
| 📌 What this article covers Semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) are being prescribed at rapidly increasing rates to women with PCOS, despite the fact that neither drug is FDA-approved for PCOS specifically. This article synthesizes what the peer-reviewed research as of 2026 shows about how GLP-1 medications affect ovulation, menstrual regularity, fertility, and pregnancy outcomes in women with PCOS. It also covers what current evidence does not show, because on this topic the gaps matter as much as the findings. This is not medical advice. If you have PCOS and are taking or considering a GLP-1 medication, the information here is a starting point for a conversation with your prescriber, not a substitute for one. |
|---|
Something has shifted in PCOS treatment over the past four years. GLP-1 receptor agonists, the class of medications that includes semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound), were originally developed for type 2 diabetes and then approved for chronic weight management. But prescribing data tells a different story about how they are actually being used. In women with PCOS, GLP-1 prescribing increased from roughly 2% of patients in 2021 to approximately 18% by 2025. That is nearly a tenfold increase, in a condition for which these drugs have no formal FDA approval.
The clinical logic is not hard to follow. PCOS is tightly linked to insulin resistance and excess weight, and GLP-1 medications address both. Many women with PCOS report improvements in their symptoms after starting these drugs. Some report spontaneous conception after years of struggling with ovulatory dysfunction. The popular media has described this as “Ozempic babies,” and the coverage has ranged from enthusiastic to alarming.
What does the peer-reviewed evidence actually show in 2026? The answer is more nuanced, and more honest about uncertainty, than most of what is circulating online.
What PCOS Is and Why Metabolism Matters So Much
Polycystic ovary syndrome affects an estimated 6 to 13% of reproductive-aged women worldwide, making it the most common endocrine disorder in this population. Despite its name, you do not need polycystic ovaries to have PCOS. The diagnosis is clinical, based on the Rotterdam criteria, which require at least two of three features: ovulatory dysfunction, clinical or biochemical signs of elevated androgens, and polycystic ovarian morphology on ultrasound.
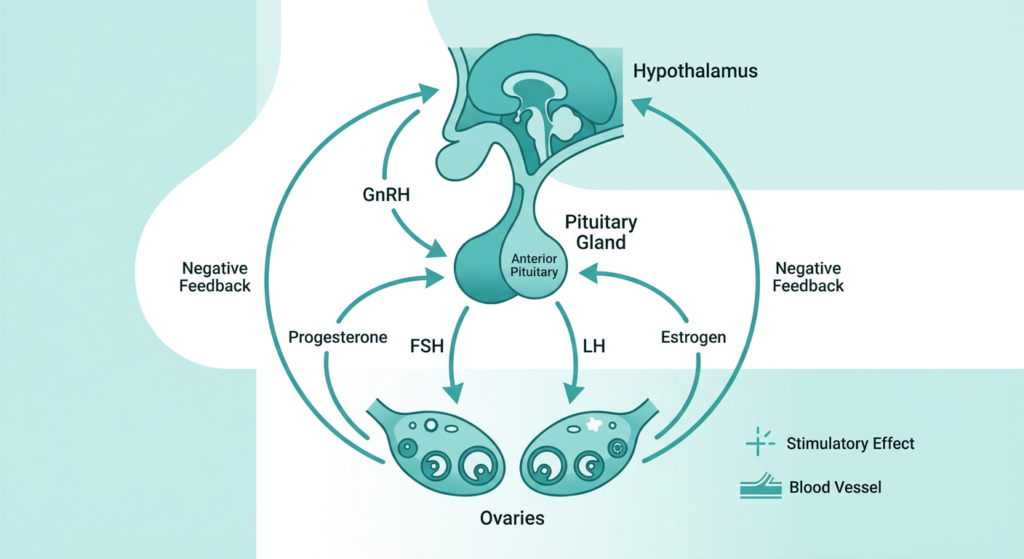
What defines PCOS at the metabolic level is a vicious cycle involving insulin resistance and androgen excess. Elevated insulin drives the ovaries to produce more androgens. Those androgens worsen insulin sensitivity. The resulting hyperinsulinemia suppresses sex hormone-binding globulin (SHBG), which increases free testosterone levels. The whole system feeds back on itself, and ovulation pays the price.
Between 40 and 90% of women with PCOS are overweight or obese, and insulin resistance is present even in roughly 60% of lean women with PCOS. This metabolic backdrop is why treatments that improve insulin sensitivity, including metformin, lifestyle modification, and now GLP-1 medications, have attracted so much interest for their potential reproductive benefits. The metabolic and reproductive problems in PCOS are not separate issues. They are the same issue, viewed from different angles.
