| 📌 The essentials On May 22, 2026, the FDA approved Hepcludex (bulevirtide-gmod, Gilead Sciences), making it the first and only FDA-approved treatment for chronic hepatitis delta virus (HDV) infection in the United States. HDV has had no approved pharmacologic therapy in the United States for the entire history of its recognition as a disease. Indication: adults with chronic HDV infection without cirrhosis or with compensated cirrhosis. Regulatory pathway: accelerated approval based on a decrease in HDV RNA and alanine aminotransferase (ALT) normalization. Continued approval may be contingent on verification of clinical benefit in a confirmatory trial. Regulatory designations: Breakthrough Therapy Designation, Orphan Drug Designation, Priority Review. The clinical basis: Phase 3 MYR301 trial (NCT03852719), 150 patients with chronic HDV infection, published in the New England Journal of Medicine. Primary endpoint at week 48: combined response rate of 48% with bulevirtide 8.5 mg versus 2% with delayed treatment. Through 144 weeks: undetectable HDV RNA in 50% of treated patients. No treatment resistance detected through the full 144-week treatment period. Critical safety warning: a boxed warning for severe acute exacerbations of hepatitis B and HDV after discontinuation. Do not stop Hepcludex without medical supervision. Dosing: 8.5 mg subcutaneous injection once daily. European status: bulevirtide 2 mg was approved in the European Economic Area in 2020; the 8.5 mg dose used in the U.S. approval was the dose studied in MYR301’s pivotal arm. |
|---|
Hepatitis delta virus is the rarest and most severe of the five major viral hepatitis types. It can only infect people who also have hepatitis B, because it is a satellite virus that needs the hepatitis B surface antigen to enter liver cells. In people with this coinfection, liver disease progresses faster, cirrhosis develops earlier, and the risks of liver cancer and liver-related death are substantially higher than with hepatitis B alone.
Despite this severity, and despite HDV being recognized for decades, there has never been an FDA-approved treatment for it in the United States. Clinicians have managed it with off-label, interferon-based regimens that are effective in a minority of patients, carry significant toxicity, and are not suitable for many patients with advanced liver disease.
That changed on May 22, 2026, when the FDA approved Hepcludex (bulevirtide-gmod) as the first approved treatment for chronic HDV in the United States. It is a first-in-class entry inhibitor that works through a mechanism unlike anything previously approved for viral hepatitis, and its approval is the culmination of a Phase 3 trial program that has generated eight years of clinical data across multiple dose levels and treatment durations.
What Hepatitis Delta Is and Why It Has Been So Hard to Treat
The biology of HDV and its relationship to HBV
Hepatitis delta virus (HDV) is a defective RNA virus discovered in 1977 by Mario Rizzetto in Italy. It is classified as a satellite virus: it cannot replicate independently. To enter hepatocytes (liver cells), it requires the hepatitis B surface antigen (HBsAg), which sits on the outer envelope of hepatitis B virus (HBV) particles and is also expressed on HDV virions. Without HBsAg, HDV cannot infect new cells.
This dependency means HDV only infects people who are already HBV-infected, either as a co-infection at the same time as HBV or as a superinfection in a person already chronically infected with HBV. Superinfection is the more clinically dangerous scenario: a person with chronic HBV who becomes superinfected with HDV typically develops accelerated liver disease.
The HDV genome encodes only one protein: the delta antigen (HDAg), in small and large isoforms. The small form promotes viral RNA replication; the large form suppresses replication and is required for virion assembly. This minimal genome is why HDV replicates so efficiently inside HBV-infected cells without needing to encode its own machinery.
The clinical consequence of HDV coinfection
In patients with chronic HBV/HDV coinfection, the presence of HDV dramatically accelerates liver injury. Compared to HBV monoinfection:
- Cirrhosis develops significantly faster, with some studies showing the median time to cirrhosis cut by half or more
- Hepatocellular carcinoma (HCC) occurs at 2 to 3 times the rate
- Liver-related mortality is substantially higher
- The risk of developing end-stage liver disease requiring transplantation is elevated
Chronic HDV infection is now recognized as the most severe form of viral hepatitis, carrying a worse prognosis than hepatitis B, C, or other viral types.
