
| 📌 The essentials On May 18, 2026, the FDA approved Baxfendy (baxdrostat, AstraZeneca) as the first and only aldosterone synthase inhibitor (ASI) for the treatment of hypertension. Baxfendy is the first drug in an entirely new pharmacological class to be approved for high blood pressure in decades. Indication: in combination with other antihypertensive drugs, to lower blood pressure in adults who are not adequately controlled on other agents. This is an add-on therapy, not a replacement for existing medications. Dosing: 2 mg orally once daily (recommended dose); 1 mg once daily for patients at increased risk of hyperkalemia or hyponatremia. Available: expected early June 2026. The clinical basis: Phase 3 BaxHTN trial (NCT06034743), published in the New England Journal of Medicine on August 30, 2025, enrolling 796 patients across 214 sites in 29 countries. Key result: placebo-adjusted systolic blood pressure reduction of 9.8 mmHg (2 mg dose) and 8.7 mmHg (1 mg dose) at 12 weeks (p less than 0.001 for both). Key safety warnings: hyperkalemia (elevated potassium) and hyponatremia (low sodium). Monitor electrolytes. Important caveat: the approval is based on blood pressure reduction as a surrogate endpoint, not on direct cardiovascular outcomes data. A cardiovascular outcomes trial is expected to follow. |
|---|
Hypertension affects an estimated 1.4 billion people worldwide and approximately 119 million adults in the United States. It is the single largest modifiable risk factor for stroke, myocardial infarction, heart failure, and chronic kidney disease. And yet, despite a treatment landscape that includes a dozen established drug classes and hundreds of individual medications, approximately 50% of patients on multiple antihypertensive treatments still do not have their blood pressure adequately controlled.
The patients in that 50% are not failing treatment through non-compliance alone. Many of them have a biological reason their blood pressure is hard to control, namely elevated or dysregulated aldosterone, a hormone that promotes sodium and water retention and raises blood pressure through mechanisms that existing drug classes do not directly address. Recognizing that aldosterone dysregulation is far more prevalent in difficult-to-control hypertension than previously understood is part of what makes Baxfendy’s approval a meaningful scientific development rather than just an incremental addition to a crowded market.
On May 18, 2026, the FDA approved Baxfendy (baxdrostat), the first aldosterone synthase inhibitor ever approved for hypertension. It targets the production of aldosterone itself, a mechanistic approach no approved drug has taken before in this indication.
What Aldosterone Is and Why Inhibiting Its Production Is a New Idea
To understand what makes Baxfendy mechanistically distinct, it helps to understand both what aldosterone does and why existing treatments have not addressed its overproduction directly.
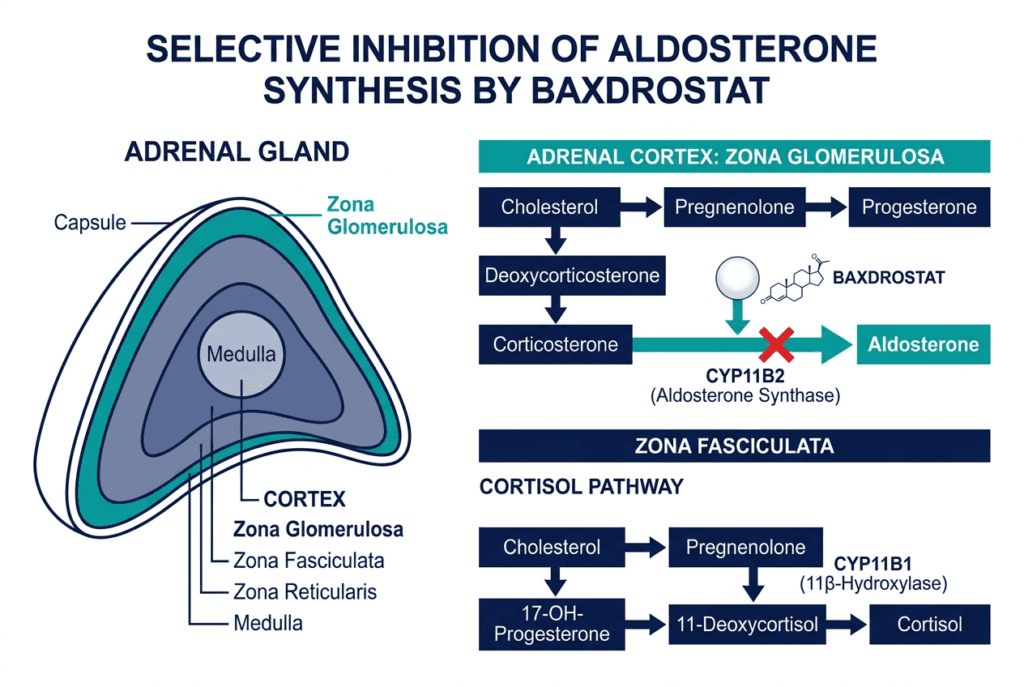