If you are navigating a recent PCOS diagnosis, our resources page has links to clinical guidelines and patient advocacy organizations.
How GLP-1 Medications Work, and Why They Might Help in PCOS
GLP-1 (glucagon-like peptide-1) is a hormone naturally produced in the gut after eating. It signals the pancreas to release insulin in a glucose-dependent way, suppresses glucagon, slows gastric emptying, and reduces appetite through direct action on the brain. GLP-1 receptor agonists are synthetic versions of this hormone, engineered to last longer in the body than the natural peptide, which degrades within minutes.
The drugs most widely used in PCOS discussions are:
- Semaglutide (weekly injection: Ozempic for diabetes, Wegovy for weight management; daily oral: Rybelsus)
- Liraglutide (daily injection: Victoza for diabetes, Saxenda for weight management)
- Tirzepatide (weekly injection: Mounjaro for diabetes, Zepbound for weight management), which targets both GLP-1 and GIP receptors
The connection to PCOS is mechanistic. If GLP-1 medications reduce insulin resistance, lower circulating insulin, and promote weight loss, then the downstream hormonal environment in the ovary should improve. Reduced insulin means reduced ovarian androgen production. Reduced androgens mean higher SHBG, lower free testosterone, and potentially restored ovulatory function.
Beyond the indirect metabolic pathway, there is some evidence that GLP-1 receptors are expressed directly in reproductive tissues, including the pituitary, ovaries, and endometrium. This has raised the question of whether GLP-1 medications might have direct effects on follicular development and ovulation, independent of weight loss. The honest answer from the current evidence is: possibly, but we cannot separate this cleanly from the effects of metabolic improvement in human studies.
What the Research Shows: Ovulation and Menstrual Regularity
The clinical evidence for GLP-1 medications improving ovulatory function in PCOS is real, but it comes from studies that are mostly small, short, and conducted in women who were also losing weight and improving insulin sensitivity simultaneously.
A 2026 narrative review published in the Journal of Clinical Medicine by Abedi et al. synthesized 49 studies on GLP-1 receptor agonists and reproductive outcomes. The review found consistent signals across multiple study designs:
- GLP-1 medications improve menstrual regularity and ovulatory frequency in women with obesity and PCOS
- Several trials reported improvements in LH and progesterone profiles, reduced androgen levels, and increased SHBG
- One randomized trial that compared exenatide to metformin in women with PCOS reported spontaneous pregnancy rates of 43.6% with exenatide versus 18.7% with metformin after 12 weeks
That last number is striking enough to warrant a caveat. It comes from a single trial, in a selected population, with a 12-week window. It should not be extrapolated as a reliable estimate of what any given woman with PCOS can expect from a GLP-1 medication. What it tells us is that the fertility signal is real and worth taking seriously, not that the magnitude is established.
The review authors concluded that GLP-1 medications may improve ovulatory function and menstrual regularity in women with obesity and PCOS, but were careful to note that most of the observed reproductive benefit likely reflects metabolic normalization rather than direct drug action on the ovary. That distinction matters clinically, because it suggests that sustained metabolic improvement, not just the drug itself, is probably what drives the reproductive benefit.
A 2024 study published in Nature Communications by Sánchez-Garrido et al. tested GLP-1-based multi-agonist compounds, including a GLP-1/Estrogen conjugate and a GLP-1/GIP/Glucagon triple agonist, in two mouse models of PCOS. The GLP-1/Estrogen combination showed superior metabolic efficacy compared to any other multi-agonist or to metformin, and in one of the mouse models (the ovulatory PCOS model), also improved ovarian cyclicity without causing uterotrophic effects. This is preclinical research and cannot be directly applied to human treatment, but it provides mechanistic support for the idea that GLP-1-based combinations may have effects on PCOS-related ovarian dysfunction beyond what either component achieves alone. Next-generation multi-agonist compounds are likely to reach clinical trials in PCOS populations in the coming years.
The RESTORE Trial: The Human Evidence We Have Been Waiting For
The most important ongoing clinical trial in this space is RESTORE (NCT05662098), a randomized controlled trial actively enrolling women aged 12 to 35 with PCOS and obesity. RESTORE is directly testing whether semaglutide improves reproductive and metabolic outcomes in PCOS in a rigorous, prospective design. Primary endpoints include ovulatory frequency, hormonal parameters, and metabolic markers. The trial is expected to generate data that will meaningfully advance the field beyond the observational and small interventional studies that currently form the evidence base.