| How many people are affected and why it is underrecognized Global prevalence estimates for chronic HDV infection range from 12 million to 72 million people worldwide, reflecting genuine uncertainty in epidemiological data because HDV testing is inconsistently performed. In the United States, estimates suggest approximately 100,000 people are living with chronic HDV infection, though the true number is likely higher because HDV testing is not routinely performed in all HBV-infected patients. HDV disproportionately affects people who inject drugs (where percutaneous transmission is efficient), immigrants from regions with high HBV/HDV endemicity (Mongolia, West Africa, Eastern Europe, the Amazon basin), and people in populations with high HBV prevalence. The gap between actual prevalence and diagnosed cases reflects both under-testing and the relative rarity of the condition in clinical training curricula. Many HBV patients are never tested for HDV despite guidelines recommending HDV testing in high-risk individuals. |
|---|
How Bulevirtide Works: The Entry Inhibitor Mechanism
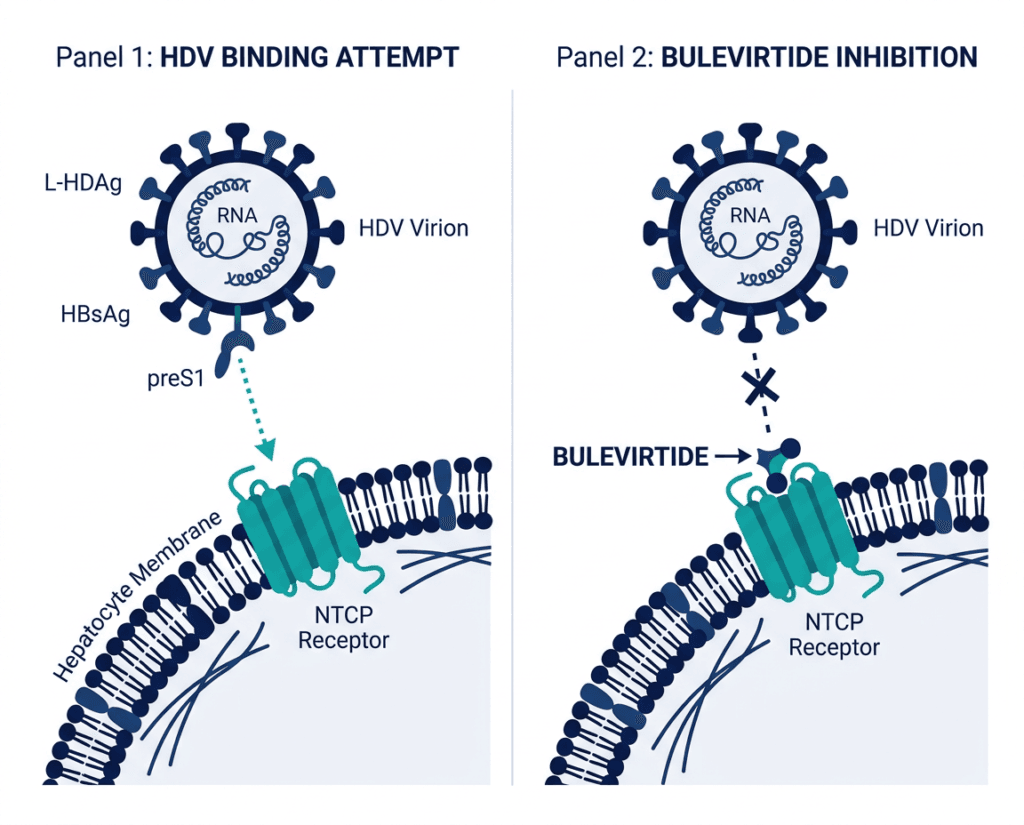
Bulevirtide is a first-in-class viral entry inhibitor. No previously approved hepatitis drug has worked through this mechanism. Understanding it requires understanding how HBV and HDV enter liver cells.
Both HBV and HDV use the same receptor to enter hepatocytes: sodium taurocholate cotransporting polypeptide (NTCP), a bile acid transporter expressed on the surface of liver cells. The viral entry process begins when a region of the HBV pre-S1 domain on the outer envelope of the virus binds to NTCP with high affinity. This binding triggers the virus to be taken up into the hepatocyte.
Bulevirtide is a myristoylated synthetic peptide, meaning it is a short chain of amino acids with a fatty acid (myristic acid) attached that anchors the molecule in cell membranes. Its amino acid sequence mimics the pre-S1 region that HBV and HDV use to bind NTCP. By competing with the virus for NTCP binding, bulevirtide prevents both HBV and HDV from entering hepatocytes, reducing the number of infected cells over time.
This is a mechanistically rational and highly targeted approach. It does not work inside the cell on the viral replication machinery, like nucleoside analogs for HBV. It works outside the cell, at the entry step, blocking new infection events. As old infected hepatocytes naturally die and are replaced, and as new cells are protected from infection, the proportion of HDV-infected hepatocytes in the liver declines.
