| 📌 The essentials Xolair (omalizumab, Genentech/Novartis) is the most commercially significant drug losing U.S. exclusivity in 2026, with $3.7 billion in 2025 U.S. sales. It is a humanized anti-IgE monoclonal antibody approved for four indications: moderate-to-severe persistent allergic asthma (2003), chronic idiopathic urticaria (2014), chronic rhinosinusitis with nasal polyps (2020), and IgE-mediated food allergy (2024). The first U.S. biosimilar, Omlyclo (omalizumab-igec, Alvotech/Teva), was approved by the FDA in March 2025 with interchangeable designation, meaning pharmacists can substitute it for a Xolair prescription at the counter without contacting the prescriber. Commercial launch is expected by September 1, 2026 per a settlement agreement between Genentech/Roche and Alvotech/Teva. The access gap this LOE addresses: Xolair’s list price ranges from approximately $1,400 to $2,800 or more per dose, with annual costs of $20,000 to $35,000 or higher. The most common reason an eligible patient does not receive omalizumab is not clinical. It is the price. Biosimilar competition has the potential to change that. |
|---|
| 📚 About This Series: The 2026 Loss of Exclusivity Watch Each year, Health Evidence Digest tracks the drugs entering the competitive generic and biosimilar market, the moment when decades of brand-name exclusivity end and the healthcare system’s long wait for more affordable alternatives begins. In 2026, ten major drugs are losing U.S. exclusivity, representing a combined estimated $17 billion or more in annual sales. This is Post 1 of 10. The drugs in this series: Xolair (omalizumab) • Pomalyst (pomalidomide) • Opsumit (macitentan) • Januvia/Janumet (sitagliptin) • Simponi (golimumab) • Mavenclad (cladribine) • Gattex (teduglutide) • Trintellix (vortioxetine) • Briviact (brivaracetam) • Xeljanz (tofacitinib). Each post follows the same format: what the drug is and how it works, what the clinical evidence shows, who uses it and why, and what the entrance of competition means for patients, prescribers, and the market. |
|---|
For a drug that most people have never heard of, omalizumab has quietly become one of the most important medications in allergy and asthma medicine. Sold as Xolair by Genentech (a Roche subsidiary) and Novartis, it generated $3.7 billion in U.S. sales in 2025, making it the most commercially significant drug among the top 10 losing exclusivity in 2026. For the patients who take it, it can be life-changing. For the healthcare system, its arrival into a competitive biosimilar market is potentially a turning point for access to a class of treatment that has historically been gated behind high costs and strict eligibility criteria.
This post covers what omalizumab actually does, how it works at a molecular level, what two decades of clinical evidence say about its benefits and limitations, who it helps most, and what the entrance of biosimilar competition, including Omlyclo (omalizumab-igec), expected to launch by September 2026, is likely to mean for patients and prescribers.
What Omalizumab Is: A 20-Year Overview
Omalizumab was first approved by the FDA in 2003 for moderate-to-severe persistent allergic asthma in adults and adolescents, a time when biologics for asthma were essentially nonexistent. It was genuinely novel: the first anti-IgE monoclonal antibody, targeting the immunological root cause of allergic disease rather than just suppressing symptoms downstream.
Over the following two decades, its approved indications expanded substantially. Today, Xolair is approved in the U.S. for four distinct conditions:
| Indication | Population | Year approved | Administration |
|---|---|---|---|
| Moderate-to-severe persistent allergic asthma | Adults and adolescents 12 years and older; inadequately controlled by inhaled corticosteroids with perennial allergen sensitization | 2003 | Subcutaneous injection every 2 or 4 weeks |
| Chronic idiopathic urticaria (CIU/CSU) | Adults and adolescents 12 years and older with symptoms inadequately controlled by antihistamines | 2014 | Subcutaneous injection every 4 weeks |
| Chronic rhinosinusitis with nasal polyps (CRSwNP) | Adults 18 years and older inadequately controlled by nasal corticosteroids | 2020 | Subcutaneous injection every 2 or 4 weeks |
| IgE-mediated food allergy | Adults and children 1 year and older to reduce allergic reactions (not a cure; used alongside allergen avoidance) | 2024 | Subcutaneous injection every 2 or 4 weeks, weight/IgE-based dosing |
The food allergy indication, approved in February 2024, significantly expanded the potential patient population and generated substantial public attention. For the first time, families managing severe food allergies had access to an FDA-approved treatment that could reduce (though not eliminate) the risk of a serious reaction from accidental exposure. The approval was based on the OUtMATCH trial, which showed that after 16 to 20 weeks of treatment, 67% of omalizumab-treated participants could tolerate a 600 mg peanut protein dose without moderate-to-severe allergic symptoms, compared to 7% of placebo-treated participants.