Until RESTORE reports, the clinical case for GLP-1 medications in PCOS rests on mechanistic plausibility, indirect trial data, and a growing body of real-world experience. That is a reasonable basis for individualized clinical decision-making with an informed prescriber. It is not yet a basis for definitive guidelines.
The Fertility Paradox: Restored Ovulation and Unintended Pregnancy
Here is where the clinical picture becomes more complicated, and where the evidence carries a warning that is underrepresented in popular coverage.
If GLP-1 medications restore ovulatory function in women with PCOS who previously had irregular or absent ovulation, those women become fertile in ways they may not have been before. If they are sexually active and not using reliable contraception, unintended pregnancy becomes a real possibility.
The Abedi et al. review notes that this creates what they describe as a clinical paradox: the same drug that offers reproductive benefit can also increase the risk of conception at a time when the drug itself is still in the body, and when current guidance recommends discontinuing GLP-1 medications before pregnancy.
This is not a theoretical concern. Prescribing data from Australia documented a rapid rise in GLP-1 prescribing in reproductive-aged women, with increasing overlap between GLP-1 initiation and contraceptive use patterns. Real-world data from across multiple countries show that inadvertent pregnancy exposure is becoming more common.
A separate pharmacokinetic issue is relevant here specifically for semaglutide. Semaglutide has an elimination half-life of approximately one week, meaning the drug accumulates with weekly dosing and persists in the body for several weeks after the last dose. Current prescribing recommendations advise discontinuing semaglutide approximately two months before attempting conception to reduce drug exposure during early organogenesis, the critical developmental window of weeks three through eight of pregnancy, when organ formation occurs.
For tirzepatide, there is an additional concern that is specific to this drug: clinical guidance indicates that tirzepatide may reduce oral contraceptive exposure during treatment initiation and dose escalation, which could compromise contraceptive effectiveness. Women starting tirzepatide who rely on oral contraceptives should discuss backup contraception options with their prescriber.
The bottom line for women with PCOS who are on a GLP-1 medication and not trying to conceive: contraception planning needs to be part of this conversation. The Abedi et al. review found evidence that this counseling is not consistently being delivered in routine clinical practice.
What the Evidence Shows About Pregnancy Safety
This is the question most women want answered, and it is also the one where the evidence is most limited.
What we know
The available human data on GLP-1 medication exposure during pregnancy come from regulatory pharmacovigilance datasets, observational cohorts, national registries, and case reports. These are not randomized pregnancy trials, because those studies cannot ethically be conducted. The findings to date are cautiously reassuring but far too limited to be interpreted as evidence of safety.
Key findings from the Abedi et al. review include:
- An analysis of FDA and EMA regulatory data by Parker et al. identified 164 unplanned pregnancies among approximately 32,000 GLP-1-treated women. Outcomes included 43% live births, 22% spontaneous abortions, and 2.7% congenital anomalies, which were comparable to the placebo group in those datasets.
- A Danish cohort study of more than 104,000 pregnancies, including 32 with first-trimester semaglutide exposure, found no increase in major malformations.
- A Taiwanese cohort of women with pregestational type 2 diabetes found no increased risk of major congenital malformations after periconceptional GLP-1 exposure compared to insulin, though confounding by the underlying diagnosis remains a limitation.
- The InPreSS consortium evaluated more than 50,000 pregnancies in women with pregestational type 2 diabetes and found no increased risk of major congenital malformations after periconceptional GLP-1 exposure compared to insulin.
Collectively, these studies do not identify a consistent teratogenic signal. But the review authors are explicit that the absence of a clear teratogenic signal should not be interpreted as confirmation of safety. Sample sizes for the exposed groups are small. Confounding by the underlying conditions (diabetes, obesity) is difficult to fully adjust for. And early pregnancy losses may be incompletely captured.
What the animal studies show
Preclinical studies across rodent and rabbit models showed dose-dependent reductions in fetal weight, delayed bone formation, and skeletal variants when GLP-1 medications were administered during pregnancy. Mechanistic studies with semaglutide specifically showed reductions in fetal and placental growth and downregulated placental nutrient transport systems in late-gestation models.
Importantly, many of these preclinical findings occurred alongside maternal weight loss and reduced food intake, making it difficult to attribute the fetal effects specifically to the drug rather than to nutritional restriction. This is an important interpretive nuance that is often missing from both alarming and reassuring headlines.
One partial reassurance from the pharmacokinetic side: placental transfer studies of large peptide GLP-1 medications (specifically dulaglutide) found very low maternal-to-fetal transfer at term, approximately 0.2 to 0.7%, suggesting limited direct fetal exposure for some agents. But this does not eliminate concern, particularly early in pregnancy, and findings may differ across agents.