The important implication: bulevirtide must be taken daily on a long-term basis, because stopping the drug removes the competitive blockade of NTCP, allowing HDV and HBV to resume infecting new hepatocytes. This pharmacological characteristic directly explains the boxed warning for severe exacerbation after discontinuation.
The MYR301 Trial: Design and Full Results
Design
MYR301 (NCT03852719) is a multicenter, randomized, open-label, parallel-arm Phase 3 trial evaluating the long-term efficacy and safety of bulevirtide in adults with chronic HDV. The trial enrolled 150 patients who were randomized 1:1:1 to three arms:
- Bulevirtide 2 mg once daily for 144 weeks (n=49)
- Bulevirtide 10 mg once daily for 144 weeks, which is approximately equivalent to the 8.5 mg U.S. approved dose (n=50)
- Delayed treatment: 48-week observational period (no antiviral treatment for HDV) followed by bulevirtide 10 mg once daily for 96 weeks (n=51)
The delayed treatment arm served as the control for the primary endpoint analysis. After 48 weeks, all delayed-treatment patients crossed over to receive bulevirtide. This design was used because withholding all treatment for 144 weeks in a condition as severe as HDV was not considered ethically appropriate.
The trial has continued through a 96-week off-treatment follow-up period, generating the longest dataset available for any HDV therapeutic program.
Primary endpoint: week 48 combined response
The primary efficacy endpoint was combined response at week 48, defined as both:
- Undetectable HDV RNA OR a decline in HDV RNA of 2 log10 IU/mL or greater from baseline, AND
- Normalization of alanine aminotransferase (ALT)
| Outcome at Week 48 | Bulevirtide (10 mg arm) | Delayed treatment (control) |
|---|---|---|
| Combined response rate | 48% | 2% |
| Undetectable HDV RNA | 20% | 0% |
| ALT normalization | Included in combined response | Minimal improvement |
| Statistical significance | p less than 0.001 | Reference |
The 46-percentage-point difference between the active treatment arm (48%) and the delayed treatment arm (2%) is the formal basis for the accelerated approval. The 2% rate in the delayed treatment arm is a direct reflection of HDV’s natural history: without treatment, spontaneous virologic suppression in chronic HDV is extremely rare.
Deepening response over time: through 144 weeks
One of the most clinically informative aspects of MYR301 is its long-term follow-up data, which was available to the FDA as part of the approval package.
| Virologic response over time | Bulevirtide (immediate treatment arm) |
|---|---|
| Undetectable HDV RNA at Week 48 | 20% |
| Undetectable HDV RNA at Week 96 | 36% |
| Undetectable HDV RNA at Week 144 | 50% |
| Combined response at Week 96 | Improved from Week 48 |
| Treatment resistance detected | None through 144 weeks |
| Patients with suboptimal early response at Week 24 who achieved virologic response by Week 96 | 43% of non-responders; 82% of partial responders |
Source: Journal of Hepatology 2024. doi:10.1016/j.jhep.2024.05.021. Gilead press release. May 2025.
The trajectory from 20% undetectable at week 48 to 50% undetectable at week 144 is the central efficacy message of the long-term MYR301 data. Patients who continue on bulevirtide are increasingly likely to achieve complete virologic suppression over time. This deepening response is consistent with the mechanism: as more cycles of hepatocyte replacement occur under entry inhibition, the proportion of infected cells progressively declines.
The absence of treatment resistance through 144 weeks is a notable finding. In HIV and HBV medicine, selection for resistance mutations under antiviral pressure is a persistent challenge. Bulevirtide’s mechanism as a host-targeting entry inhibitor rather than a direct-acting antiviral targeting viral enzymes may contribute to the absence of resistance.
Off-treatment durability
Final data from MYR301, presented in 2025, showed that 90% of patients who had achieved undetectable HDV RNA at the end of treatment (144 weeks) remained undetectable for nearly two years off treatment. This durability after stopping therapy is an important finding for patients who want to understand what long-term treatment success might look like.
| Why combined response (virologic plus biochemical) is the right endpoint for HDV In chronic viral hepatitis, virologic suppression alone does not capture the full clinical picture. ALT normalization reflects reduction in active liver inflammation: elevated ALT indicates ongoing hepatocyte injury, and its normalization suggests that the liver injury driven by active HDV replication is being controlled. The FDA required both components in the primary endpoint because treatment with HDV antivirals can suppress viral replication (virologic response) without fully resolving the inflammatory liver injury (biochemical response), and the combination captures both dimensions of disease activity that matter for long-term liver health. This is why the 48% combined response rate, rather than just the virologic response rate, is the appropriate headline number from MYR301. |
|---|
Safety: What the Prescribing Information Covers
Boxed warning: severe acute exacerbations after discontinuation
Hepcludex carries a boxed warning for severe acute exacerbations of hepatitis B and HDV after stopping treatment. When bulevirtide is discontinued, NTCP receptors that were competitively blocked by the drug become available again, allowing HBV and HDV to rapidly resume infecting hepatocytes. In some patients, this viral rebound produces a sudden, severe flare of hepatitis that can be clinically dangerous.