The Science: How Anti-IgE Therapy Actually Works
To understand why omalizumab matters, it helps to understand IgE (immunoglobulin E), the antibody class at the center of allergic disease.
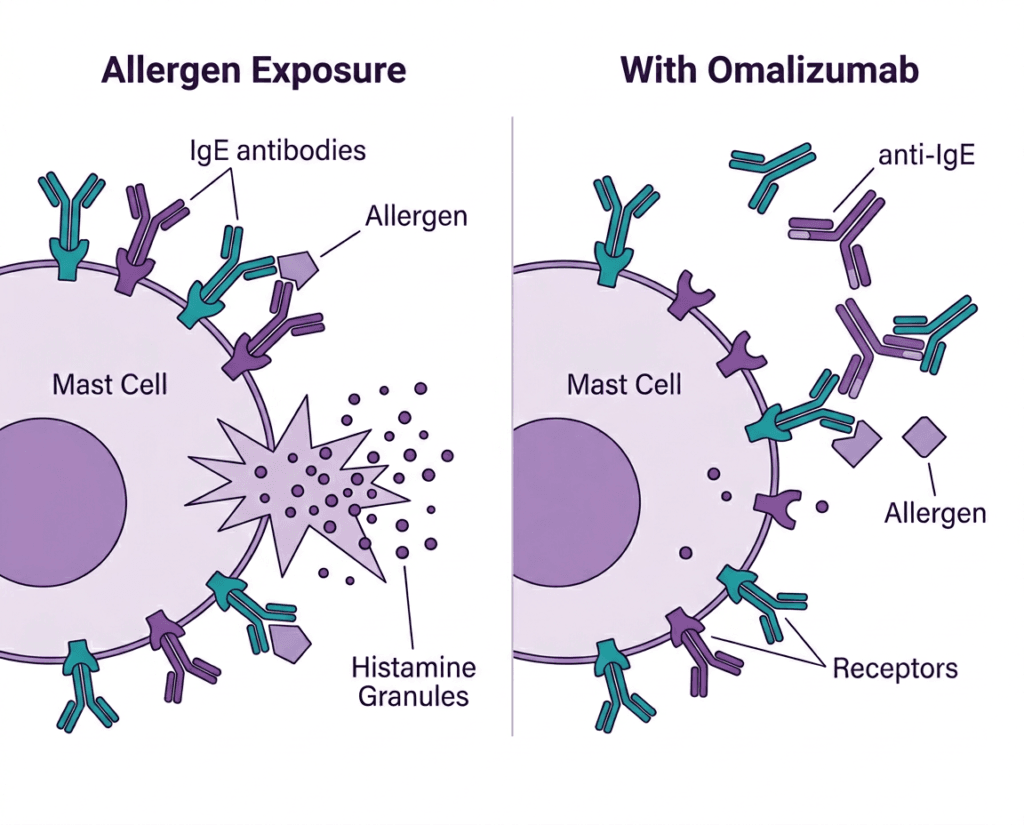
In allergic individuals, the immune system has become sensitized to specific environmental antigens: pollen, pet dander, dust mites, mold, certain foods. When exposed to these antigens, specialized immune cells called B cells produce IgE antibodies targeted against them. These IgE antibodies then bind to high-affinity receptors (FcεRI) on mast cells and basophils, white blood cells that patrol tissues and mucous membranes. The IgE sits there, primed.