What to Ask Your Doctor: A Practical Guide
If you have PCOS and are currently taking or considering a GLP-1 medication, these are the questions worth bringing to your prescriber.
If you are not trying to conceive:
- Is my current contraceptive method reliable on this medication? (Relevant especially for oral contraceptives with tirzepatide)
- Do I understand that improved ovulation may increase my fertility even if I have had irregular periods?
- What is the plan if I become pregnant while on this medication?
If you are planning to conceive in the next year:
- How far in advance should I stop this medication before trying to conceive?
- What metabolic management plan will replace the medication after I stop, to prevent rebound weight gain and worsening insulin resistance?
- Are there clinical trials I would be eligible for, including RESTORE?
If you have had an unintended pregnancy while on a GLP-1 medication:
- The review by Abedi et al. recommends individualized assessment rather than reflexive reassurance or alarm. Multidisciplinary care involving endocrinology, obstetrics, and potentially maternal-fetal medicine is appropriate in this situation.
What Still Needs to Be Answered
The evidence gaps in this area are significant, and researchers are aware of them.
The most important outstanding questions include:
- Do GLP-1 medications have direct effects on follicular development and ovulation in women with PCOS, beyond what is explained by weight loss and improved insulin sensitivity?
- What are the pregnancy outcomes specifically in women with PCOS (as opposed to women with type 2 diabetes) who are exposed to these drugs periconceptionally?
- How should these medications be sequenced and discontinued in women planning pregnancy, particularly given the weight rebound that often follows discontinuation?
- What are the reproductive safety profiles of tirzepatide and newer dual and triple agonists specifically, since most of the existing data focuses on semaglutide and liraglutide?
Large prospective pregnancy registries with standardized definitions and outcomes are the path forward. The field needs them urgently, because real-world exposure is already far ahead of the evidence base.
The Broader Context: GLP-1s and Women’s Health in 2026
The rapid expansion of GLP-1 prescribing into PCOS and women’s reproductive health is part of a broader pattern of these medications crossing into conditions they were not originally developed for. That pattern is not inherently problematic. Metformin followed a similar path in PCOS, and the evidence eventually caught up. But the pace of prescribing in PCOS has outrun the evidence in ways that make careful clinical counseling essential.
The evidence supports cautious optimism about GLP-1 medications for metabolic and reproductive improvement in women with PCOS. It also supports genuine uncertainty about pregnancy safety. Both of those things are true simultaneously, and patients deserve to understand both.
For related coverage of how changing evidence is reshaping women’s health care, including the new 2026 cervical cancer screening guidelines that now allow self-collection for HPV testing, see our post here. For our earlier analysis of semaglutide in PCOS clinical trials, including a breakdown of the RESTORE trial design and what the research will need to show, see Ozempic for PCOS: Clinical Trials Are Testing It Right Now.
Sources
Primary narrative review: Abedi MM, Patni MM, Shajahan ANB, et al. GLP-1 Receptor Agonists, Fertility Restoration, and Reproductive Safety in Women of Reproductive Age: A Narrative Review. Journal of Clinical Medicine. 2026;15(9):3204. doi:10.3390/jcm15093204
Nature Communications multi-agonist study: Sánchez-Garrido MA, Serrano-López V, Ruiz-Pino F, et al. Superior metabolic improvement of polycystic ovary syndrome traits after GLP1-based multi-agonist therapy. Nature Communications. 2024;15:8498. doi:10.1038/s41467-024-52898-y
RESTORE trial registration: NCT05662098. ClinicalTrials.gov.
Danish semaglutide cohort: Kolding L, et al. Pregnancy outcomes after semaglutide exposure. Basic and Clinical Pharmacology and Toxicology. 2025;136:e70021.
Parker regulatory analysis: Parker CH, Slattery C, Brennan DJ, le Roux CW. GLP-1 receptor agonists’ use during pregnancy: Safety data from regulatory clinical trials. Diabetes, Obesity and Metabolism. 2025;27:4102-4108.
PCOS overview: National Institute of Child Health and Human Development. Polycystic Ovary Syndrome.
| Disclaimer: Health Evidence Digest provides general information about clinical research and health topics for educational purposes only. Nothing on this site constitutes medical advice, diagnosis, or treatment. GLP-1 medications (semaglutide, tirzepatide, liraglutide) are not FDA-approved for PCOS. Treatment decisions, contraception planning, and preconception counseling should be made in consultation with a licensed healthcare provider who can evaluate your individual health history. If you are pregnant or planning pregnancy while taking a GLP-1 medication, contact your prescriber promptly. |
|---|
Leave a Reply