This warning has direct clinical implications for prescribers and patients:
- Do not stop Hepcludex without discussing a discontinuation plan with your hepatologist
- If discontinuation is necessary (surgery, tolerability issue, non-adherence), patients require close monitoring of liver function tests and HDV RNA for a minimum of 24 weeks after stopping
- Patients should be counseled about this risk before starting treatment to ensure informed decision-making about the long-term nature of therapy
Serious adverse reactions
- Hypersensitivity reactions including anaphylaxis: Reported with bulevirtide. Monitor for signs of allergic reaction after each injection, especially during the initial treatment period.
- Bile acid transporter inhibition: Because bulevirtide blocks NTCP, which is a bile acid transporter in addition to being the HBV/HDV entry receptor, it elevates circulating bile acid concentrations in the blood. This is a pharmacological consequence of the mechanism. In MYR301, elevated bile acids were observed and were generally asymptomatic, but the clinical implications of chronic NTCP inhibition with respect to bile acid metabolism are monitored as part of the drug’s safety profile.
Common adverse reactions
The most commonly reported adverse reactions in MYR301 were headache, abdominal pain, fatigue, pruritus (itching), and injection site reactions. Adverse events were mostly mild in severity, with no serious adverse events related to bulevirtide reported through 96 weeks of treatment.
Dosing and Administration
Approved dose: 8.5 mg as a subcutaneous injection once daily.
Administration: The drug is supplied as a lyophilized powder for injection. After reconstitution, the solution is administered as a subcutaneous injection. Patients can be trained to self-inject.
Duration: MYR301 treated patients for up to 144 weeks. The approved label does not specify a fixed treatment duration, consistent with the evolving evidence on long-term response and the expectation that patients who respond well may continue treatment.
Timing relative to other medications: Because bulevirtide blocks NTCP, it should not be taken simultaneously with medications that depend on NTCP for their hepatic uptake. Notable interactions include teriflunomide and some statins. Review the full prescribing information for the complete drug interaction list before prescribing.
HBV management: Most patients with HDV are also being managed for HBV with oral antivirals (entecavir, tenofovir). HBV suppression therapy is typically continued alongside bulevirtide; bulevirtide does not replace HBV antiviral management.
The Regulatory Journey: Why This Took So Long and What Changed
Bulevirtide has been in development for nearly a decade. It received European Medicines Agency approval for 2 mg use in the European Economic Area in July 2020, making it available to European patients more than five years before U.S. approval. The delay in U.S. approval reflected the FDA’s requirement for robust Phase 3 controlled data from a U.S.-eligible trial, which MYR301 was designed to provide.
The drug received multiple FDA designations recognizing the seriousness of HDV and the absence of alternatives:
- Breakthrough Therapy Designation: reserved for drugs showing substantial improvement over available therapy in a serious condition
- Orphan Drug Designation: recognizing HDV as a rare condition affecting fewer than 200,000 Americans
- Priority Review: 6-month review clock rather than the standard 10 to 12 months
The accelerated approval was granted on the basis that combined virologic and biochemical response is reasonably likely to predict long-term clinical benefit, specifically a reduction in the risk of cirrhosis, liver failure, and hepatocellular carcinoma. Confirmation of that clinical benefit in a dedicated outcomes trial is required as a post-marketing commitment.
What This Means for Patients With Chronic HDV Infection
For patients currently diagnosed with HDV
Hepcludex is now available in the United States for adults with chronic HDV infection without cirrhosis or with compensated cirrhosis. If you have been diagnosed with chronic HDV coinfection, this is the first FDA-approved therapy you can discuss with your hepatologist.
The most important questions to raise with your provider:
- Is my cirrhosis status (absent, compensated, or decompensated) consistent with the approved indication?
- What is my current HBV management regimen, and how will it interact with bulevirtide?
- What is my baseline HDV RNA and ALT level, which will serve as the reference point for monitoring treatment response?
- What is the monitoring schedule for HDV RNA, ALT, and bile acid levels during treatment?
- What is the plan if I need to stop treatment for any reason?