When the sensitized person is re-exposed to the allergen, it binds to the IgE already docked on those cells, cross-linking adjacent IgE molecules. This cross-linking triggers the cell to degranulate, releasing a cascade of inflammatory mediators including histamine, leukotrienes, prostaglandins, and cytokines. The result is the classic allergic response: bronchoconstriction in asthma, urticaria wheals in hives, mucus hypersecretion in rhinosinusitis, and anaphylaxis in severe food allergy reactions.
| Where omalizumab intervenes in the allergic cascade Omalizumab is a humanized monoclonal antibody that binds specifically to the constant region (Cε3 domain) of free IgE in circulation, the IgE that is floating in the bloodstream before it can bind to mast cells and basophils. By capturing free IgE, omalizumab prevents it from loading onto the FcεRI receptors on mast cells. With fewer IgE-loaded receptors available, allergen exposure produces a much weaker degranulation response, or none at all. Over weeks and months of treatment, FcεRI receptor expression on mast cells and basophils also decreases, a downstream effect that further reduces the cellular machinery available for allergic responses. Critically, omalizumab does not block allergen-specific IgE that is already bound to mast cells. It only captures free circulating IgE. This is why dosing is based on the patient’s baseline total serum IgE level and body weight: higher IgE levels require higher doses to adequately capture the circulating IgE pool. |
|---|
Two Decades of Clinical Evidence: What It Shows and What It Does Not
Allergic asthma: the foundational indication
The clinical evidence base for omalizumab in moderate-to-severe allergic asthma is one of the most extensive in respiratory medicine. The pivotal trials and post-marketing studies have consistently shown:
| Outcome | Evidence | Clinical significance |
|---|---|---|
| Asthma exacerbation reduction | Approximately 25 to 50% reduction in exacerbation rates versus placebo in pivotal trials; sustained in long-term registry data | High: exacerbations drive hospitalizations, ER visits, and oral steroid burden |
| Corticosteroid sparing | Reduction in inhaled corticosteroid dose; reduced need for oral corticosteroid rescue | High: reduces steroid-related side effects including bone loss and metabolic effects |
| Quality of life (AQLQ scores) | Clinically meaningful improvements in validated asthma QoL scores across multiple trials | Moderate to high: patient-reported outcomes aligned with clinical endpoints |
| Exacerbation seasonality (PROSE study) | 47% reduction in fall exacerbations versus guideline-based care in low-income inner-city children | High: real-world evidence from the population historically least able to access the drug |
| Real-world effectiveness | PROSPERO registry and other post-marketing data confirm effectiveness broadly consistent with trial results over 5 or more years | Moderate: real-world data generally aligns with RCT findings |
The critical qualification in the allergic asthma data is eligibility: omalizumab only works in patients who have documented IgE-mediated allergic sensitization (positive skin test or RAST) to a perennial allergen. It does not work for non-allergic asthma, a meaningful subset of severe asthma patients. Patient selection, confirming allergic phenotype before initiating therapy, is essential and is required by the prescribing information.
Chronic idiopathic urticaria: the evidence is cleaner
For chronic idiopathic urticaria (CSU), the evidence base is particularly strong. The three pivotal GLACIAL, ASTERIA I, and ASTERIA II trials all demonstrated significant reductions in itch severity, hive activity, and overall disease burden compared to placebo, with 150 mg and 300 mg doses both showing benefit. The 300 mg dose is generally more effective.
What makes the CIU/CSU evidence distinctive is that it does not require IgE-mediated sensitization to a specific allergen. The mechanism in CIU/CSU is less fully understood but involves IgE’s role in mast cell activation through different pathways. Patients with CIU who have failed antihistamines have historically faced a frustrating situation with limited alternatives. Omalizumab changed that calculus.
Nasal polyps and food allergy: newer indications, growing evidence
The CRSwNP approval in 2020 was supported by the POLYP 1 and POLYP 2 trials showing meaningful reductions in nasal polyp score and nasal congestion severity versus placebo. The food allergy OUtMATCH data is discussed above. Both are real expansions of evidence, though the food allergy data in particular warrants honest framing: omalizumab does not desensitize patients or cure food allergy. It raises the threshold for a reaction, giving families more margin for accidental exposures. It is not a replacement for allergen avoidance, epinephrine auto-injectors, or allergen immunotherapy where appropriate.