Aldosterone is a steroid hormone produced by the adrenal glands, specifically in a region called the zona glomerulosa. Its primary role is to regulate sodium and potassium balance in the kidneys. When aldosterone is elevated, the kidneys retain more sodium and water, increasing blood volume and raising blood pressure. Aldosterone also promotes potassium excretion, which is why elevated aldosterone is often associated with low potassium levels.
The enzyme responsible for producing aldosterone in the zona glomerulosa is called aldosterone synthase (CYP11B2). There is a closely related enzyme, cortisol synthase (CYP11B1), that makes cortisol in a neighboring region of the adrenal gland. Earlier attempts to develop aldosterone synthase inhibitors failed because they could not distinguish between CYP11B2 and CYP11B1 well enough: blocking both suppresses not only aldosterone but also cortisol, which is essential for the stress response and metabolic regulation. The side effects of cortisol suppression at therapeutic doses were unacceptable.
Baxdrostat is designed to solve this problem. It is described as a highly selective inhibitor of CYP11B2 that spares CYP11B1. In the BaxHTN trial, cortisol levels were monitored and remained stable, with no clinically meaningful cortisol suppression detected.
How existing drug classes compare mechanistically
Existing antihypertensive classes target aldosterone’s effects downstream rather than its production:
- ACE inhibitors and ARBs block the renin-angiotensin-aldosterone system (RAAS) at earlier steps, reducing angiotensin II signaling that drives aldosterone secretion. But in many patients, aldosterone eventually “escapes” this inhibition through angiotensin-independent pathways.
- Mineralocorticoid receptor antagonists (MRAs) like spironolactone and eplerenone block the aldosterone receptor in the kidney rather than reducing aldosterone itself. They are effective in resistant hypertension but carry a significant hyperkalemia risk, limiting their use in patients with chronic kidney disease.
- Diuretics reduce blood volume directly, addressing one consequence of aldosterone excess without reducing aldosterone levels.
Baxdrostat is the first approved drug to work at the top of this pathway, reducing aldosterone production in the adrenal gland before it reaches the circulation. Whether this upstream approach ultimately produces better clinical outcomes than MRAs in head-to-head comparison is not yet established by trial data.
The BaxHTN Trial: Design and Full Results
Trial design
The BaxHTN Phase 3 trial (NCT06034743) was a multinational, randomized, double-blind, placebo-controlled study conducted at 214 clinical sites across 29 countries. Results were presented at the European Society of Cardiology Congress 2025 in Madrid in August 2025 and simultaneously published in the New England Journal of Medicine.
Eligibility:
- Seated systolic blood pressure (SBP) of 140 mmHg or higher and less than 170 mmHg
- Receiving stable treatment with at least 2 antihypertensive medications of different classes, one of which was a diuretic (uncontrolled hypertension group), or at least 3 antihypertensive medications including a diuretic (resistant hypertension group)
- Estimated glomerular filtration rate (eGFR) of 45 mL/min/1.73m² or higher
- Serum potassium within acceptable range at baseline
Enrollment: 796 patients total across uncontrolled and resistant hypertension subgroups.