For patients who have not yet been tested for HDV
If you have chronic hepatitis B and have never been tested for HDV, and you fall into any of the higher-risk groups for HDV exposure (history of injection drug use, immigration from or travel to a high-prevalence region, or sexual contact with someone who has HDV), ask your hepatologist or primary care provider about HDV testing. The test is straightforward: an HDV antibody test initially, followed by HDV RNA if the antibody is positive.
The American Association for the Study of Liver Diseases (AASLD) and the Infectious Diseases Society of America (IDSA) both recommend HDV testing in patients with chronic HBV and risk factors for HDV exposure. Many patients with HDV are currently undiagnosed.
Patient support
Gilead’s Support Path program provides resources to help patients and healthcare professionals navigate coverage and financial assistance for Hepcludex. The Hepatitis B Foundation and the American Liver Foundation both maintain patient-facing resources on viral hepatitis management including HDV. The Global Hepatitis Delta Partnership is an international patient advocacy organization specifically focused on HDV.
For related HED coverage of other liver disease treatment approvals in 2026, see our post on Lynavoy (linerixibat) for cholestatic pruritus in primary biliary cholangitis and our post on Tavneos (avacopan) and the serious liver injury warning that has put the FDA and Amgen at odds.
Sources
FDA press announcement: FDA Approves First Treatment for Chronic Hepatitis Delta Virus (HDV) Infection. FDA.gov. May 22, 2026.
Gilead Sciences press release: FDA Grants Accelerated Approval to Gilead’s Hepcludex (bulevirtide-gmod), the First and Only Approved Treatment for Chronic Hepatitis Delta Virus (HDV). businesswire.com. May 22, 2026.
Drugs.com approval news: FDA Grants Accelerated Approval to Hepcludex (bulevirtide-gmod) for Chronic Hepatitis Delta Virus (HDV). drugs.com. May 22, 2026.
MYR301 primary NEJM publication: Wedemeyer H et al. A Phase 3, Randomized Trial of Bulevirtide in Chronic Hepatitis D. New England Journal of Medicine. 2023;389:22-32. doi:10.1056/NEJMoa2213429.
MYR301 week 96 Journal of Hepatology publication: Wedemeyer H et al. Bulevirtide monotherapy in patients with chronic HDV: Efficacy and safety results through week 96 from a phase III randomized trial. J Hepatol. 2024. doi:10.1016/j.jhep.2024.05.021.
MYR301 final 144-week data (Gilead press release): Final Data From the Phase 3 MYR301 Study Demonstrated Longer Treatment With Bulevirtide Was Associated With Sustaining Undetectability. gilead.com. May 2025.
MYR301 trial registration: NCT03852719. ClinicalTrials.gov.
Pharmacy Times clinical review: FDA Approves Bulevirtide-gmod as First-Ever Treatment for Chronic Hepatitis Delta Virus Infection. pharmacytimes.com. May 2026.
HCPLive clinical coverage: Bulevirtide Receives Historic First FDA Approval for Chronic Hepatitis Delta. hcplive.com. May 2026.
Contagion Live approval summary: Bulevirtide Approved as First US Treatment for Chronic Hepatitis Delta Virus. contagionlive.com. May 2026.
EMA Hepcludex EPAR: Hepcludex: European Public Assessment Report. ema.europa.eu.
HDV biology overview: Hepatitis Delta Virus. StatPearls. NCBI.
Bulevirtide mechanism (NTCP): Sodium Taurocholate Cotransporting Polypeptide as a Drug Target. PMC9283099.
NIDDK hepatitis D overview: Hepatitis D. NIDDK.
FDA accelerated approval: Accelerated Approval Program. FDA.gov.
FDA breakthrough therapy: Breakthrough Therapy Designation. FDA.gov.
FDA orphan drug: Designating an Orphan Product. FDA.gov.
Hepcludex prescribing information: Hepcludex (bulevirtide-gmod) Prescribing Information. Gilead Sciences. 2026.
Patient resources: American Association for the Study of Liver Diseases | Hepatitis B Foundation | American Liver Foundation | Global Hepatitis Delta Partnership | Gilead Support Path Program
| Disclaimer: Health Evidence Digest provides general information about FDA approvals and health research for educational purposes. This content is not a substitute for professional medical advice, diagnosis, or treatment. Hepcludex received accelerated approval; continued approval may be contingent on confirmatory trial results. Do not start or stop Hepcludex without guidance from a qualified hepatologist. Treatment decisions for chronic HDV infection should be made in close consultation with a physician experienced in viral hepatitis management. |
|---|
Leave a Reply