Who Uses Xolair and Who Has Not Been Able To
The gap between who benefits from omalizumab and who actually receives it is significant, and that gap is almost entirely price-driven.
Eligible patients include: people with moderate-to-severe allergic asthma who have documented IgE sensitization and inadequate control on inhaled corticosteroids; patients with chronic hives unresponsive to antihistamines; adults with nasal polyps after nasal corticosteroid failure; and children as young as 1 year old with certain food allergies. This is a substantial patient population.
Xolair’s list price is approximately $1,400 to $2,800 or more per dose depending on the dose administered, with most patients receiving injections every 2 to 4 weeks. Annual costs can reach $20,000 to $35,000 or more. Genentech offers a patient support program, but access has remained limited for uninsured and underinsured patients, and prior authorization requirements have historically created barriers even for insured patients.
The most common reason an eligible patient does not receive omalizumab is not clinical. It is the price. This is the core public health significance of the 2026 loss of exclusivity: if biosimilar competition drives meaningful price reductions, the gap between who can benefit and who actually accesses treatment should narrow.
The Biosimilar Landscape: Omlyclo and What Comes Next
In March 2025, the FDA approved Omlyclo (omalizumab-igec), the first U.S. biosimilar to Xolair, developed by Alvotech and commercialized in the U.S. by Teva. The FDA also designated Omlyclo as an interchangeable biosimilar, the more valuable regulatory designation that allows pharmacists to substitute it for Xolair at the counter without a new prescription, subject to state pharmacy laws.
Omlyclo is approved for all four of Xolair’s indications and all dosing presentations. It is expected to enter the U.S. market by September 1, 2026 per a settlement agreement between Genentech/Roche and Alvotech/Teva.
| Product | Company | Status | Interchangeable? | Expected U.S. launch |
|---|---|---|---|---|
| Xolair (omalizumab) | Genentech / Novartis (Roche) | Reference product; approved 2003 | N/A | Available now |
| Omlyclo (omalizumab-igec) | Alvotech / Teva | FDA approved March 2025 | Yes, interchangeable designation | By September 1, 2026 |
| TEV-574 and other pipeline biosimilars | Multiple companies | In development/filing | TBD | 2026 to 2027 |
The interchangeable designation for Omlyclo is clinically and commercially significant. Unlike the majority of recently approved denosumab biosimilars, including Teva’s own PONLIMSI which did not receive interchangeable designation, Omlyclo can be automatically substituted at the pharmacy in most states. This is the mechanism that drives faster market conversion and stronger price competition.
| What interchangeability means at the pharmacy counter In the U.S., a biosimilar with an interchangeable designation can be substituted by a pharmacist for the reference product without calling the prescribing physician, provided state pharmacy law allows it, which most states do. This is the same standard that applies to generic small-molecule drugs, and it significantly reduces the friction of market conversion. A prescriber can always specify “brand medically necessary” to prevent substitution. But in routine practice, interchangeability allows formulary managers and pharmacists to automatically route patients to the lower-cost biosimilar as it enters the market, which is what drives meaningful price competition. For patients: if your insurer’s formulary adds Omlyclo as a preferred alternative, you may be automatically switched at your next fill unless your physician specifies otherwise. This is worth a brief conversation with your allergist or pulmonologist when the switch happens, not because biosimilars are less safe or effective, but to ensure the transition is coordinated and that your dose and administration schedule are clearly confirmed. |
|---|
What Patients Need to Know About the Transition
Is a biosimilar omalizumab as safe and effective as Xolair?
Yes. Biosimilar approval requires demonstration of no clinically meaningful differences in safety, purity, and potency compared to the reference product. The FDA’s biosimilar approval pathway includes analytical similarity data, pharmacokinetic/pharmacodynamic studies, and clinical data. For Omlyclo specifically, the FDA reviewed a comprehensive data package before granting both biosimilar and interchangeable designations, a higher regulatory bar than biosimilar approval alone.
The mechanism, the molecular target, and the clinical effects are identical. Patients should not expect any change in how the medication works.
Will the price actually go down, and by how much?