Design structure: After a placebo run-in period, the trial had four sequential phases: a 12-week double-blind, placebo-controlled period (the primary analysis period); a 12-week open-label extension; an 8-week randomized withdrawal period to assess persistence of effect; and a 20-week open-label safety assessment.
Primary endpoint results
| Outcome at 12 weeks | Baxdrostat 2 mg | Baxdrostat 1 mg | Placebo |
|---|---|---|---|
| Mean seated SBP reduction from baseline | 15.7 mmHg (95% CI 13.7 to 17.6) | 14.6 mmHg | Approximately 5.9 mmHg |
| Placebo-adjusted SBP reduction | 9.8 mmHg (95% CI 7.0 to 12.6) | 8.7 mmHg (95% CI 6.0 to 11.4) | Reference |
| p-value | p less than 0.001 | p less than 0.001 | — |
| Cortisol levels | No clinically meaningful change | No clinically meaningful change | — |
| Aldosterone reduction | Significant | Significant | No change |
Source: Efficacy and Safety of Baxdrostat in Uncontrolled and Resistant Hypertension. New England Journal of Medicine. Published August 30, 2025. doi:10.1056/NEJMoa2507109. BaxHTN NCT06034743.
The 9.8 mmHg placebo-adjusted SBP reduction at the 2 mg dose is clinically significant in context. Epidemiological data consistently show that a 10 mmHg reduction in systolic blood pressure is associated with approximately a 20% lower risk of serious cardiovascular events. In a population already on two or more antihypertensive medications, achieving nearly 10 mmHg additional reduction from one add-on pill is a meaningful result.
The randomized withdrawal period confirmed that blood pressure rose when baxdrostat was stopped and returned to target when it was reintroduced, confirming that the drug’s effect was causal rather than incidental.
The Bax24 trial: 24-hour ambulatory blood pressure
A separate Phase 3 study, Bax24 (NCT06168409), evaluated baxdrostat specifically in resistant hypertension using 24-hour ambulatory blood pressure monitoring (ABPM) rather than seated office measurements. Ambulatory blood pressure is considered a more reliable predictor of cardiovascular outcomes than clinic-based readings because it captures average pressure across the full daily cycle including nighttime.
Presented at the American Heart Association Scientific Sessions 2025 and published in The Lancet in March 2026, Bax24 showed a placebo-adjusted reduction of 14.0 mmHg in 24-hour average systolic blood pressure (p less than 0.0001) in patients with resistant hypertension. Nighttime systolic blood pressure was reduced by 13.9 mmHg (placebo-adjusted). Notably, 71% of baxdrostat-treated patients achieved a 24-hour average SBP below 130 mmHg compared with 17% of placebo-treated patients.
The Bax24 findings are not part of the current FDA approval label, but they are relevant context for understanding how comprehensively baxdrostat controls blood pressure across the full daily cycle in the most difficult-to-treat patients.
| The uncontrolled vs. resistant hypertension distinction The BaxHTN trial enrolled two overlapping but distinct populations. Uncontrolled hypertension is defined as blood pressure that remains above target despite the use of two antihypertensive medications. Resistant hypertension is a more stringent category: blood pressure that remains above target despite three antihypertensive agents including a diuretic, or that requires four or more agents to achieve control. Resistant hypertension is estimated to affect 10 to 15% of all hypertension patients and carries a substantially higher risk of end-organ damage, including left ventricular hypertrophy, kidney disease, and stroke. Both groups were included in BaxHTN because elevated aldosterone has been implicated in both, though the biological rationale is strongest in resistant hypertension where aldosterone escape from RAAS therapy is well-documented. |
|---|
Safety: What the Label Covers
Baxdrostat was generally well tolerated in the BaxHTN trial, with no unexpected safety findings reported. The most clinically significant warnings in the prescribing information are:
Hyperkalemia (elevated potassium): The most important class-related concern. Aldosterone promotes potassium excretion in the kidney. Inhibiting aldosterone synthesis reduces that excretion, which can raise serum potassium. The risk is greatest in patients with chronic kidney disease or those on other drugs that raise potassium, including ACE inhibitors, ARBs, MRAs, and potassium-sparing diuretics. The 1 mg starting dose is specifically recommended for patients at increased risk of hyperkalemia. Baseline and periodic electrolyte monitoring is essential.
