option with their oncologist and pharmacist as the first step to understanding whether switching to the generic reduces their out-of-pocket costs. |
|---|
What This Means for Patients Currently on Venclexta or Starting Venetoclax
For patients currently on Venclexta
In most states, a pharmacist can substitute a generic for a brand-name drug at the counter without calling the prescriber, as long as the generic has been rated therapeutically equivalent (AB-rated) by the FDA. If Dr. Reddy’s venetoclax receives an AB rating, your pharmacist may substitute it automatically when you fill or refill your prescription. The clinical effect will be identical: the same molecule, same doses, same therapeutic outcomes.
If you have concerns about the substitution, you or your prescriber can request “dispense as written” (DAW) on your prescription. However, for generic small-molecule drugs with established bioequivalence, there is no clinical reason to prefer the brand-name over the generic from a therapeutic perspective.
One practical note: Venetoclax has a complex titration schedule, particularly at initiation. If you have recently completed ramp-up and are at a stable maintenance dose, switching to the generic is straightforward. If you are mid-ramp-up, discuss the timing of any formulation switch with your oncologist to avoid any disruption to your dosing schedule.
For patients being newly prescribed venetoclax
Your pharmacist will likely dispense the generic by default, as it will typically be the lower-cost formulary-preferred option. You will receive the same drug at the same doses. The ramp-up schedule, TLS monitoring requirements, and safety monitoring parameters are identical for generic and brand-name venetoclax.
For related HED coverage of recent venetoclax approvals and the expanding landscape of venetoclax-based regimens, see our post on the Inqovi plus venetoclax approval creating the first all-oral AML regimen and our venetoclax coverage index for a full archive of related posts.
Sources
FDA generic approval: Venetoclax tablets 10 mg, 50 mg, 100 mg. ANDA 214733. Dr. Reddy’s Laboratories. Approved May 15, 2026. FDA.gov.
Drugs.com venetoclax drug information: Venetoclax: Uses, Dosage, Side Effects and Warnings. drugs.com.
AbbVie/Genentech Venclexta prescribing information: Venclexta (venetoclax) Prescribing Information. AbbVie Inc. and Genentech. Updated 2026.
Venetoclax plus acalabrutinib AMPLIFY trial approval: FDA Approves Combination Treatment of Venclexta and Acalabrutinib for Previously Untreated CLL. AbbVie/Genentech press release. February 20, 2026.
AMPLIFY trial (acalabrutinib-venetoclax): Pharmacy Times AMPLIFY coverage. pharmacytimes.com. February 2026.
VIALE-A trial (venetoclax + azacitidine AML): DiNardo CD, Jonas BA, Pullarkat V, et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. NEJM. 2020;383(7):617-629.
MURANO trial (venetoclax + rituximab CLL): Seymour JF, Kipps TJ, Eichhorst B, et al. Venetoclax-Rituximab in Relapsed or Refractory Chronic Lymphocytic Leukemia. NEJM. 2018;378(12):1107-1120.
CLL14 trial (venetoclax + obinutuzumab): Fischer K, Al-Sawaf O, Bahlo J, et al. Venetoclax and Obinutuzumab in Patients with CLL and Coexisting Conditions. NEJM. 2019;380(23):2225-2236.
FDA original venetoclax approval (2016): FDA approves venetoclax for CLL with 17p deletion. FDA.gov. April 2016.
BCL-2 inhibitor mechanism review: BCL-2 Inhibitors in Hematologic Malignancies. PMC8626879.
Apoptosis: Apoptosis. StatPearls. NCBI.
CLL overview: Chronic Lymphocytic Leukemia. American Cancer Society.
AML overview: Acute Myeloid Leukemia. American Cancer Society.
Hatch-Waxman Act and ANDA pathway: Abbreviated New Drug Application. FDA.gov.
Patent challenge history: Venclexta patent and exclusivity data. DrugPatentWatch.
Patient resources: Leukemia and Lymphoma Society: CLL | Leukemia and Lymphoma Society: AML | AbbVie Venclexta patient support | NCI CLL information | NCI AML information
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Venetoclax (generic or brand) carries a boxed warning for tumor lysis syndrome and requires specific ramp-up dosing with mandatory TLS risk assessment and monitoring. Initiation must be supervised by a qualified hematologist or oncologist. Patients currently on Venclexta should not make any changes to their regimen without guidance from their treating oncologist. |
|---|
Leave a Reply