This is where honest uncertainty is warranted. The U.S. biosimilar market has not always delivered the dramatic price reductions seen in Europe, for structural reasons covered in our post on PONLIMSI and the denosumab biosimilar market. Xolair’s manufacturer has tools available, rebate arrangements with PBMs, patient assistance programs, and patient loyalty programs, that can complicate the competitive dynamics.
The interchangeable designation for Omlyclo is a meaningful advantage that most denosumab biosimilars lacked. And the omalizumab biosimilar market is at an earlier stage, meaning Omlyclo enters with a stronger competitive position as the sole biosimilar initially, before additional competitors arrive. The denosumab precedent showed first-mover biosimilars entering at 14 to 15% below reference list price. Whether omalizumab biosimilar pricing follows that pattern or goes deeper will depend on how many competitors enter and how aggressively PBMs and insurers push conversion. Patients should watch their formulary notifications and talk to their prescribers if they have concerns about a formulary switch.
What about patients on the food allergy indication?
Omlyclo is approved for the food allergy indication, same as Xolair. The 2024 food allergy approval specifically expanded access to children as young as 1 year old, a population for which omalizumab had not previously been approved for any indication. The dosing calculation based on body weight and total serum IgE level applies the same way for the biosimilar.
For families managing severe food allergies, a formulary switch to Omlyclo should not change the clinical management plan. The same dosing schedule, the same monitoring for injection-site reactions, and the same need for continued allergen avoidance and epinephrine auto-injectors as rescue medication all apply.
The Safety Profile: What Two Decades of Use Has Shown
With 20 years of post-marketing surveillance and millions of patients treated, omalizumab’s safety profile is unusually well-characterized for a biologic.
| Safety item | Details | Clinical guidance |
|---|---|---|
| Anaphylaxis | Rare but real: approximately 0.1 to 0.2% of patients in post-marketing surveillance. Most reactions occur within 2 hours of the first three injections. | All omalizumab injections must be given in a healthcare setting. Patients must be observed for at least 30 minutes after each of the first 3 injections and 30 minutes for subsequent injections. Prescribers should have anaphylaxis treatment available. |
| Injection site reactions | Most common adverse event: redness, warmth, pain at injection site. Typically mild and self-limiting. | Usually manageable with cold compress and rotating injection sites. |
| Malignancy (boxed warning) | FDA added a boxed warning in 2009 based on post-marketing data. The absolute risk increase is small and uncertain, and longer-term data has been reassuring, but the warning remains on the label. | Discuss with prescriber in patients with active or prior malignancy; clinical judgment required. |
| Parasitic infection susceptibility | IgE plays a role in defense against helminth infections. Theoretical risk, primarily seen in endemic areas. | Relevant for patients living in or traveling to regions with high helminth prevalence. |
| Churg-Strauss / EGPA | Cases of eosinophilic granulomatosis with polyangiitis reported in asthma patients on omalizumab. Causal relationship not established; may reflect unmasking as oral steroid dose is reduced. | Monitor for vasculitic symptoms including rash, worsening pulmonary symptoms, and peripheral neuropathy during steroid tapering. |
| Cardiovascular events | Post-marketing EXCELS study showed a small numerical increase in cardiovascular and cerebrovascular events in the omalizumab arm versus a comparison population, though not statistically significant. | Cardiovascular risk should be considered in individual patient assessment. |
What the Loss of Exclusivity Means for the Market
Xolair’s LOE is one of the most commercially consequential in 2026, not because of its current sales alone, but because of what access expansion could mean for underserved patient populations.
In severe allergic asthma, the patients most likely to benefit from anti-IgE therapy are disproportionately likely to be low-income and uninsured. Inner-city asthma, the disease burden concentrated in urban neighborhoods with poor air quality and high allergen exposure, is one of the strongest settings where omalizumab efficacy has been demonstrated. The PROSE study, one of the most important real-world omalizumab trials, was conducted specifically in low-income inner-city children: it showed a 47% reduction in fall exacerbations compared to guideline-based care. Those are exactly the patients who historically could not afford the drug.
If biosimilar competition drives Omlyclo’s net cost down meaningfully, even 20 to 30%, formulary access should broaden. More insurers and Medicaid programs are likely to add omalizumab to preferred formulary tiers. Prior authorization criteria may loosen. The public health downstream of genuine price competition in this market is real.