Hyponatremia (low sodium): Less common than hyperkalemia but present in the trial data. Monitor sodium, particularly in older patients or those at risk for volume-related sodium shifts.
Adrenal function: Despite the selective mechanism, monitoring for signs of adrenal insufficiency is prudent in patients undergoing physiological stress such as illness or surgery, given the proximity of the drug’s mechanism to cortisol synthesis.
Common adverse events from the trial included headache, dizziness, and fatigue. Rates of these were generally comparable between baxdrostat and placebo.
Drug interactions to know: Because baxdrostat reduces aldosterone, its combination with MRAs (spironolactone, eplerenone, finerenone) produces additive aldosterone-lowering effects and substantially increases the risk of hyperkalemia. The prescribing information addresses this interaction specifically. Clinicians should review the full prescribing information before initiating.
What This Means for Patients and Clinicians
Who is this drug for?
Baxfendy is approved as add-on therapy for adults with hypertension that is not adequately controlled on other agents. The typical candidate based on the BaxHTN enrollment criteria is a patient who:
- Has systolic blood pressure of 140 mmHg or higher despite being on at least 2 established antihypertensive medications
- Is already taking a diuretic as part of their regimen
- Has adequate kidney function (eGFR of 45 or higher)
- Does not have a potassium level that contraindicates further aldosterone suppression
It is not approved as monotherapy or as initial hypertension treatment. Patients already well-controlled on existing medications have no indication to switch.
Who should discuss this with their cardiologist or hypertension specialist?
Patients with documented uncontrolled or resistant hypertension who have cycled through ACE inhibitors, ARBs, calcium channel blockers, and diuretics without achieving target blood pressure are the population this drug was designed for. The mechanism is specifically compelling for patients suspected to have elevated aldosterone as a driver, including those with primary aldosteronism or confirmed aldosterone excess, though the approval does not require this testing.
What is still unknown
The current FDA approval is based on blood pressure reduction as a surrogate endpoint, not on direct demonstration that baxdrostat reduces heart attacks, strokes, kidney disease progression, or death. In antihypertensive drug development, this is standard and accepted: the FDA has long approved blood pressure medications based on surrogate blood pressure endpoints given the overwhelming prior evidence that blood pressure reduction reduces cardiovascular events across drug classes.
That said, a cardiovascular outcomes trial is expected to follow. The results of that trial will be important for fully establishing Baxfendy’s place in the treatment hierarchy and for understanding whether aldosterone-specific lowering produces benefits beyond what is predicted by the blood pressure reduction alone. AstraZeneca has also announced trials in primary aldosteronism, chronic kidney disease with hypertension, and heart failure prevention, as well as a combination development program with dapagliflozin.
The Bigger Picture: A New Mechanism in a Disease That Has Needed One
Hypertension’s pharmacological armamentarium has not seen a genuinely new mechanism in a long time. Most drug classes currently prescribed for hypertension were developed between the 1950s and 1990s. Baxfendy’s approval is notable precisely because it represents a new biological angle on a very old problem.
The recognition that aldosterone dysregulation is far more prevalent in treatment-resistant hypertension than the classical primary aldosteronism diagnosis would suggest has been building in the cardiology literature for more than a decade. Studies using more sensitive aldosterone assays have found that a significant proportion of patients with resistant hypertension have inappropriately elevated aldosterone relative to their sodium and volume status, even without the discrete aldosterone-secreting adenomas that define classical primary aldosteronism. BaxHTN’s results are consistent with this evolving understanding: the magnitude of blood pressure reduction seen suggests that the drug is addressing a real and prevalent biological driver of difficult-to-control hypertension, not just an edge-case mechanism.