What This Means for Patients Right Now
If you are currently on Xolair and well-controlled, there is no clinical reason to change anything. What you should do is watch for formulary notifications from your insurer about transitions to Omlyclo when it launches in the second half of 2026. If a switch is planned, a brief check-in with your allergist or pulmonologist is worthwhile, not because the biosimilar is different, but because a care transition is always an opportunity to confirm your current dose and schedule are still appropriate.
If you have been told omalizumab might help you but could not access it because of cost, 2026 and 2027 may be the window where that changes. Biosimilar competition tends to improve formulary access before it dramatically reduces list prices. Ask your prescriber to revisit the conversation when Omlyclo is available.
For prescribers: the eligibility criteria have not changed. Documenting IgE sensitization and baseline total IgE is still required before initiating, and dosing is still based on the body weight/total IgE nomogram. The biosimilar approval does not alter the clinical eligibility framework. It only changes the pricing and access picture.
For related HED coverage on how biosimilar market entry actually works in practice and why regulatory approval does not automatically translate to patient savings, see our post on PONLIMSI and the denosumab biosimilar landscape and our post on Langlara and what interchangeable insulin biosimilar approvals mean for patient access.
Sources
Xolair FDA approval history: FDA Drug Approvals: Xolair (omalizumab). fda.gov.
Omlyclo FDA biosimilar approval, March 2025: FDA Biosimilar and Interchangeable Products. fda.gov.
LOE market context (Optum Rx): Blockbuster Drug Patent Expirations in 2026 and What They Mean. business.optum.com. April 29, 2026.
LOE market context (FDCELL): Top 10 Drugs Losing U.S. Patent Protection in 2026. fdcell.com. March 18, 2026.
OUtMATCH Trial (food allergy): Wood RA et al. Omalizumab for the Treatment of Multiple Food Allergies. New England Journal of Medicine. 2024;390:889–899. doi:10.1056/NEJMoa2312382.
PROSE Study (inner-city asthma): Teach SJ et al. Preseasonal treatment with either omalizumab or an inhaled corticosteroid boost to prevent fall asthma exacerbations. J Allergy Clin Immunol. 2015;136(6):1476–1485. PMID 26535077.
GLACIAL, ASTERIA I and II trials (CIU): Maurer M et al. Omalizumab for the treatment of chronic idiopathic or spontaneous urticaria. New England Journal of Medicine. 2013;368:924–935. doi:10.1056/NEJMoa1215372.
POLYP 1 and 2 trials (nasal polyps): Gevaert P et al. Omalizumab is effective in allergic and nonallergic patients with nasal polyps and asthma. J Allergy Clin Immunol. 2013;131:110–116.
Xolair prescribing information: Xolair (omalizumab) Prescribing Information. Genentech/Novartis. gene.com.
Xolair pricing reference: Xolair pricing. GoodRx. goodrx.com. Updated 2026.
Omalizumab StatPearls: Omalizumab. StatPearls. NCBI.
IgE biology: Immunoglobulin E. StatPearls. NCBI.
Mast cells and basophils: Mast Cells. StatPearls. NCBI.
Anaphylaxis: Anaphylaxis. StatPearls. NCBI.
Non-allergic asthma: Asthma. StatPearls. NCBI.
Chronic idiopathic urticaria: Chronic Urticaria. PMC4496130.
FDA biosimilar development: Biosimilar Development, Review, and Approval. FDA.gov.
Genentech patient support: Genentech Access Solutions: Xolair. genentech-access.com.
Patient resources: Asthma and Allergy Foundation of America | American Academy of Allergy, Asthma and Immunology: Find an Allergist | FARE: Food Allergy Research and Education
| Disclaimer: Health Evidence Digest provides general information about FDA approvals, loss of exclusivity events, and health research for educational purposes. This content is not a substitute for professional medical advice. Decisions about transitioning between omalizumab products, including Xolair and biosimilars, should be made in consultation with your prescribing allergist, pulmonologist, or other qualified clinician. Drug pricing information reflects figures at time of publication and is subject to change. |
|---|
Leave a Reply