For patients whose blood pressure has resisted years of medication escalation, having a drug that works through a pathway none of their existing medications addresses is clinically meaningful, independent of where it eventually lands in outcome trials.
For related coverage of advances in cardiovascular and metabolic drug development, see our post on the first generic dapagliflozin, which covers the SGLT2 inhibitor class and its now-expanding role from blood sugar management to cardiovascular and kidney protection, and our post on Awiqli, the first once-weekly basal insulin for type 2 diabetes.
Sources
AstraZeneca FDA approval press release: BAXFENDY approved in the US as the first and only aldosterone synthase inhibitor treatment for adults with hypertension. AstraZeneca. May 18, 2026.
AstraZeneca US press release: FDA Approves Baxfendy (baxdrostat) as the First Aldosterone Synthase Inhibitor Treatment for Adults with Hypertension. businesswire.com. May 18, 2026.
BaxHTN primary NEJM publication: Efficacy and Safety of Baxdrostat in Uncontrolled and Resistant Hypertension. New England Journal of Medicine. August 30, 2025. doi:10.1056/NEJMoa2507109.
BaxHTN trial registration: NCT06034743. ClinicalTrials.gov.
Bax24 primary Lancet publication: Azizi M et al. Effect of baxdrostat on ambulatory blood pressure in patients with resistant hypertension (Bax24). The Lancet. 2026 Mar 7;407(10532):988-999.
Bax24 trial registration: NCT06168409. ClinicalTrials.gov.
BaxHTN Phase 3 design paper: Flack JM et al. Baxdrostat for uncontrolled and resistant hypertension: rationale and design of the Phase 3 clinical trials BaxHTN, BaxAsia, and Bax24. Hypertension Research. 2025. doi:10.1038/s41440-025-02297-7.
BioPharma Dive approval coverage: AstraZeneca wins US approval for Baxfendy hypertension drug. biopharmadive.com. May 18, 2026.
Cardiology Advisor approval coverage: Baxfendy Earns FDA Nod as First-in-Class Hypertension Treatment. thecardiologyadvisor.com. May 2026.
PharmExec coverage: FDA Approves Baxdrostat for Uncontrolled Hypertension in First-in-Class Entry. pharmexec.com. May 2026.
HCPLive approval coverage: FDA Approves Baxdrostat for Uncontrolled Hypertension on Background Therapy. hcplive.com. May 2026.
ESC Congress 2025 presentation: BaxHTN top-line data presented at ESC Congress 2025, Madrid, August 30, 2025.
AHA Scientific Sessions 2025 (Bax24): Bax24 Phase III trial full results presented at AHA Scientific Sessions 2025.
Drugs.com approval news: FDA Approves Baxfendy (baxdrostat) as the First Aldosterone Synthase Inhibitor Treatment for Adults with Hypertension. drugs.com. May 18, 2026.
Aldosterone biology: Aldosterone. StatPearls. NCBI.
Aldosterone synthase selectivity: CYP11B2 and CYP11B1 selectivity in aldosterone synthase inhibitors. PMC6116014.
ACE inhibitors and ARBs: ACE Inhibitors. StatPearls. NCBI.
MRAs in hypertension: Mineralocorticoid Receptor Antagonists. StatPearls. NCBI.
Diuretics in hypertension: Diuretics. StatPearls. NCBI.
NHLBI hypertension overview: High Blood Pressure. National Heart, Lung, and Blood Institute.
Patient resources: American Heart Association: High Blood Pressure | National Hypertension Control Initiative | AstraZeneca Baxfendy information
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Baxfendy is approved as add-on therapy and should only be initiated and monitored by a qualified healthcare provider. Blood pressure management requires individualized care; do not stop or change antihypertensive medications without consulting your prescriber. |
|---|
Leave a Reply